By Matthew McKenzie – Cygnet PCREF Carer Lead & Carer Ambassador
Cygnet PCREF Carer Lead & Carer Ambassador
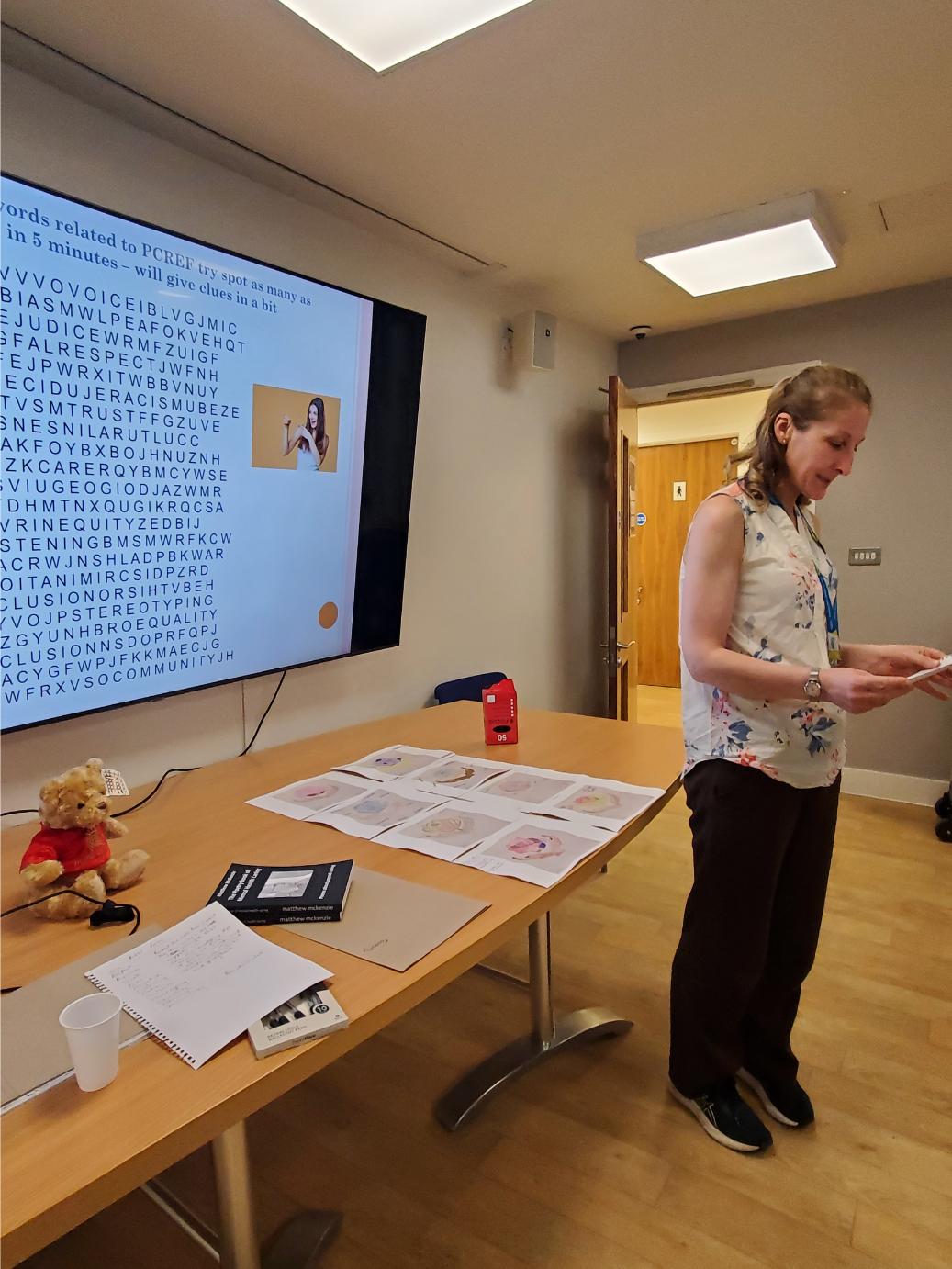
On 4 August 2026, unpaid carers, professionals and people with lived experience came together at Cygnet Churchill for the second Voices & Verses Carers Poetry Event. The purpose of the afternoon was not simply to read poetry, but to create a safe space where carers could express experiences that are often overlooked within mental health services.
The event formed part of Cygnet’s ongoing commitment to the Patient and Carer Race Equality Framework (PCREF) by exploring how creativity, culture and storytelling can strengthen co-production and improve relationships between carers and services. The afternoon was designed around inclusion, psychological safety and optional participation, allowing people to contribute in whatever way felt comfortable to them.
As someone who has cared for family members affected by severe mental illness for many years, I continue to believe that poetry allows carers to communicate emotions that ordinary conversations often fail to capture. Statistics tell us what is happening, but poetry often explains how it feels. This aligns closely with PCREF’s ambition to humanise care, improve understanding of racial inequalities and ensure lived experience genuinely influences service development.
The event opened with readings from my forthcoming collection of PCREF poems, including “Change is Possible.” Rather than focusing solely on racism, the discussion explored hope, community, partnership, co-production and carers becoming recognised as equal partners within mental health care. Participants reflected that although change often feels slow, meaningful progress can still occur when carers are given opportunities to influence services.
One participant commented that the poem should never have needed to exist because carers should already be recognised and listened to. Another reflected that the line “those doors open slowly” accurately described the experience of advocating for loved ones over many years. These discussions reminded everyone that poetry can stimulate conversations which may never emerge during formal meetings or consultations.
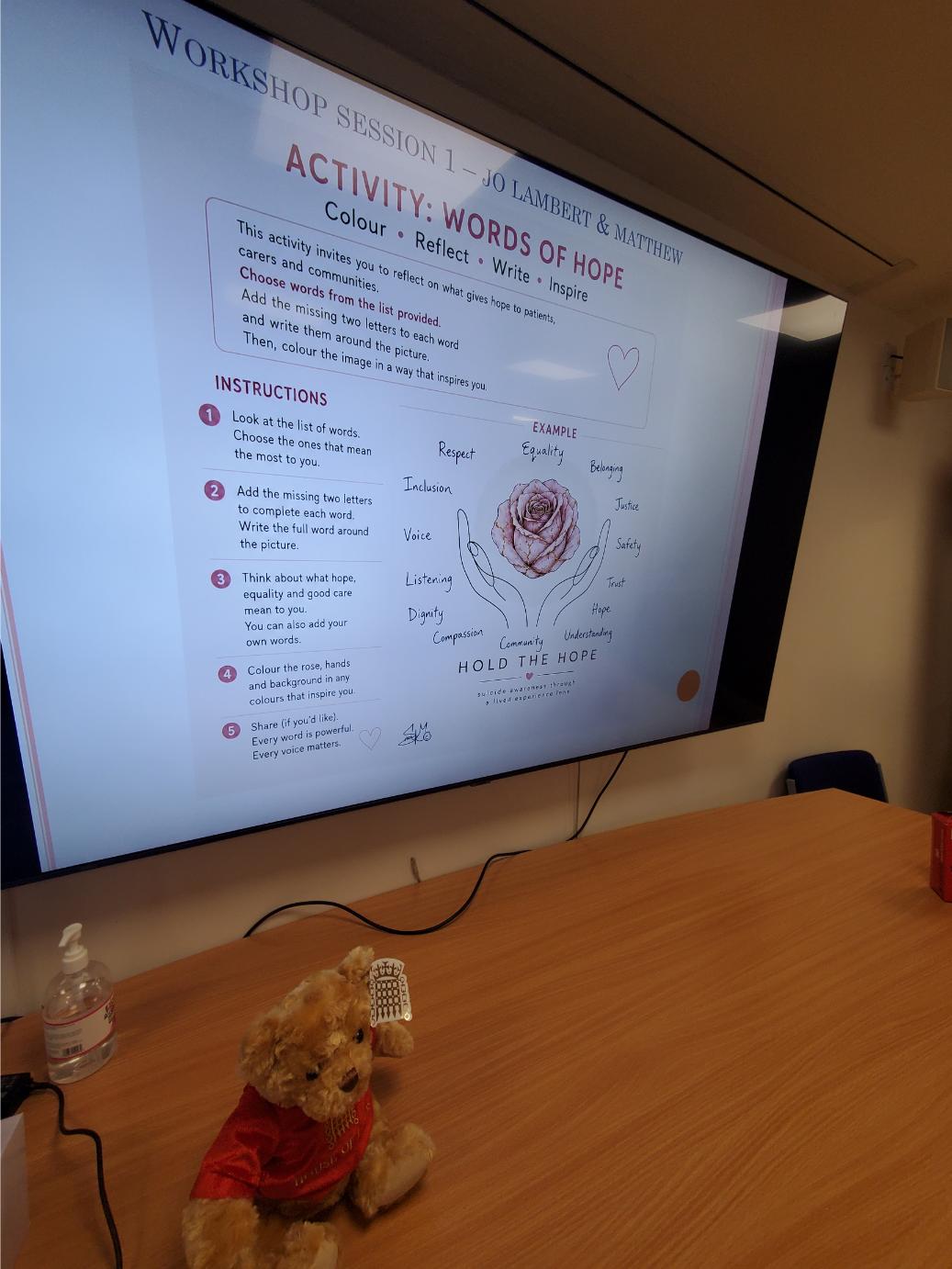
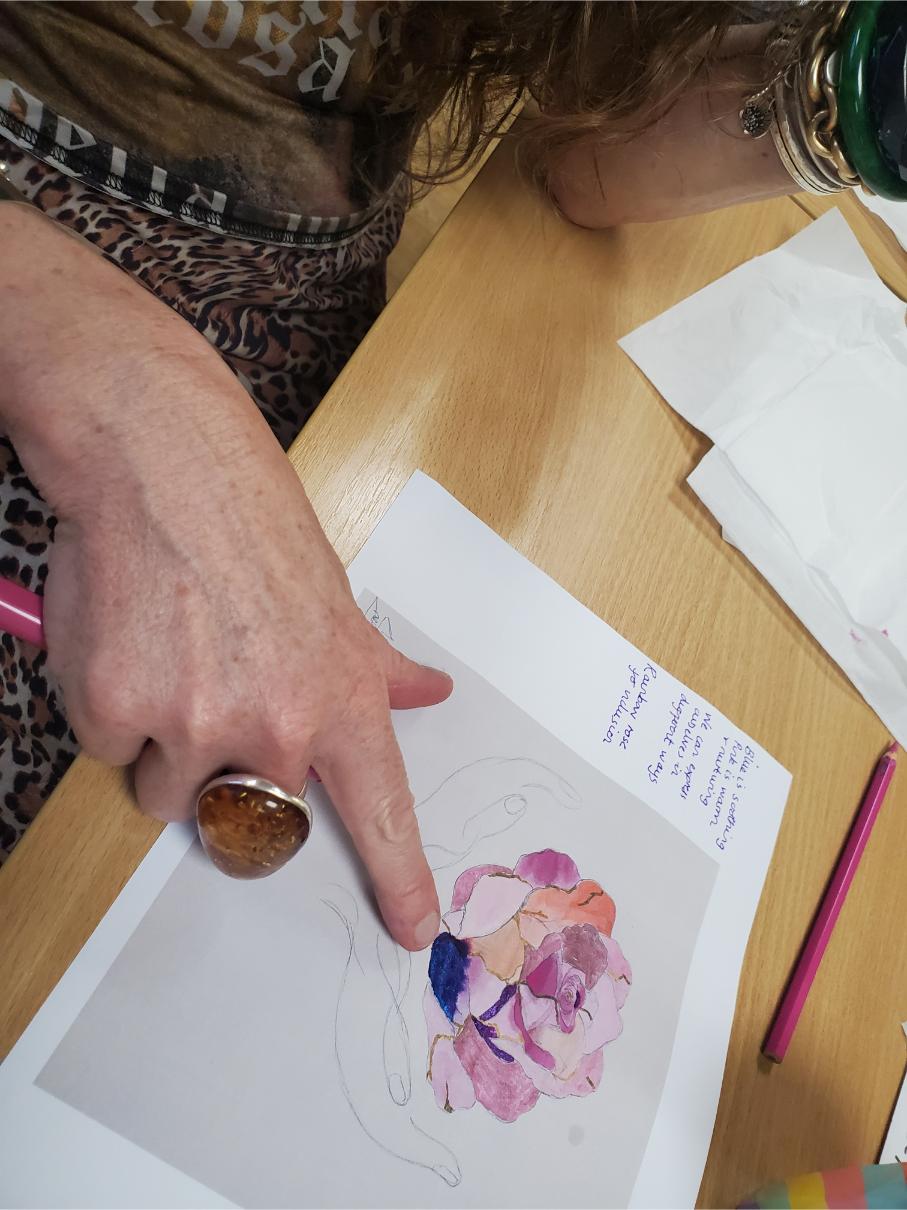
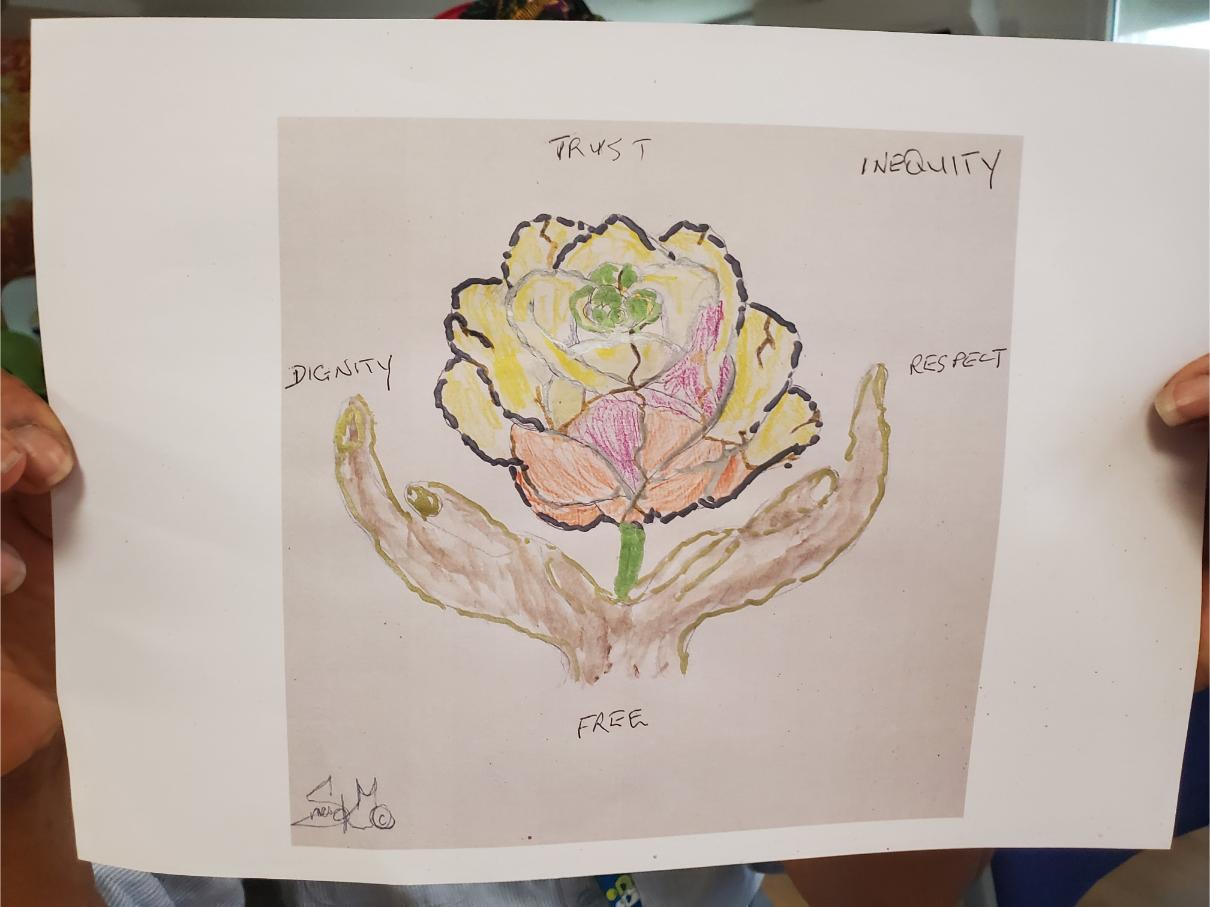
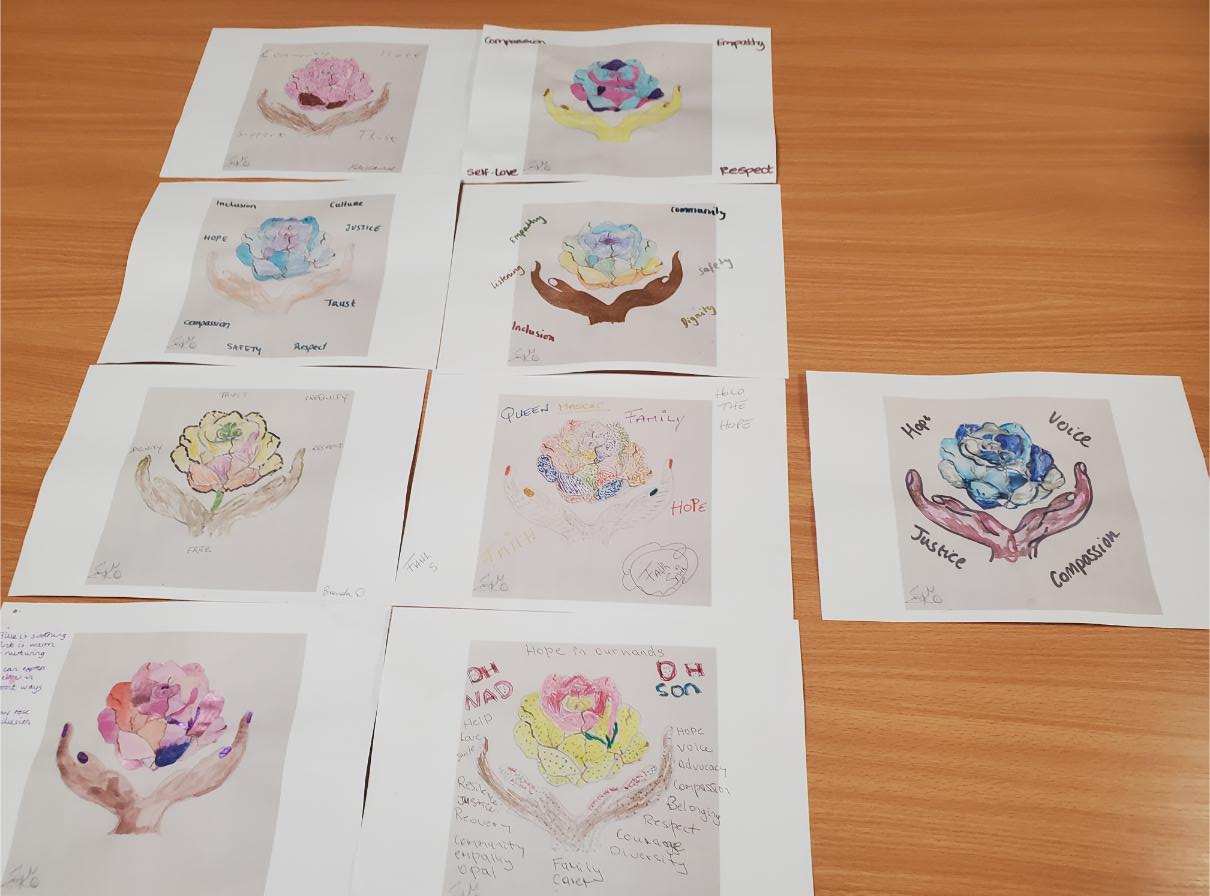
One of the highlights of the afternoon was a collaborative workshop led by Jo Lambert, introducing participants to the Hold the Hope project through art, colour and reflection.
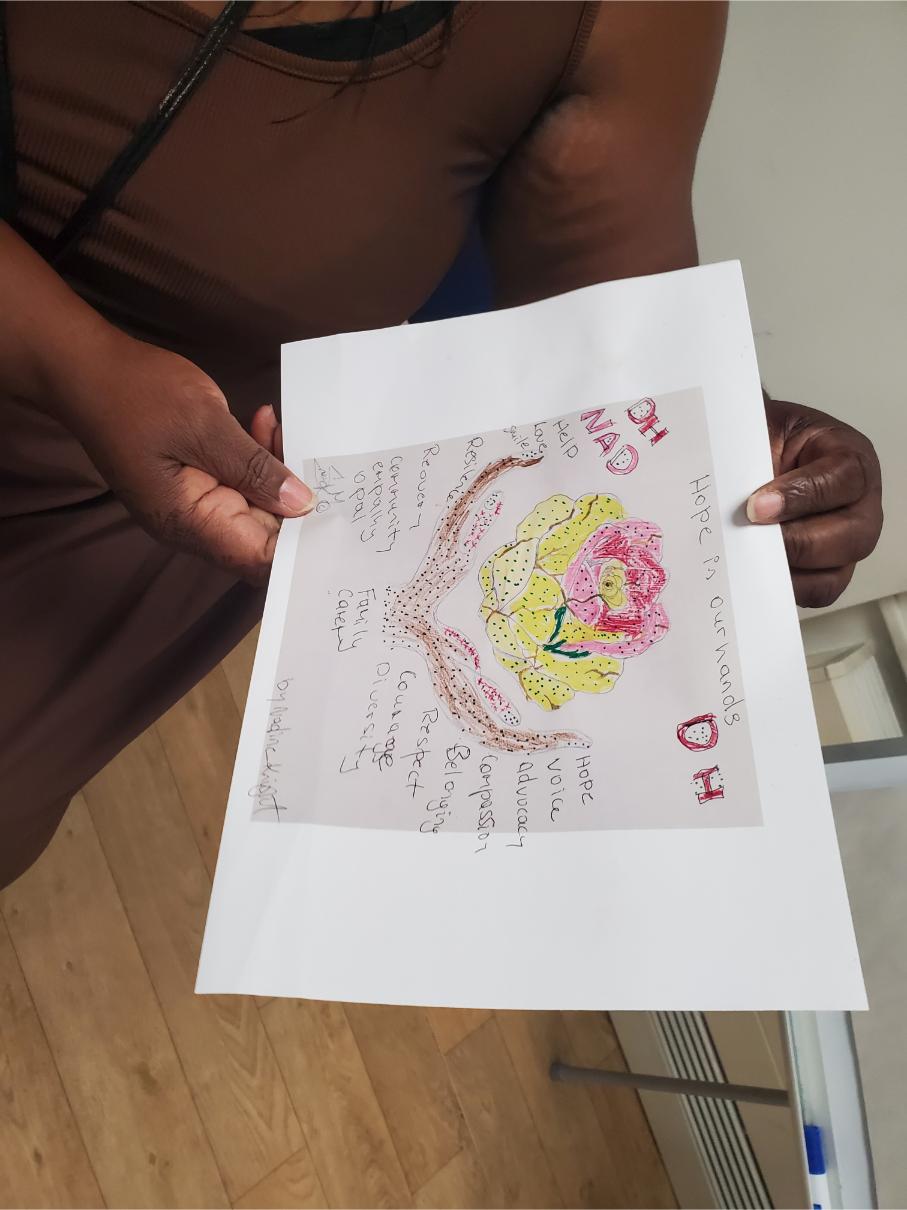
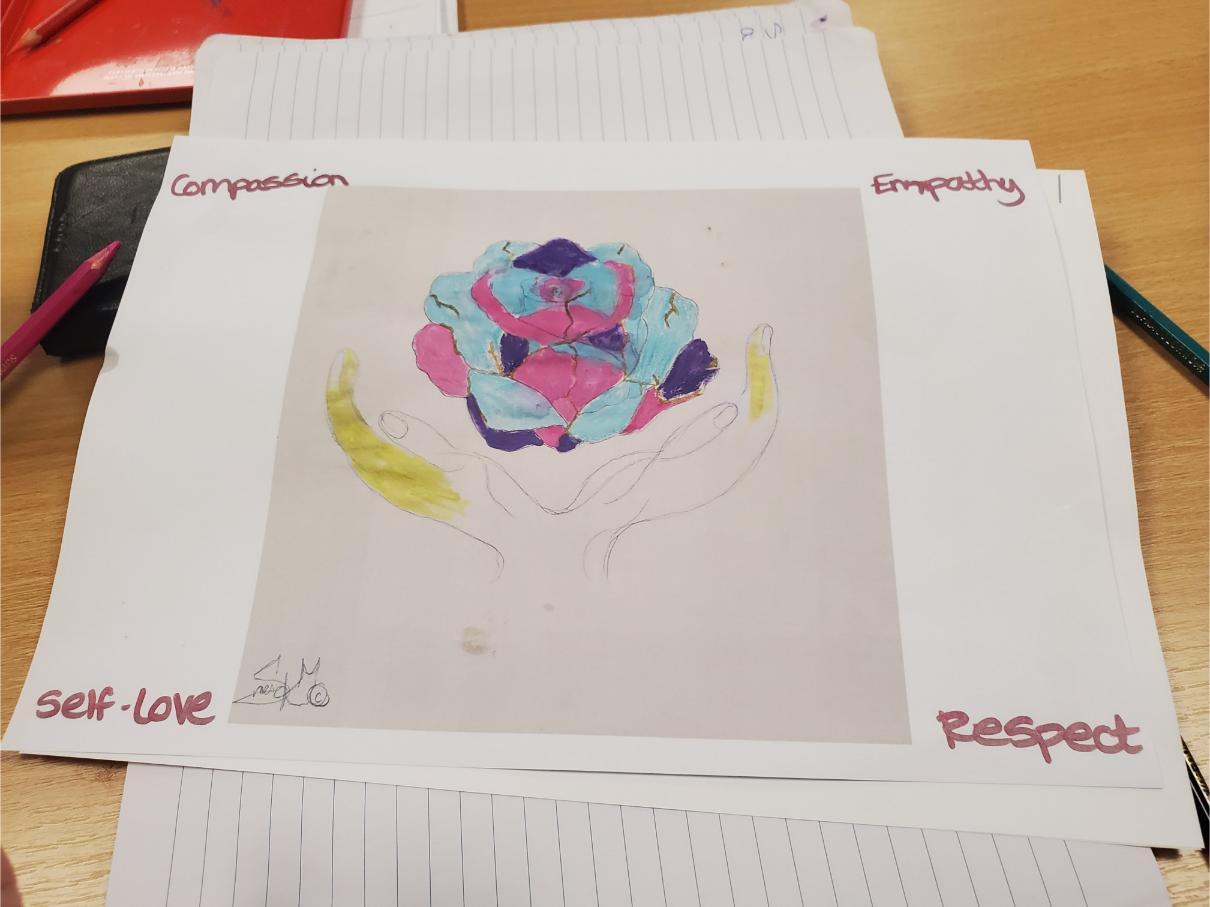
Rather than asking carers to simply colour a picture, participants were encouraged to think about what hope, equality, dignity and belonging meant to them personally. They selected PCREF-related words, explored why particular colours reflected their emotions and discussed how creativity can communicate experiences beyond spoken language.
The discussion demonstrated that every participant interpreted the same image differently.
Some chose calming blues to represent peace and trust.
Others used brighter colours to symbolise recovery, resilience and optimism.
Several carers explained that colouring became a form of mindfulness, allowing them to process difficult emotions whilst talking with others.
The activity also highlighted something particularly important from a lived experience perspective. Mental health carers frequently spend years speaking on behalf of others. Opportunities to express their own feelings are much rarer. Through art and poetry, carers were able to focus on themselves without feeling they had to justify or defend their experiences.
This reinforced one of the strongest messages of the day:
Creative expression is not simply an enjoyable activity, it is another form of lived experience evidence.
Participants also appreciated that there were no “right” or “wrong” answers. Every artwork reflected an individual caring journey, demonstrating the diversity that exists within the unpaid carer community.
The power of shared lived experience
Perhaps the most valuable aspect of the event was the conversation that developed naturally between carers.
Discussions moved beyond poetry into themes including:
feeling excluded because of confidentiality
racial inequality within services
the emotional burden of long-term caring
recognition of carers as equal partners
loss of identity through caring
maintaining hope during crisis
the importance of community support
Many participants reflected that carers often possess significant practical knowledge but are still not viewed as equal partners within clinical decision making.
One participant explained that carers are frequently expected to educate professionals whilst simultaneously managing the emotional impact of supporting someone in crisis. Others spoke about the exhaustion of constantly advocating for loved ones whilst trying to maintain their own wellbeing.
These conversations demonstrated exactly why creative events have an important place within PCREF. Rather than collecting another questionnaire, participants were able to describe experiences in their own words, using poetry, storytelling and discussion.
Importantly, professionals attending the session also listened.
This helped create genuine dialogue rather than the traditional model where professionals ask questions and carers provide short answers.
The atmosphere remained respectful throughout, allowing difficult topics including racism, discrimination and feeling unheard to be explored constructively.
For many attendees, simply meeting other carers who understood their experiences reduced feelings of isolation.
Celebrating culture and creativity
The second half of the afternoon celebrated cultural diversity through music, spoken word and performance.
Faith shared “Soothing Blue,” a poem that had been transformed into music. Hearing lived experience expressed through song demonstrated another creative way carers can communicate emotions that may otherwise remain hidden. Participants reflected on themes of healing, identity and rediscovering themselves beyond their caring role.
Brenda then performed traditional Jamaican folk songs, including “Chi-Chi Bud Oh” and “By the Rivers of Babylon.” These performances reminded everyone that culture forms an important part of identity and wellbeing. Cultural expression can strengthen belonging and create opportunities for people from different backgrounds to learn from one another.
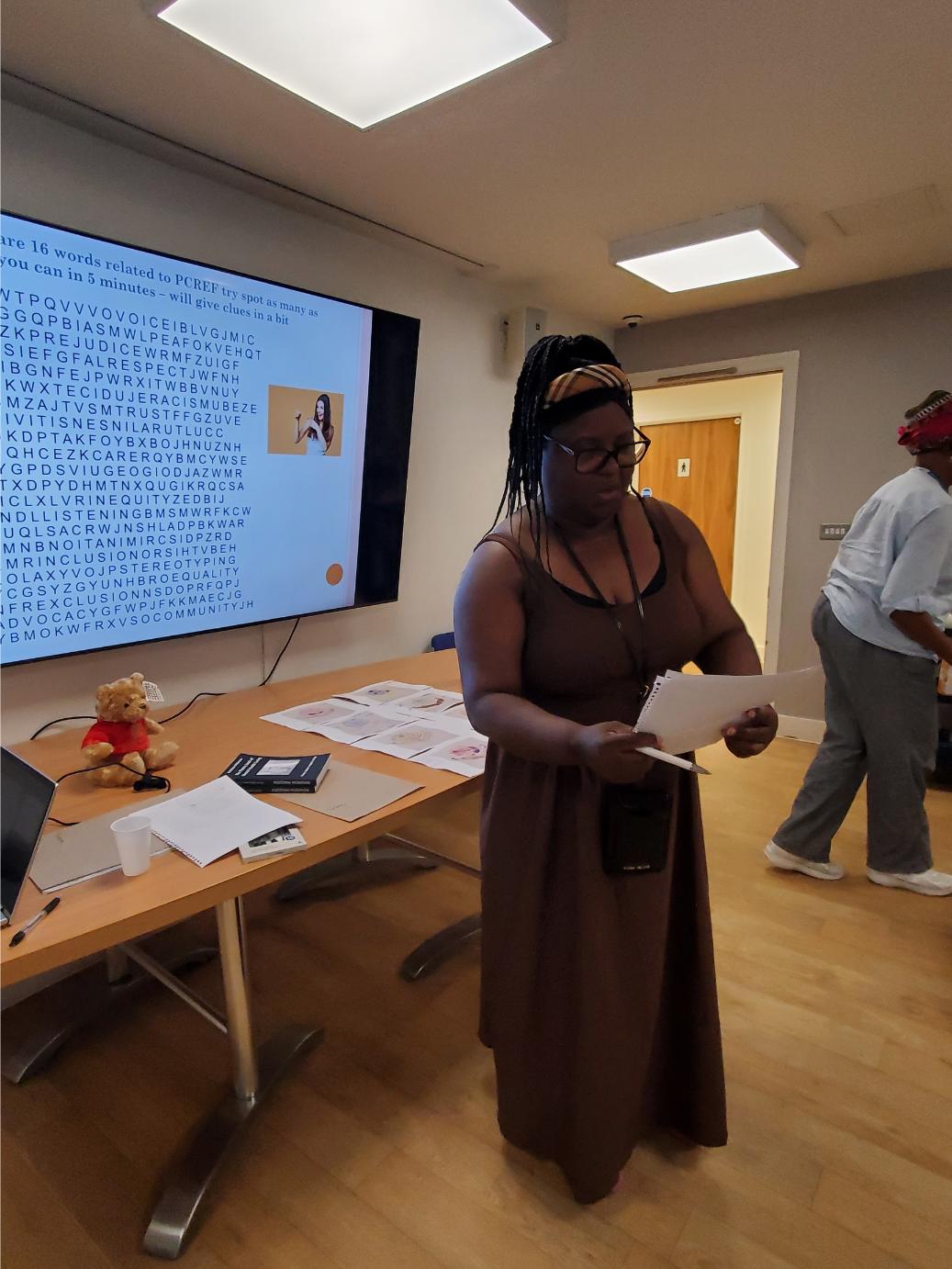
The PCREF word search and poetry activity further encouraged participants to explore words such as community, dignity, inclusion, hope, equality and compassion before creating short poems of their own. What initially appeared to be a simple puzzle became another opportunity for reflection and discussion.
Throughout the afternoon there was laughter, encouragement and mutual support. Participants applauded one another’s contributions regardless of previous poetry experience, reinforcing that everyone had something valuable to contribute.
By combining poetry, visual art, music and conversation, the event demonstrated that creativity can become a powerful vehicle for engagement with carers who may not usually participate in traditional consultation events.
Reflections and looking ahead
Looking back as both a lived experience carer and PCREF Carer Lead, I believe this event demonstrated several important lessons.
Firstly, carers do not simply want to be consulted, they want to be heard.
Secondly, creative approaches allow conversations to emerge that formal meetings often miss.
Thirdly, culture matters. When people feel safe enough to bring their whole identity into a room, discussions become richer, more authentic and more meaningful.
The Voices & Verses programme is gradually becoming more than a poetry group. It is developing into a community where carers can connect, learn from one another and influence future mental health services through creativity.
Future events will continue to develop this approach by:
expanding hybrid participation so more carers can join remotely;
increasing opportunities for cultural storytelling;
creating more collaborative art and poetry projects;
transforming poems into music and other creative media;
strengthening links between PCREF, Triangle of Care and co-production.
Most importantly, the event reminded us that lived experience should never be viewed as an optional extra.
Every poem, every conversation and every shared story represented expertise developed through years of caring.
PCREF asks organisations to listen more carefully to diverse communities.
This event showed that when carers are given the right environment, they do not simply speak—they inspire, educate and help shape better mental health services for everyone.
By Matthew McKenzie – Chair, National Ethnic Mental Health Carers Forum
The July meeting welcomed unpaid carers, NHS organisations, universities, researchers and community groups from across England to discuss how mental health services can become more inclusive for carers from ethnic communities.
Matthew McKenzie opened the meeting by reflecting on over thirteen years of facilitating the forum and explained how its purpose has grown alongside national initiatives such as the Patient and Carer Race Equality Framework (PCREF) and the Triangle of Care. The forum continues to provide a national platform where carers can influence NHS services, hear about new research and share experiences with professionals and decision-makers.
Matthew introduced the day’s programme, which included research presentations, NHS England engagement, updates from mental health trusts and national organisations, and opportunities for carers to influence future policy
Dr Ida Doherty – King’s College London
Supporting Ethnic Carers in South West London
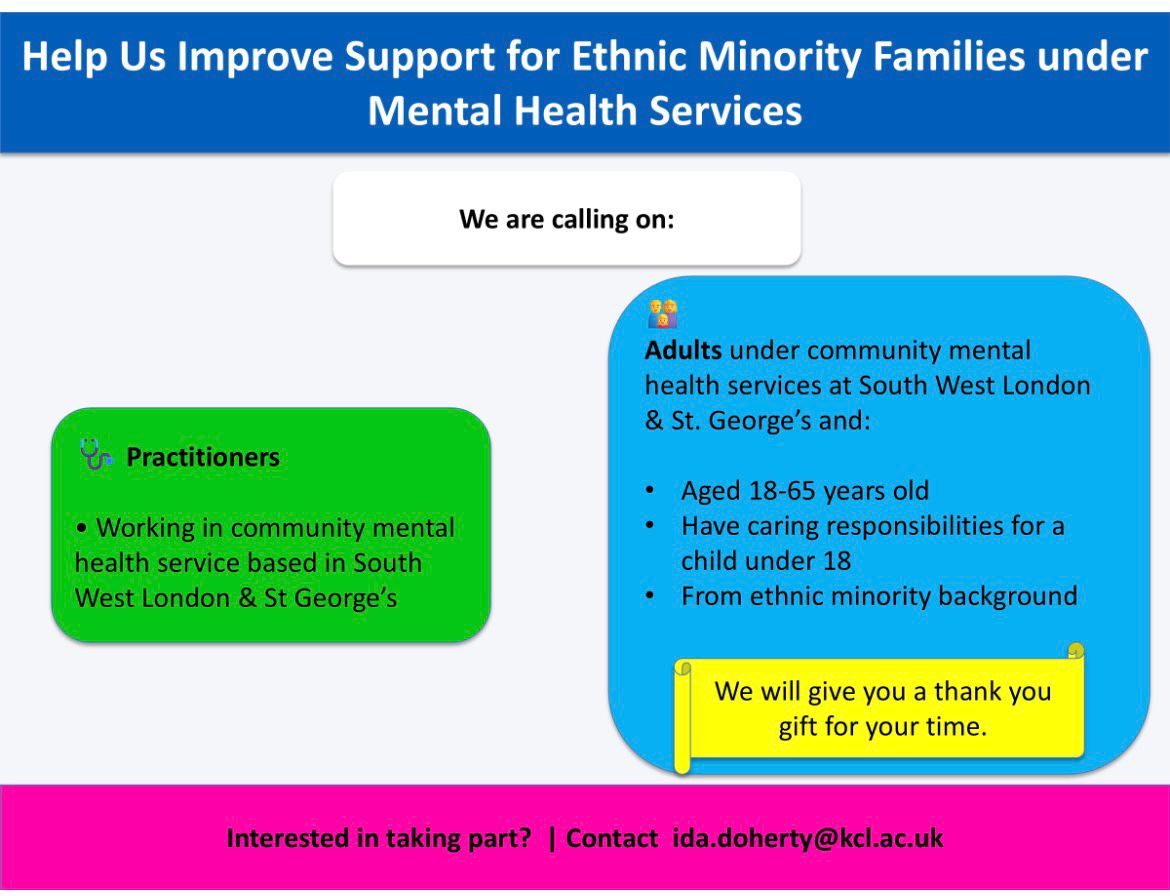
Dr Ida Doherty presented her doctoral research exploring how adult mental health services support ethnic minority families where a parent experiences mental illness.
She explained that despite national policy promoting a Think Family approach, implementation across England remains inconsistent. Many parents receiving mental health support are never asked about their children, meaning opportunities for preventative family support are often missed.
Discussion Highlights
This presentation generated one of the longest discussions of the meeting.
Carers highlighted:
Adult and children’s services continue to work separately.
Families often have to repeat their stories to multiple organisations.
Parents fear seeking support because of concerns about children being removed.
Structural racism continues to affect safeguarding and mental health services.
Disabled parents and carers experience multiple layers of discrimination.
Services often respond only during crisis rather than providing early intervention.
There was also an important discussion about safeguarding carers who participate in research. Participants stressed that research should include emotional support, culturally appropriate safeguarding and co-produced approaches to prevent re-traumatisation. Dr Doherty welcomed these suggestions and explained the safeguarding measures built into her study.
Dr Doherty encouraged forum members to promote the study across South West London to help ensure ethnic families are represented within the research.
Certainly. Here’s a more professional version that focuses on the discussion rather than identifying who asked each question.
Questions and Discussion
Q1. How can mental health services better implement the “Think Family” approach?
A question was raised about the continuing separation between children’s and adult mental health services, with concern that families are often required to navigate multiple systems that fail to communicate with one another. It was suggested that supporting one family member in isolation overlooks the wider impact of mental illness on the entire household.
Response
Dr Doherty agreed that this is a significant challenge and explained that her research is centred on improving whole-family support. She highlighted that current services often operate in silos, limiting opportunities for early intervention and joined-up care. The aim of her research is to identify practical ways of embedding the Think Family approach more effectively within adult mental health services.
Q2. How will the research address the inequalities experienced by ethnic minority families?
A discussion focused on the additional challenges faced by ethnic minority families, particularly where disability, poverty, language barriers and mental health intersect. Concerns were raised about institutional racism, unequal treatment and the fear some parents experience when engaging with services.
Response
Dr Doherty acknowledged that these intersecting inequalities can significantly affect families’ experiences. She recognised that services can often adopt a risk-focused rather than strengths-based approach and explained that her research seeks to identify earlier, more supportive interventions that better meet the needs of ethnic minority families.
Q3. How will carers participating in the research be protected from emotional harm?
The discussion explored the importance of safeguarding participants involved in research. It was suggested that sharing lived experiences can be emotionally challenging and that researchers should have appropriate support mechanisms in place before, during and after participation.
Response
Dr Doherty explained that safeguarding had been a key consideration throughout the development of the study. She described how support, supervision, training and ongoing review have been built into the project, alongside close collaboration with Experts by Experience from the earliest stages of the research.
Q4. Will participants receive ongoing emotional support after difficult discussions?
A further question explored whether structured debriefing and emotional support would be available for participants who may experience distress after discussing traumatic experiences.
Response
Dr Doherty confirmed that the study includes a comprehensive safeguarding framework, including debrief sessions and wellbeing support. She explained that the project had undergone rigorous NHS ethics approval and that participant welfare continues to be reviewed throughout the research process.
Q5. How is co-production embedded within the research?
The final discussion focused on ensuring that the research is genuinely co-produced with ethnic communities rather than being designed solely from a professional perspective. There was also support for developing safeguarding approaches jointly with carers.
Response
Dr Doherty explained that co-production is fundamental to the project. She has worked alongside Experts by Experience since the study was first developed and described the research as something being undertaken in partnership with people who have lived experience. She also welcomed suggestions for strengthening carer-led safeguarding approaches as the project progresses.
Dr Maeve (King’s College London)
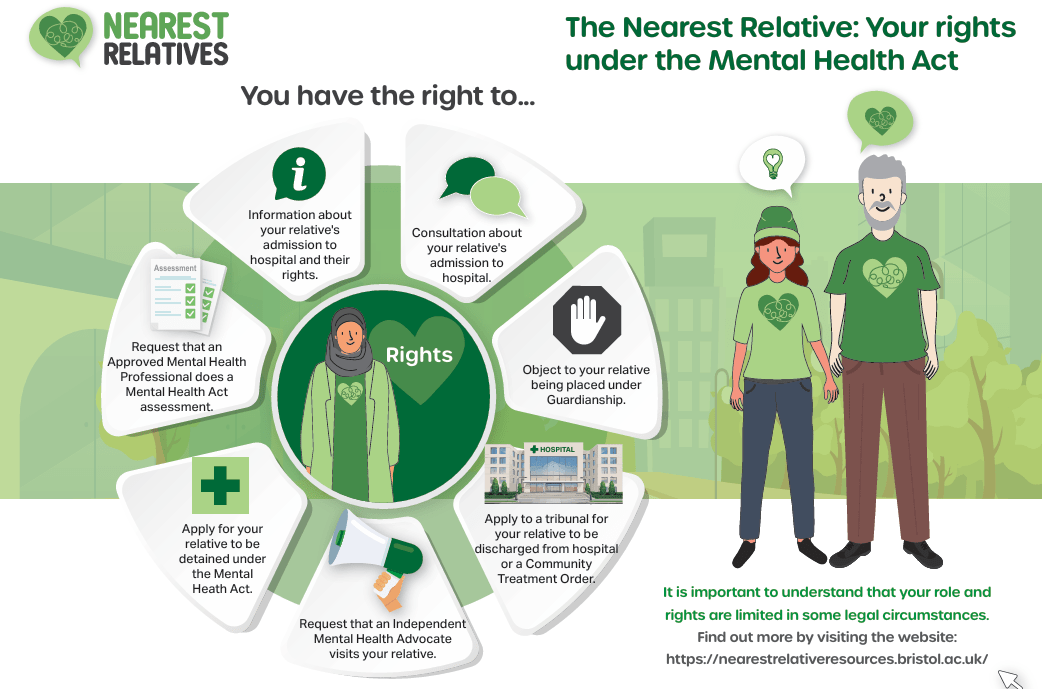
Research Study: The Nearest Relative under the Mental Health Act
Dr Maeve introduced a new King’s College London research project examining experiences of the Nearest Relative provisions within the Mental Health Act. She explained that the study aims to understand how the current legislation works in practice and gather views ahead of the proposed reforms to mental health law. The researchers are interested in hearing directly from people who have lived experience of the system, recognising that the Nearest Relative can play a crucial role in supporting someone during assessment, detention and treatment.
The study is seeking participants from a range of backgrounds, particularly unpaid carers who have supported someone detained or assessed under the Mental Health Act, as well as individuals who have themselves experienced detention or assessment. The research team is especially keen to hear from Black and other ethnic minority communities, along with younger people, to ensure that a wide range of perspectives help inform future policy and practice. Interviews are conducted online via Microsoft Teams at a convenient time for participants, last approximately one hour, and participants receive a £30 shopping voucher as a thank-you for contributing their experiences. Dr Maeve encouraged anyone interested to contact the research team or share the opportunity with others who may wish to participate.
Ruby Neish – University College London
Cancer Care and Black Women
Research Study: Supporting Carers of Women with Endometrial (Womb) Cancer
Ruby Neish, a Master’s researcher from University College London working in collaboration with the Centre for Early Detection, introduced a research project exploring the experiences of family members, friends and unpaid carers supporting women diagnosed with endometrial (womb) cancer. She explained that while much research focuses on the experiences of patients themselves, comparatively little is known about the challenges faced by those providing informal care throughout diagnosis, treatment and recovery. The study aims to build a more complete picture by understanding how carers experience the cancer pathway, the support they receive and the barriers they encounter. Ruby emphasised that carers often play a vital role in navigating appointments, providing emotional support, helping with treatment decisions and managing the practical realities of living with cancer, yet their experiences are frequently overlooked in research.
Following the presentation, forum members shared a wealth of lived experience highlighting why this research is particularly important for Black and minority ethnic communities. The discussion explored how delayed diagnosis, language barriers, cultural expectations, disability, poor communication and wider health inequalities can all contribute to poorer experiences for both patients and their families. Members also reflected on the importance of improving awareness of cancer symptoms within communities, encouraging uptake of screening programmes and ensuring services are culturally responsive. Several contributors stressed that carers often become advocates, interpreters and navigators of the healthcare system, particularly where individuals experience multiple forms of disadvantage. The discussion reinforced the importance of ensuring that future cancer services recognise and support carers as an essential part of the patient’s journey.
Questions and Discussion
Q1. Why is it particularly important to understand the experiences of Black and minority ethnic women living with cancer?
Forum members discussed how people from Black and minority ethnic communities can face additional barriers throughout the cancer pathway. These included language differences, lower awareness of symptoms, cultural beliefs about illness, disability, mental health needs and difficulties accessing appropriate support. It was suggested that these factors can contribute to delayed diagnosis and poorer outcomes if services fail to respond to people’s individual circumstances.
Response
Ruby welcomed these observations and explained that hearing directly from carers is essential to understanding these inequalities. She noted that while patients’ experiences are being explored separately, the research hopes to capture the perspectives of carers to identify barriers that may otherwise remain invisible. Together, these findings will help build a more complete understanding of how cancer services can better support families from diverse communities.
Q2. How can cancer services improve early diagnosis within ethnic communities?
The discussion highlighted the importance of encouraging earlier engagement with screening programmes and improving awareness of cancer symptoms within local communities. Examples were shared of women whose diagnoses were delayed after repeated visits to healthcare services, alongside reflections on the positive impact that culturally appropriate information and trusted community support can have in encouraging people to attend screening appointments. Participants emphasised that services need to communicate in ways that are accessible and sensitive to different cultural backgrounds.
Response
The discussion reinforced that improving awareness, reducing communication barriers and working more closely with communities could contribute to earlier diagnosis and improved outcomes. The research aims to identify where carers believe improvements can be made across the diagnostic and treatment journey, helping to inform future service development.
Q3. What role do unpaid carers play throughout the cancer journey?
A final discussion focused on the often unseen contribution of unpaid carers. Members described how carers frequently provide emotional reassurance, accompany relatives to appointments, help explain medical information, advocate for concerns to be taken seriously and support individuals throughout treatment and recovery. It was recognised that carers often become the link between patients, families and healthcare professionals, particularly where communication barriers or additional health conditions exist.
Response
Ruby explained that this is precisely why the study is focusing on carers’ perspectives. Understanding their experiences will provide valuable evidence about the practical and emotional challenges carers face and identify ways that cancer services can better recognise and support them alongside the person receiving treatment.
NHS England – Allied Health Professions Strategy
Steve Tolan (Deputy Chief Allied Health Professions Officer) & Barry O’Donovan (Senior Programme Manager)
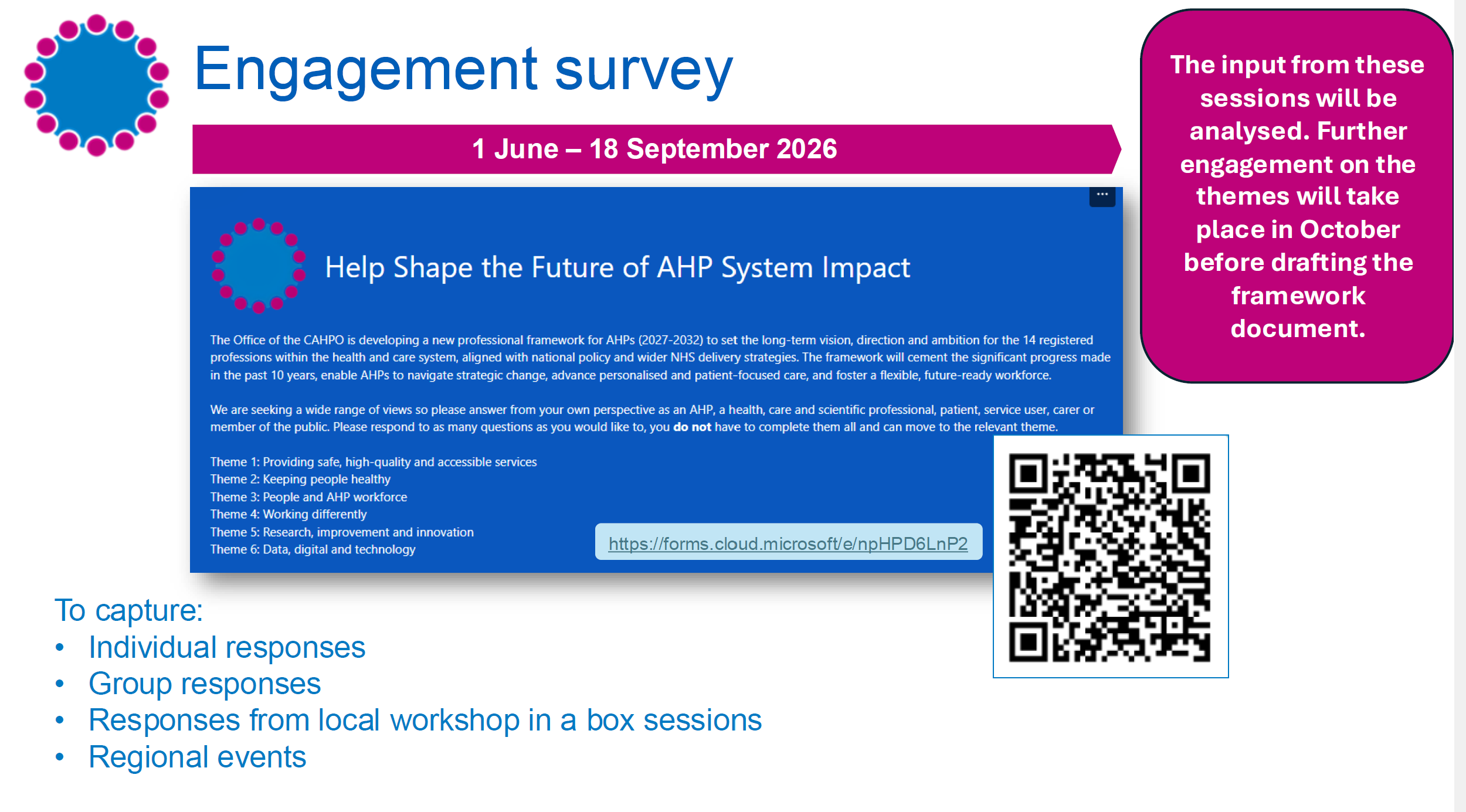
Steve Tolan and Barry O’Donovan from NHS England joined the forum to begin an important conversation about developing a new national Allied Health Professions (AHP) Strategy. Rather than presenting a completed strategy for consultation, they explained that NHS England wanted to engage with carers, patients and communities before the strategy was written, ensuring that lived experience would help shape its priorities from the outset.
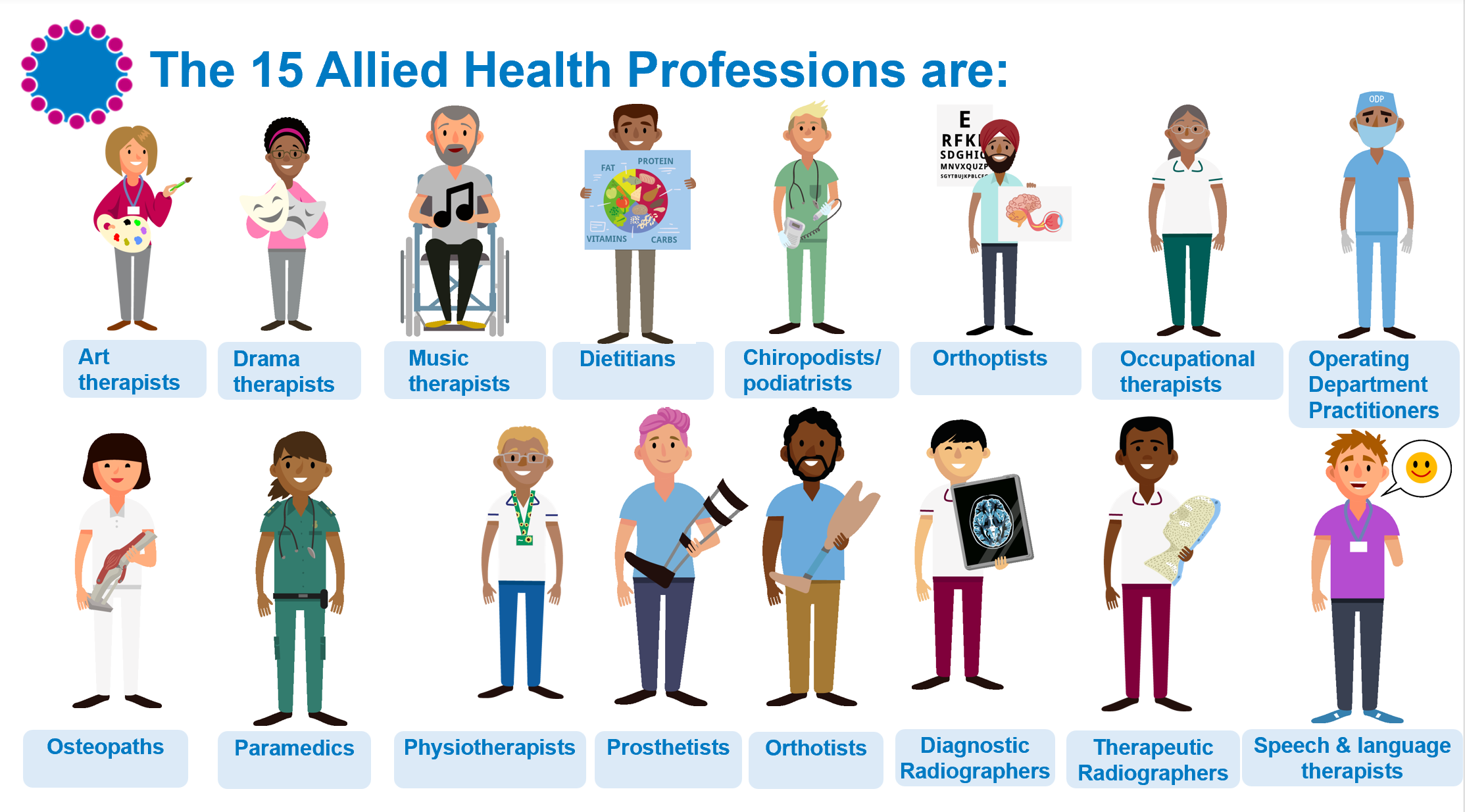
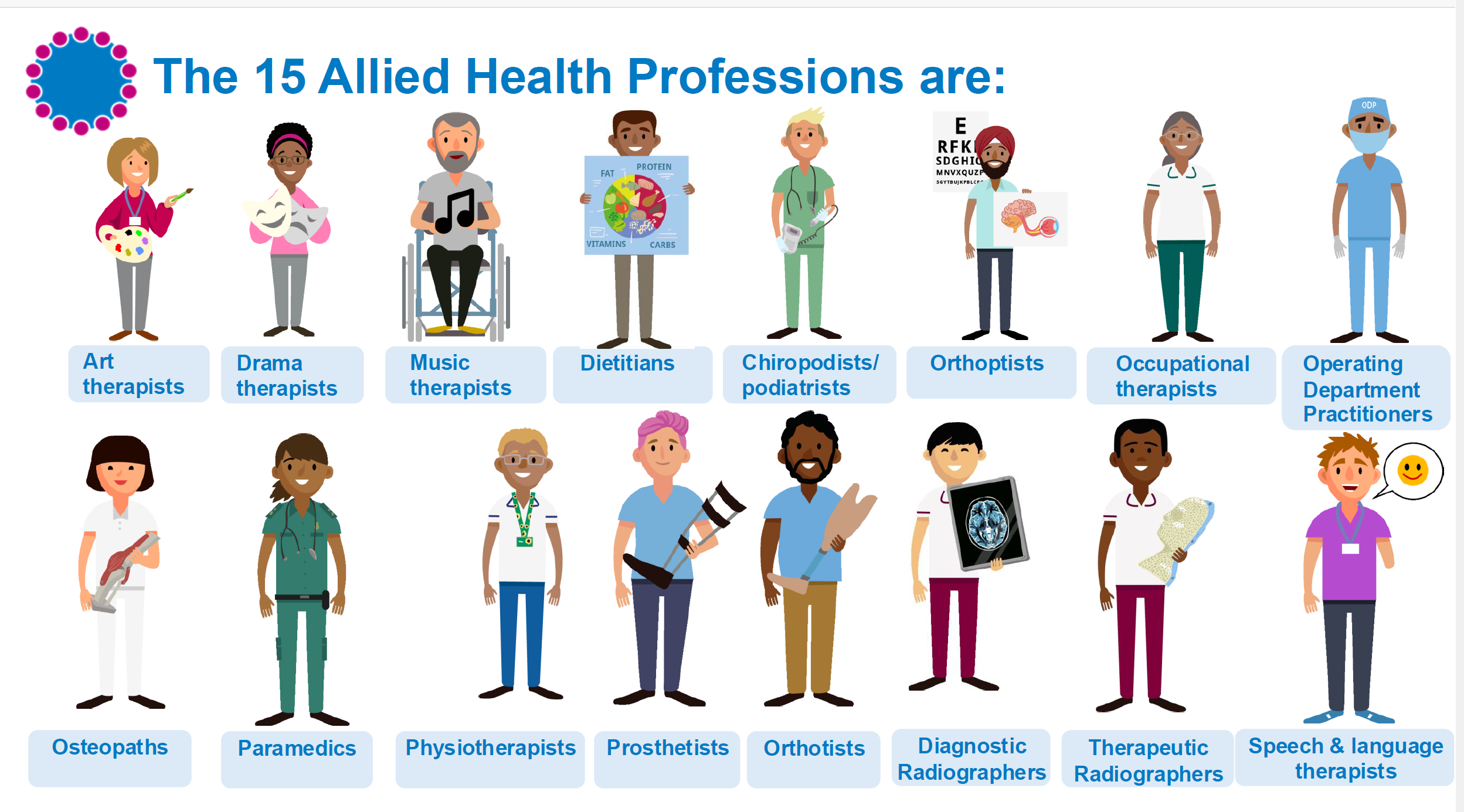
Steve introduced the Allied Health Professions as the third largest clinical workforce in the NHS, comprising fourteen professions including occupational therapists, physiotherapists, speech and language therapists, dietitians, radiographers and several others. He explained that these professionals work across virtually every part of health and care, from mental health and primary care to acute hospitals, rehabilitation and community services, making their contribution central to improving patient outcomes.
Barry explained that NHS England was seeking honest feedback on what Allied Health Professionals currently do well and, more importantly, where improvements were needed over the next five years. The discussion centred around several key questions, including how AHPs could help people stay healthier for longer, improve prevention, reduce health inequalities, remove barriers to accessing care, and work more effectively across different care settings. Forum members were also encouraged to complete a wider national survey, but NHS England emphasised that hearing directly from unpaid carers during the meeting would provide invaluable insight into the everyday realities experienced by families supporting loved ones with mental illness and other long-term conditions.
What followed was one of the richest discussions of the meeting, with carers sharing personal experiences of navigating health services and offering practical recommendations for change. Contributors acknowledged the important work undertaken by Allied Health Professionals but stressed that future success would depend upon moving beyond clinical interventions alone. Members called for greater emphasis on prevention rather than crisis management, stronger action to address racism and health inequalities, more personalised and culturally responsive care, improved communication with families and better recognition of unpaid carers as essential partners within the healthcare system. NHS England representatives listened carefully throughout the discussion, responding positively to the feedback and confirming that the experiences shared during the forum would help inform the development of the national strategy.
Feedback from Forum Members
There was a lot more feedback, but I have only included 4 feedback to the strategy
Feedback 1 – Prevention must become the priority, not simply responding to crisis
One of the strongest messages from the discussion was that health services often intervene too late. Contributors explained that many families recognise early warning signs long before services become involved, yet support is frequently unavailable until a situation has escalated into crisis. Members argued that Allied Health Professionals are well placed to identify emerging concerns earlier, particularly for people living with long-term mental health conditions, autism, learning disabilities and chronic physical illnesses. Earlier intervention, they suggested, would reduce avoidable hospital admissions while improving outcomes for both patients and carers.
NHS England acknowledged this feedback, explaining that one of the key ambitions of the new strategy is to support the wider NHS objective of shifting from reactive treatment towards prevention. Representatives welcomed examples from carers illustrating where earlier support could make the greatest difference.
Feedback 2 – Tackling racism and health inequalities requires more than training
Forum members spoke candidly about experiences of racism, discrimination and unequal treatment within health services. While acknowledging that cultural awareness training is becoming more common, contributors argued that training alone is insufficient unless accompanied by accountability and meaningful changes in practice. Some described inaccurate clinical records, assumptions based on ethnicity and situations where concerns raised by families were not properly reflected in care planning. There was a strong call for services to improve communication, record keeping and trauma-informed practice, ensuring that staff understand the impact of racism on health outcomes rather than viewing cultural competence as a one-off training exercise.
NHS England representatives recognised that tackling health inequalities and promoting anti-racist practice were already identified as “non-negotiable” priorities within the developing strategy. They explained that this was precisely why engagement with forums such as this was so valuable, helping ensure that policy reflects the real experiences of people using NHS services.
Feedback 3 – Unpaid carers must be recognised as equal partners in care
A recurring theme throughout the discussion was the role of unpaid carers within healthcare systems. Members explained that carers are often the people coordinating appointments, supporting communication, monitoring deterioration, providing emotional support and helping professionals understand an individual’s needs. Despite this, carers frequently remain unidentified by services or receive little information and support themselves. Contributors argued that Allied Health Professionals should routinely identify carers, involve them in care planning where appropriate and recognise them as equal partners whose knowledge can significantly improve patient outcomes.
NHS England welcomed these comments and recognised that carers play a fundamental role in delivering effective, preventative care. The examples shared demonstrated how stronger partnerships with carers could improve continuity of care while helping services better understand the needs of individuals and families.
Feedback 4 – Share and learn from examples of excellent practice
The discussion concluded with examples of positive experiences that illustrated what good care can look like. One contributor described receiving outstanding support from an Occupational Therapist who not only arranged practical adaptations within the home but also followed up afterwards to ensure everything was working well. Members suggested that NHS England should identify and promote examples of excellent practice across the Allied Health Professions so that high standards become the norm rather than the exception. Ideas included involving patients and carers more directly in evaluating services and using lived experience to help identify what compassionate, person-centred care looks like in practice.
West London Health Trust – PCREF Update
Linda Thomas – Co-producing an Independent PCREF Advisory Group
Linda Thomas, Co-production and Partnerships Development Manager at West London NHS Trust, opened the Trust’s presentation by describing how they have developed an independent PCREF Advisory Group designed to challenge, support and hold the Trust to account as a “critical friend.” Rather than creating a traditional advisory panel, West London NHS Trust commissioned three established community organisations GOS&D (Ealing), SHEWISE (Hounslow) and Managing Our Mental (Hammersmith & Fulham) to help design the model and understand how communities genuinely want to engage with mental health services. The approach seeks to increase diversity of voices, identify barriers preventing community involvement and rebuild trust between local communities and the Trust. Linda explained that members of the advisory group now sit alongside Trust leaders as equal partners on the Steering Group, while work is progressing to secure long-term funding to sustain the network and strengthen relationships with community organisations. The initiative demonstrates how co-production can move beyond consultation towards genuine shared decision-making between the NHS and the communities it serves.
Debbie Best – PCREF Carer Lead: Racial Trauma Workshops
Debbie Best, PCREF Carer Lead at West London NHS Trust, presented the development of the Trust’s Racial Trauma Workshops, which were co-designed alongside Natalie Mark (PCREF Lived Experience Lead), Dr Anne Aiyegbusi and Chief Nurse Gillian Kelly. Debbie explained that the workshops were created in response to the persistent racial inequalities experienced within mental health services, including disproportionate detention under the Mental Health Act, restrictive interventions, mistrust of services and the re-traumatisation experienced by many people from ethnic communities.
Rather than delivering traditional equality training, the workshops create reflective spaces where staff openly discuss difficult issues including trust, power, emotional labour, racialised assumptions and barriers to culturally safe care. Debbie emphasised that racial trauma affects not only patients but also carers and NHS staff, and that creating psychologically safe spaces for honest conversations is an essential step towards improving relationships, reducing inequalities and embedding the aims of the Patient and Carer Race Equality Framework (PCREF) across mental health services.
Christine – Triangle of Care, Carer Awareness Training and PCREF
Christine, speaking as a carer representative involved in co-production, highlighted how West London NHS Trust has successfully embedded carers within staff training through the Triangle of Care programme. She explained that the Trust achieved Stage 2 Triangle of Care accreditation in March 2026 and has developed Carer Awareness Training that is designed and delivered alongside carers themselves.
The training introduces staff to both the Triangle of Care and the Patient and Carer Race Equality Framework, helping colleagues understand the importance of recognising carers as equal partners while strengthening communication and collaboration with families. Christine also announced that West London NHS Trust has been selected as one of only thirteen national pilot sites testing the integration of Triangle of Care and PCREF guidance over the next twelve months. Ten clinical teams will take part in reviewing and implementing the updated guidance, ensuring that national best practice is informed by both professional expertise and lived experience.
Debbie Best – Ethnicity Data Capture Project
Debbie concluded the presentation by introducing West London NHS Trust’s Ethnicity Data Capture Project, funded through a small grant from the NHS Race and Health Observatory. She explained that the project aims to improve understanding of why ethnicity information is not always accurately recorded and why some communities remain reluctant to share this information. Working alongside community organisations including SHEWISE, Our Voices and Managing Our Mental, the Trust has co-produced a range of resources including information leaflets, awareness films, social media campaigns, frequently asked questions and staff training materials. The campaign, titled “Seen, Heard, Counted,” aims to reassure communities that ethnicity data is collected to improve healthcare, tackle inequalities and ensure services better reflect the needs of local populations. Debbie explained that the next phase of the project will focus on wider public awareness and rolling out staff training across the Trust to improve confidence, transparency and trust around ethnicity data collection.
Bren McInerney
Race Equality Observatory
Bren McInerney provided an update on behalf of the NHS Race and Health Observatory, explaining that although he works closely with the organisation through its Stakeholder Engagement Group, he was speaking from his role supporting engagement rather than as an NHS employee. He began by outlining the Observatory’s purpose, which is to identify, understand and help reduce ethnic inequalities across health and social care through research, evidence and partnership working.
Bren highlighted that the Observatory has now produced a growing body of evidence to support NHS organisations in tackling inequalities and emphasised that this work must ultimately lead to practical improvements in services rather than simply producing reports. He also noted that the Observatory’s current funding arrangement is due for renewal in 2027, making it increasingly important to demonstrate the value and impact of its work across the NHS. The presentation encouraged attendees to remain engaged with the Observatory’s programmes and continue sharing lived experience to strengthen the evidence base for future policy and service improvement.
Bren also highlighted several recent initiatives designed to strengthen collaboration between the NHS and local communities. These included the publication of the Trauma-Informed Care and Racialised Communities Report, which explores how trauma-informed approaches can better respond to the experiences of people affected by racism and discrimination. He also described the Observatory’s Small Grants Programme, which has supported community-led projects across England, and introduced a new Community Participation and Co-production Resource developed in partnership with the Race Equality Foundation. This resource aims to help NHS organisations and Integrated Care Boards build stronger relationships with communities, improve meaningful involvement in decision-making and ensure that local knowledge helps shape healthcare services. Bren concluded by encouraging carers, voluntary organisations and community leaders to make use of these resources, share them widely and continue influencing the national conversation on race equality within health services.
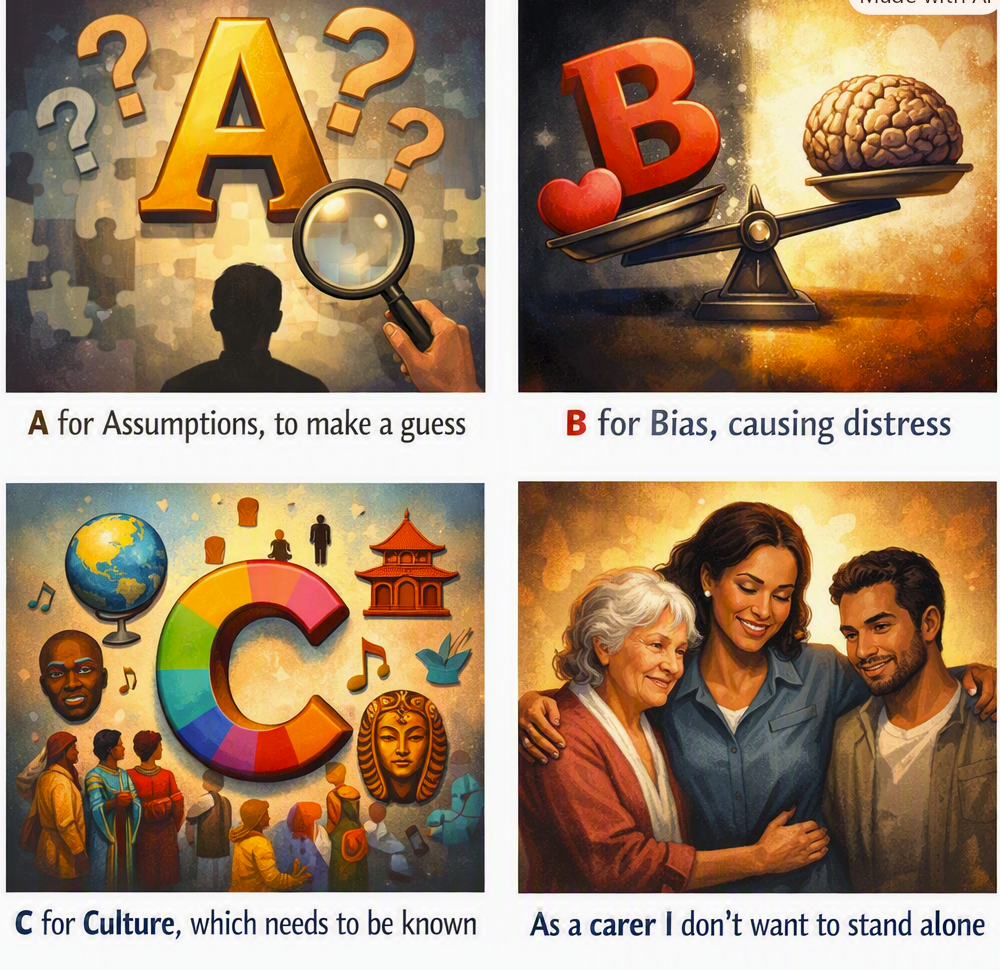
What does racial inequality in mental health really look like from the perspective of an unpaid carer?
In this powerful spoken-word poem, Matthew McKenzie explores the realities of racism, bias, exclusion, stigma, and unequal treatment experienced by many ethnic communities when accessing mental health services.
Through an A–R alphabet structure, this poem highlights why the Patient and Carer Race Equality Framework (PCREF) matters and why genuine cultural understanding, listening, and inclusion are essential to improving care.
This poem is part of my 200-poem PCREF collection, Unpaid, Unseen and Yet Unbroken, giving voice to the experiences of unpaid carers supporting relatives with mental illness while challenging racial inequalities across mental health services.
By Matthew McKenzie – Chair of the South London MH carers forum
Another month has passed, and I would like to thank everyone who joined our South London Mental Health Carers Forum. It was fantastic to welcome carers, NHS professionals, voluntary sector organisations and local authority representatives from across South London to discuss issues affecting unpaid mental health carers.
As always, the forum provides a safe place where carers can raise concerns directly with decision makers, hear about new developments, share experiences and help shape improvements across mental health services.
For those who were unable to attend, here is a detailed summary of the meeting.
Welcome and introductions
We welcomed carers from across Lewisham, Lambeth, Southwark, Croydon, Richmond and surrounding boroughs, alongside representatives from:
Lewisham GP Mental Health Transformation
Carers First Croydon
Carers Hub Lambeth
POWHER (NHS complaints advocacy)
Southwark Council
Carers with lived experience
Voluntary sector organisations
The strength of the forum continues to be its mix of lived experience alongside professionals willing to listen directly to carers.
One particularly encouraging update at the beginning of the meeting was confirmation that South London and Maudsley NHS Foundation Trust (SLaM) is reviewing its Triangle of Care work and wishes to involve carers more closely in that process.
This is extremely important because Triangle of Care is one of the main national frameworks that helps mental health services work better with families and unpaid carers.
Lewisham Mental Health Transformation Update
Our first guest speaker was Dr Anna Robinson, GP Clinical Lead for Mental Health Transformation in Lewisham.
Dr Robinson explained that one of her main priorities is improving communication between GP practices and specialist mental health services. She recognised that many of the difficulties experienced by carers occur during transitions, particularly when someone moves between primary care and secondary mental health services. To help address this, she has already begun bringing together GP leaders and mental health professionals, creating opportunities for closer collaboration and establishing direct communication channels, including a new WhatsApp group linking GPs with mental health clinicians so concerns can be discussed more rapidly. She hopes these improvements will lead to better referral pathways, clearer discharge arrangements and more consistent communication between services.
Improving communication between GPs and mental health services
One of the biggest priorities is improving communication between GP practices and specialist mental health services.
Many carers know only too well how stressful it can be when someone is discharged from secondary mental health care back to their GP.
Communication delays often create uncertainty about:
medication
follow-up care
relapse planning
physical health monitoring
who is actually responsible for ongoing care
To improve this, Lewisham has already begun bringing together GPs and mental health clinicians, including establishing direct communication channels so problems can be discussed much more quickly.
This was welcomed by carers, although many explained there remains considerable work to do.
Carers’ biggest concern: discharge back to GPs
This became the largest discussion of the afternoon.
Many carers expressed anxiety about people with severe mental illness being discharged from community mental health teams back to primary care.
Some of the concerns raised included:
GPs may not know the patient as well as specialist teams.
Carers worry relapses may not be identified quickly enough.
Missed appointments are sometimes an early warning sign rather than a sign that someone is well.
Some medications require specialist monitoring.
Communication between services is still inconsistent.
One carer explained that if someone experiencing psychosis fails to attend appointments, it should trigger concern rather than assumptions that everything is fine.
Another highlighted that patients can sometimes cancel appointments themselves, meaning clinicians may never realise there is actually a developing crisis.
Dr Robinson acknowledged these concerns and confirmed they are exactly the type of issues she wishes to improve through stronger collaboration between GP practices and specialist services.
Early identification of mental illness in schools
Another important discussion focused on children and young people.
One parent shared how concerns about their child’s mental health had been dismissed at school months before a serious psychotic episode eventually occurred.
This led to discussion about whether all school staff should receive training to recognise early signs of serious mental illness as part of safeguarding training.
Dr Robinson explained that Lewisham is expanding mental health support teams in schools and is also developing alternative services for young people because traditional CAMHS services remain under enormous pressure.
The discussion highlighted how earlier recognition may prevent future crises for some young people.
Universal Care Plans and identifying carers
During the discussion I raised the growing use of the Universal Care Plan (UCP) across London.
One area we discussed was whether GP surgeries are identifying unpaid carers more effectively.
Many carers are still not recorded as carers within GP systems, meaning they may miss out on:
health checks
vaccinations
support services
referrals
carers’ information
Dr Robinson confirmed GP systems can record carers through coding, but acknowledged this often depends upon carers identifying themselves.
This remains an important challenge because many people caring for relatives still do not think of themselves as “carers.”
Better identification continues to be essential if carers are to receive the support they deserve.
The discussion also broadened into medication safety, the role of GPs in supporting people with long-term mental health conditions and the identification of unpaid carers within GP practices. A carer shared her own lived experience of being misdiagnosed and suffering severe adverse reactions to medication before eventually receiving the correct diagnosis and treatment. Dr Robinson acknowledged that medication can sometimes initially worsen symptoms and stressed the importance of clinicians discussing potential side effects openly with patients.
As I raised questions about the rollout of Universal Care Plans and whether GP surgeries are preparing to identify carers more effectively through SNOMED coding and improved care planning. Dr Robinson explained that GP systems can record carers, although this often depends upon carers identifying themselves, and recognised that many people providing substantial care still do not see themselves as carers. The discussion reinforced the importance of improving carer identification, strengthening communication between services and ensuring carers are recognised as genuine partners in care rather than remaining invisible within the healthcare system
Carers First Croydon
Our second presentation came from Carers First, the organisation delivering carers’ services across Croydon.
Jessica and Toby introduced their service and explained how they are developing support specifically for unpaid carers, including those caring for someone with mental illness.
Although their service supports all carers, they recognised that mental health carers often experience unique challenges.
These include:
confidentiality barriers
crisis situations
unpredictable relapses
emotional exhaustion
isolation
uncertainty around care planning
Their presentation showed a genuine understanding of the pressures faced by mental health carers.
I agree. For a blog, that section reads more like meeting notes than an article. Here’s a much smoother narrative version that still captures the main points without relying on long bullet lists.
Carers First Croydon: Supporting Carers Before Crisis
The organisation commissioned by Croydon Council to provide support for unpaid carers across the borough. Jessica and Toby introduced the service and explained how they are working to ensure carers receive support much earlier in their caring journey, rather than only when they reach crisis point. Although the organisation supports carers of all ages and caring situations, they recognised that those caring for someone with mental ill health often face unique challenges, including emotional exhaustion, confidentiality issues, unpredictable relapses and the constant uncertainty that can accompany serious mental illness.
A key message throughout the presentation was that support for carers needs to be holistic. Carers First offers statutory carers assessments, practical advice, emotional support, peer support and wellbeing activities, but these conversations extend far beyond simply discussing the caring role. Staff work with carers to understand the wider impact that caring has on everyday life, including issues such as employment, finances, poor sleep, housing difficulties, physical health and emotional wellbeing. The aim is to identify the pressures that make caring more difficult and then work alongside carers to find practical solutions, whether through grants, referrals to other organisations, respite opportunities or local wellbeing services.
The presenters emphasised that many carers wait too long before asking for help, often believing they should simply cope on their own. By the time support is requested, carers may already be physically and emotionally exhausted. Carers First hopes to change this by encouraging earlier referrals from GPs, mental health services and carers themselves, allowing support to be put in place before problems become overwhelming. The earlier carers receive advice and practical assistance, the more likely they are to maintain both their own wellbeing and their ability to continue caring.
There was also a strong focus on carers’ own health and wellbeing. The presenters spoke about activities such as carers cafés, Qigong sessions, volunteering opportunities and wellbeing programmes, not simply as recreational activities, but as an essential part of sustaining carers over the long term. One particularly powerful message from the presentation was that self-care should never be viewed as a luxury or something to feel guilty about. Instead, looking after carers is fundamental to maintaining safe, sustainable caring relationships. By supporting carers emotionally, socially and practically, organisations like Carers First help ensure that carers themselves remain healthy enough to continue supporting the people who rely upon them.
Southwark Council Engagement: Safeguarding Review
Later in the meeting we welcomed representatives from Southwark Council, who attended to discuss the council’s current review of safeguarding arrangements and, importantly, to hear directly from carers about their experiences. The discussion recognised that safeguarding is not simply about responding to abuse or neglect, but about ensuring that people with mental health needs receive safe, person-centred care while families and carers are appropriately involved throughout the process.
The review aims to strengthen safeguarding by making it:
More consistent across services.
More proportionate to individual circumstances.
More person-centred and focused on outcomes.
Better at involving families and carers where appropriate.
More responsive to concerns raised by people with lived experience.
Council representatives emphasised that this was not simply a consultation exercise but an opportunity for carers to genuinely influence how safeguarding develops in Southwark. Those attending the forum were encouraged to continue sharing their experiences so that future improvements are informed by the realities of supporting someone with mental illness.
Questions and discussion
The discussion that followed highlighted a number of recurring themes experienced by carers across South London.
Several carers explained that they often recognise subtle changes in a person’s behaviour weeks before professionals become aware that something is wrong. As the people who know their relative best, carers felt that their observations should be taken more seriously when concerns are first raised, particularly where there is evidence of deteriorating mental health or increasing risks.
Questions were also raised around how safeguarding concerns are assessed and whether professionals always communicate effectively with families once a concern has been reported. Some carers described occasions where they were uncertain about what action had been taken, what the next steps were, or whether their concerns had been fully understood.
There was also discussion about balancing confidentiality with safeguarding responsibilities. Whilst recognising the importance of protecting an individual’s rights, carers emphasised that excluding families from conversations can sometimes mean valuable information about risks, changes in behaviour or previous crises is overlooked. Many felt that better communication with carers could strengthen safeguarding rather than compromise it.
Another important point raised was that safeguarding should not only focus on responding after a crisis has occurred. Instead, carers felt services should recognise early warning signs, intervene sooner where possible and view carers as partners in identifying emerging risks before situations escalate.
The representatives welcomed these reflections and acknowledged the value of hearing directly from lived experience. They encouraged carers to continue engaging with the review process so that future safeguarding arrangements better reflect the realities faced by families supporting someone with serious mental illness.
Lambeth Update
We were also pleased to receive an update from Karen Ibrahim, Mental Health Carers Coordinator at Carers Hub Lambeth, who shared a number of developments taking place across the borough to improve support for unpaid carers.
Karen explained that Carers Hub continues to expand its offer to carers, with several new initiatives now available. One of the most significant developments is the introduction of the Lambeth Carers Card, which is intended to help carers identify themselves more easily when accessing services and encourage wider recognition of the vital role unpaid carers play. Alongside this, Carers Hub has strengthened its welfare benefits support, enabling carers to access specialist advice on benefits, financial entitlements and income maximisation, an increasingly important service given the financial pressures many carers continue to face.
Another important area of work has been raising awareness of carers throughout local services. Karen described the continued delivery of carers awareness training for professionals, helping frontline staff better understand carers’ rights, the challenges families experience and why carers should be recognised as partners in care rather than simply relatives accompanying patients. She also highlighted the ongoing development of the Lambeth Mental Health Carers Group, which continues to provide carers with opportunities to share experiences, influence local services and receive peer support from others who understand the realities of caring for someone living with mental illness.
Questions and discussion
The discussion then moved towards some of the more difficult experiences carers continue to face within inpatient mental health services.
One issue raised was the safety of inpatient wards, with concerns expressed about incidents involving patient-on-patient violence and the emotional impact these situations can have on both patients and their families. Carers discussed the importance of ensuring that safety concerns are taken seriously and that families are kept appropriately informed when incidents occur.
Questions were also asked about how carers’ concerns are escalated when they believe someone is at risk or when communication between staff and families begins to break down. Karen acknowledged that these situations can be extremely distressing for carers and stressed the importance of maintaining open communication between inpatient teams, community services and families wherever possible.
The discussion also reinforced the wider importance of involving carers throughout a person’s mental health journey, rather than only contacting families during periods of crisis. Participants agreed that carers often hold valuable knowledge about changes in behaviour, early warning signs and previous experiences of relapse, and that this lived experience should be recognised as an important contribution to safe and effective care.
Karen thanked carers for continuing to share their experiences and encouraged everyone to remain engaged with Carers Hub Lambeth, emphasising that feedback from carers plays a vital role in helping improve local mental health services and ensuring carers’ voices continue to influence future developments.
Looking ahead
Our forum will continue bringing together carers, NHS services, local authorities and voluntary organisations to improve mental health support across South London.
If you are an unpaid mental health carer living in South London, you are always welcome to join us.
Together we can continue raising carers’ voices, influencing services and helping ensure that carers are recognised not simply as visitors to mental health services, but as valued partners in care.
By Matthew McKenzie – Chair of ethnic mental health carer forum.
For my latest spoken word video, “Today I Prayed,” I present a piece from my PCREF poetry collection that I am working on, Unpaid, Unseen and Yet Unbroken.
Grounded in the spirit of the Patient Carer Race Equality Framework (PCREF), this poem centers on the often hidden realities faced by unpaid Black mental health carers.
The poem explores spirituality not just as a source of private comfort and endurance, but as a solitary lifeline when formal systems fail and the heavy emotional weight of duty takes its toll.
I think watching this video is an invitation to witness the quiet strength of minority carers, plus raise awareness of systemic gaps in our care frameworks.
I hope the poem ensures that these vital carer voices are finally seen, heard, and respected.
By Matthew McKenzie – Chair of Carers Hospital Discharge group
Thanks to everyone who attended our July Hospital Carer Discharge Meeting. We welcomed representatives from NHS trusts, local authorities, carers organisations, Healthwatch, and voluntary sector partners from across London. As always, the purpose of the meeting was to share developments, learn from each other’s work, and strengthen collaboration to improve hospital experiences and discharge planning for unpaid carers.
Although every organisation is at a different stage of development, one message came through very clearly: supporting unpaid carers is becoming an increasingly important priority across hospitals, councils and the NHS.
A Strong Focus on Earlier Carer Identification
One of the recurring themes throughout the meeting was the importance of identifying carers as early as possible during a patient’s hospital journey.
Many hospitals continue to recognise that carers are often identified too late—sometimes only when discharge is already taking place. Earlier identification allows staff to:
involve carers in care planning
understand the practical support available at home
recognise carers’ own support needs
prevent unsafe or delayed discharges
improve communication between hospital teams and families.
Lewisham & Greenwich NHS Trust provided an update on its Standard Operating Procedure (SOP) designed to improve the identification and involvement of unpaid carers. Although implementation has been delayed because of competing organisational priorities, the framework remains in place and includes:
earlier identification of carers on admission
recording carers within hospital systems
involving carers in discharge planning
ensuring carers understand care needs following discharge
connecting carers with local authority assessments and community support.
Alongside this, the Trust continues reviewing its Carers Charter and strengthening relationships with voluntary organisations across Lewisham, Greenwich and Bexley to improve partnership working. Training for ward staff is also beginning with support from local councils to improve awareness of carers and available services.
This demonstrates that improving hospital discharge is not simply about creating new policies, but embedding carer awareness throughout everyday clinical practice.
Excellent Examples of Partnership Working
Several organisations shared encouraging examples of collaboration across health and social care.
The North Central London Carer Support Project described a wide range of initiatives already underway across several NHS trusts.
These include:
weekly co-delivered carer awareness sessions with Camden Carers at University College London Hospital
regular online training sessions at Whittington Hospital attracting around forty staff members each session
development of an e-learning programme for professionals working with carers
greater involvement of patient experience teams in monitoring referrals to carers organisations.
Particularly encouraging was the decision to begin monitoring hospital referral numbers to carers organisations as a performance measure. Measuring referrals each month provides a practical way of understanding whether carers are actually being identified and connected to support rather than relying solely on policy documents.
Camden Carers also highlighted continued outreach into GP surgeries through dedicated engagement work, recognising that many carers first come into contact with primary care long before hospital admission.
Learning from Cancer Carers
Healthwatch representatives shared plans for a significant research project exploring the experiences of carers supporting someone with cancer. The study is expected to begin later this year and will gather the views of carers across several London boroughs before producing recommendations for NHS trusts and publishing the findings publicly. The aim is to better understand what is working well for carers, where support can be strengthened, and how healthcare services can respond more effectively to the realities faced by those caring for someone undergoing cancer treatment.
The discussion highlighted the importance of ensuring that the voices of unpaid carers are heard throughout the research process. Caring for someone with cancer can involve navigating complex treatment pathways, managing appointments across multiple services, providing emotional support, and balancing caring responsibilities alongside work and family life. Research such as this provides an opportunity to capture those lived experiences and translate them into practical recommendations that can improve communication, discharge planning, access to information, and the support available to carers across NHS services.
As Chair of the Cancer Caregiver Forum, I also highlighted opportunities for researchers and NHS organisations to work more closely with existing cancer carer networks to ensure lived experience remains central to future improvements.
Hospital Discharge Remains a National Priority
Several organisations reflected on how hospital discharge continues to be one of the biggest concerns raised by unpaid carers.
Chelsea and Westminster Hospital NHS Foundation Trust
Chelsea and Westminster Hospital explained that feedback from carers is regularly discussed through its Patient Experience Group, with hospital discharge continuing to be one of the most common issues raised by families. Representatives acknowledged that while significant work has taken place, there remains more to do to ensure carers are consistently recognised, listened to, and involved throughout a patient’s stay in hospital.
The Trust also highlighted the important role that carers play in shaping future improvements. By regularly hearing directly from carers through patient experience forums, the hospital is building a better understanding of the practical challenges families face before, during and after discharge. Although their Carers Lead was unable to attend this meeting, the Trust expressed a strong commitment to continuing engagement with regional partners and learning from initiatives taking place across London to strengthen discharge planning and carer support.
Richmond Carers Centre
Richmond Carers Centre reported strong referral links with Kingston Hospital, particularly through dementia services, while also developing opportunities for joint education sessions where hospital staff and carers can better understand each other’s experiences of discharge planning.
Alongside its close working relationship with Kingston Hospital, Richmond Carers Centre continues to raise professional awareness across the borough, encouraging more organisations to identify unpaid carers and refer them for support. The team reflected on ideas gathered from national conferences, including improving engagement with diverse communities and strengthening links with GP practices and Primary Care Networks. Although capacity remains a challenge, Richmond Carers Centre continues to explore new ways of increasing visibility so that carers receive information, advice and emotional support as early as possible rather than only after a hospital discharge has taken place.
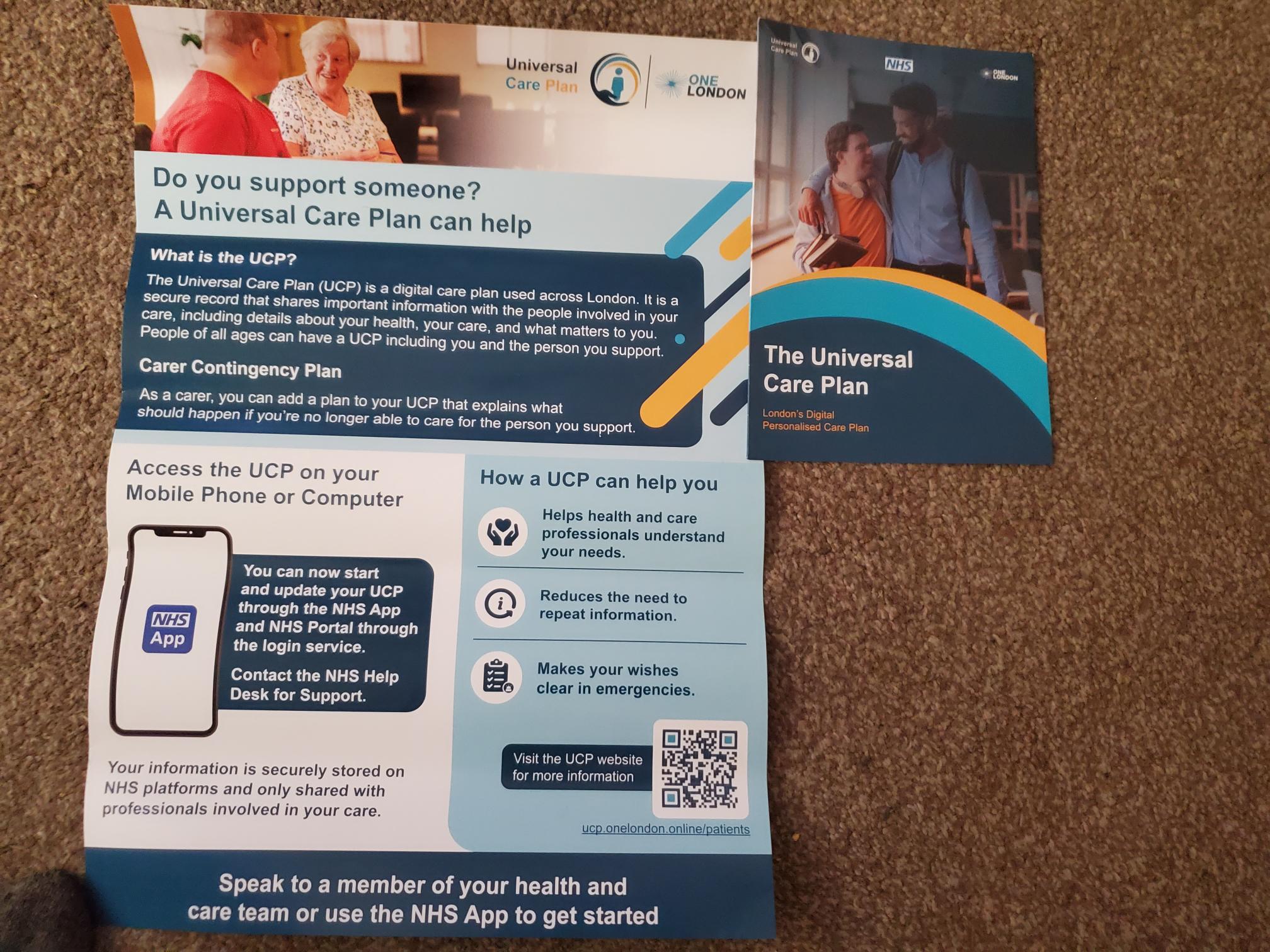
Universal Care Plan and Care Contingency Plan (UCP/CCP)
An important update was shared regarding the Universal Care Plan (UCP) and Care Contingency Plan (CCP), which are being developed through NHS England to improve how carers are identified and supported across health services. Attendees heard that the programme is currently being piloted in London and aims to allow unpaid carers to record emergency contingency arrangements and important caring information digitally through the NHS App and GP systems. The long-term ambition is for this information to be accessible across different parts of the NHS, helping professionals better understand both the needs of the person receiving care and the vital role played by their unpaid carer. Representatives who attended the recent NHS England workshop described the programme as a positive and promising development, with training opportunities expected to become available as the rollout progresses.
The discussion also highlighted that increasing awareness will be just as important as the technology itself. Many carers remain unaware that care planning and contingency planning can help prepare for emergencies where they may suddenly be unable to provide care. By encouraging hospitals, GP practices and carers organisations to promote the Universal Care Plan and Care Contingency Plan, there is an opportunity to improve continuity of care, reduce avoidable crises, and ensure that carers’ knowledge and wishes are better recognised within the wider health and care system. As these initiatives develop, organisations across London will have an important role in helping carers understand how to access and make effective use of these new digital planning tools.
Southwark Council
Southwark Council also described ongoing partnership work with Guy’s & St Thomas’ and King’s College Hospital. King’s College Hospital is currently developing a Care and Support Navigator service designed to support patients while they remain on waiting lists, assist with discharge planning, and improve signposting into community services once patients return home.
The Council explained that while its refreshed Carers Strategy is not solely focused on hospital discharge, close partnership working with local NHS trusts remains a key priority. Through the Southwark Carer Collaborative, which meets quarterly with representatives from King’s College Hospital and Guy’s & St Thomas’, organisations are sharing developments, identifying opportunities for joint working, and ensuring carers remain firmly on the agenda. Southwark also confirmed that the newly launched Cross-Government Unpaid Carers Action Plan is already helping to inform the direction of its refreshed strategy, demonstrating how national policy is beginning to influence local planning and partnership working.
National Developments – A Significant Moment for Unpaid Carers
Perhaps the most significant national development discussed during the meeting was the publication of the UK Government’s first Cross-Departmental Unpaid Carers Action Plan, launched on early July.
Although many details will continue developing over the coming months, the plan represents an important step because responsibility for unpaid carers is now being considered across multiple government departments rather than solely within health and social care.
Key priorities include:
improving identification of unpaid carers
increasing referrals into carers support services
strengthening employment support for working carers
making greater use of digital systems including the NHS App.
Alongside this sits the development of the Universal Care Plan and Carers Contingency Plan. Early pilots suggest these tools could allow carers to record emergency contingency arrangements and important caring information digitally, making that information more accessible across health services when needed. Training opportunities are expected to become available as the programme expands.
Looking Ahead
Although considerable progress is being made, many of the discussions reinforced that improving hospital discharge requires sustained partnership between NHS trusts, councils, carers organisations and, most importantly, unpaid carers themselves.
Future meetings will continue sharing practical examples of good practice, highlighting successful projects, and identifying opportunities for organisations to learn from one another.
At our September meeting we look forward to welcoming Carers UK, who will provide regarding hospitals and unpaid carers.
Thank you once again to everyone who contributed to the July meeting. Your willingness to share ideas, successes and challenges continues to strengthen our collective efforts to ensure unpaid carers are recognised, valued and fully involved throughout the hospital discharge process.
By Matthew McKenzie – Carers UK ambassador / Chair of National ethnic mental health carers forum
Are you a Black unpaid carer supporting a family member with a learning disability (sometimes referred to as an intellectual disability) who has experienced mental health difficulties?
Have you ever tried to access mental health support on their behalf? This could include contacting services such as Community Learning Disability Teams, CAMHS, Community Mental Health Teams, Talking Therapies or other mental health services.
If so, your experiences matter.
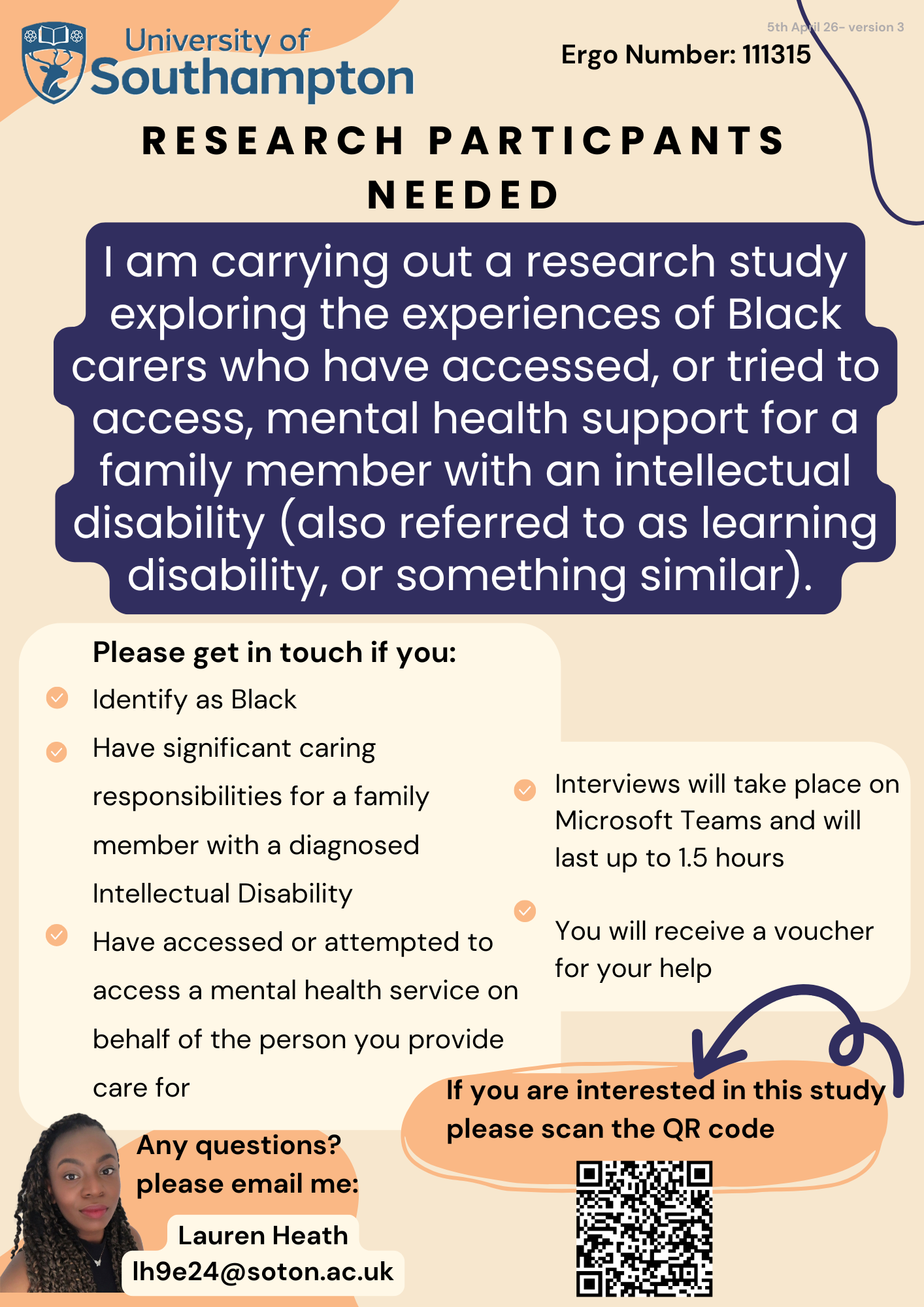
Lauren Heath, a second-year Trainee Clinical Psychologist at the University of Southampton, is conducting doctoral research exploring the experiences of Black carers who have accessed, or attempted to access, mental health support for a family member with a diagnosed learning disability.
We know that Black unpaid carers often face additional challenges when trying to navigate health and social care systems. Too often, their experiences are unheard or underrepresented in research. This study aims to better understand those experiences and help inform more culturally sensitive and inclusive services in the future.
You may be eligible to take part if you:
Identify as Black.
Have significant caring responsibilities for a family member with a diagnosed learning disability (or intellectual disability).
Have accessed, or attempted to access, mental health services on their behalf.
Taking part will involve:
A confidential interview lasting approximately 1.5 hours via Microsoft Teams.
Your responses will be anonymised once all interviews have been completed.
You will receive a voucher to thank you for your time and contribution.
Lauren previously worked within Community Learning Disability Teams across the UK and became interested in understanding why so few Black families appeared to be accessing these services. Her doctoral research hopes to amplify the voices of Black carers and contribute towards improving culturally sensitive support for families in the future.
If you think this research may apply to you, or someone you know, please consider taking part or sharing this opportunity within your networks.
To find out if you are eligible, you can complete the short questionnaire or contact Lauren directly at L.Heath@soton.ac.uk.
Your lived experience could help shape future services for Black families and carers.
By Matthew McKenzie – Triangle of Care – Community group chair
Putting Carers at the Centre of Care
The latest Triangle of Care Community Group brought together carers, professionals and partner organisations from across England to share learning, celebrate progress and identify where further improvements are needed. The meeting highlighted the growing influence of the Triangle of Care across mental health and acute services, whilst reinforcing that there is still much work to do to ensure carers are consistently recognised, valued and supported.
One of the most powerful aspects of the meeting was hearing directly from carers about their experiences. Whilst many spoke positively about the progress that has been made over recent years, there was a shared view that carer involvement remains inconsistent across services. Carers described feeling more included than ever before, with greater awareness of the Triangle of Care principles and more opportunities to participate in steering groups, service developments and community discussions. However, concerns remain around automatic carer identification, information sharing and ensuring that carers are genuinely recognised as partners in care.
Several carers reflected on the importance of having their voices heard early in a patient’s care journey. Examples were shared of services introducing carer contribution templates that ensure family members are involved within 72 hours of admission, whilst others highlighted improvements to confidentiality processes that allow patients to determine what information can be shared with carers at different stages of their recovery. These practical changes demonstrate how relatively small adjustments can have a significant impact on relationships between carers, patients and professionals.
Progress Across the Triangle of Care Programme
Mary Patel, Triangle of Care Programme Lead at Carers Trust, provided an update on developments across the national programme. The Triangle of Care continues to grow, with a number of organisations progressing through the STAR accreditation process and demonstrating their commitment to embedding carer-inclusive practice across services.
Importantly, members were reminded that the STAR awards are not designed to rank organisations, but instead reflect the breadth of implementation across different service areas. STAR I focuses primarily on inpatient and crisis services, STAR II expands into community services, whilst STAR III recognises organisations delivering integrated services across multiple clinical areas.
Several trusts have recently achieved STAR awards, whilst others are progressing through the assessment process over the coming months. The programme’s peer review approach continues to ensure that carers remain central to the assessment process, with carers actively involved in reviewing evidence, identifying good practice and making recommendations for future development.
The Triangle of Care Member Hub continues to provide valuable opportunities for peer learning, resource sharing and collaborative working. Upcoming webinars will include sessions exploring Open Dialogue approaches developed by Devon Partnership NHS Trust, providing members with further opportunities to learn about therapeutic models that place families and carers at the heart of care planning.
Advancing Equality Through the Patient and Carer Race Equality Framework
A significant development announced during the meeting was the launch of Phase Two of the Triangle of Care and Patient and Carer Race Equality Framework (PCREF) project.
PCREF represents the first mandatory anti-racism framework within mental health services in England. Recognising that carers from racially marginalised communities often experience poorer outcomes and face additional barriers when accessing support, the Triangle of Care programme has been working collaboratively with carers and mental health providers to strengthen the way services assess and respond to carers’ needs.
The revised self-assessment framework encourages services to move beyond assumptions and adopt a more professionally curious approach to understanding carers’ individual experiences. Rather than viewing carers as a homogenous group, the framework recognises that caring experiences are shaped by culture, identity, language, personal circumstances and wider health inequalities.
Pilot sites from across England are now testing the revised guidance, with learning being shared nationally throughout the project. Importantly, organisations do not need to be participating in the pilot to begin implementing the principles and learning that emerge from this work.
Alongside PCREF, Carers Trust continues to contribute to national policy developments, including the Modern Service Framework for Severe Mental Illness and the forthcoming Mental Health Strategy for England. Throughout these discussions, there has been a consistent message that carers must be recognised as partners in care and have access to appropriate support in their own right.
Confidentiality, Information Sharing and Carer Inclusion
Confidentiality remained one of the most prominent themes throughout the meeting. Whilst participants acknowledged the importance of protecting patients’ rights and preferences, carers highlighted that confidentiality can sometimes become a barrier to meaningful engagement.
Several contributors reflected that confidentiality should never prevent professionals from listening to carers’ concerns or receiving valuable information that may support a patient’s care. Others spoke about the importance of revisiting conversations around consent over time, recognising that patients’ preferences may change as their circumstances and wellbeing improve.
Practical examples of good practice included breaking confidentiality discussions down into specific areas, allowing patients to decide what information can be shared about medication, activities, wellbeing and treatment plans, rather than relying on simple ‘yes or no’ decisions. There was also discussion around the importance of staff training to improve confidence when navigating complex conversations around confidentiality and information sharing.
Participants agreed that carers should never be expected to provide significant levels of support without receiving the information necessary to do so safely and effectively. Achieving the right balance between confidentiality and partnership working remains an important priority for the Triangle of Care community.
Triangle of Care Principles Within Acute Services
The meeting concluded with an inspiring presentation from Wendy Doyle, Head of Patient Experience at St George’s University Hospitals NHS Foundation Trust and Epsom and St Helier Hospitals, exploring how Triangle of Care principles can be successfully implemented within acute hospital settings.
Whilst the Triangle of Care originated within mental health services, Wendy demonstrated that its principles are equally applicable across acute care environments. Her organisation supports approximately 19,000 members of staff across multiple hospital sites and has developed a comprehensive approach to identifying, recording and supporting unpaid carers.
Staff are encouraged to identify carers at the earliest possible opportunity, with this information recorded within patient records to ensure continuity throughout the patient’s hospital journey. Comprehensive carer awareness training is delivered through virtual sessions, ward-based education and e-learning resources, helping staff understand both the practical and emotional importance of recognising carers.
Importantly, identifying carers is only the beginning of the process. Every carer recorded within the hospital system receives a follow-up wellbeing check from the Patient Experience Team to discuss their own support needs, identify any challenges and facilitate referrals to local carers’ organisations where appropriate.
Partnership working sits at the heart of this approach, with close collaboration between acute services and local carers’ centres ensuring carers can access a broad range of practical and emotional support. Adult and Young Carers’ Charters have also been co-produced with carers themselves, helping to shape organisational commitments around kindness, inclusion and meaningful engagement.
Perhaps most importantly, Wendy highlighted that supporting carers improves outcomes for everyone. Better communication strengthens discharge planning, reduces avoidable hospital admissions and readmissions, improves patient safety and helps prevent carer burnout. Acute hospital stays can provide valuable opportunities to identify carers who may previously have remained invisible and connect them with longer-term support.
Looking Ahead
The discussions throughout the meeting demonstrated both the progress that has been made and the challenges that remain. There is increasing recognition that carers are essential partners in delivering high-quality care across both mental health and acute services. However, meaningful involvement cannot rely upon individual goodwill alone; it requires consistent systems, robust policies and a genuine commitment to partnership working.
Looking ahead, the Triangle of Care programme will continue to expand opportunities for peer learning, influence national policy developments and support organisations to embed carer-inclusive practices across services. The ongoing work around PCREF and wider mental health policy developments provide important opportunities to ensure that carers’ voices remain central to future service transformation.
Above all, the meeting reinforced a simple but powerful message: carers must not be viewed as an afterthought or an optional addition to care planning. They are experts through experience, invaluable partners in care and individuals with support needs of their own. When carers are identified early, listened to meaningfully and supported appropriately, outcomes improve not only for carers themselves, but for patients, families and services alike.
The Triangle of Care Community Group continues to provide an important space where carers and professionals can learn from one another, challenge existing practices and work collectively towards more compassionate, inclusive and effective care.
By Matthew McKenzie – NHS England involvement, Chair of National ethnic mental health carer forum
As carers, your voices are the most powerful tools we have to change how healthcare is delivered. Every day, you navigate complex systems to support your loved ones, seeing firsthand what works and crucially where the gaps are.
Right now, NHS England’s Office of the Chief Allied Health Professions Officer (CAHPO) is developing its next big strategy: The AHP Framework for System Impact for England (2027–2032). Because this strategy is built on the core values of anti-racism, co-production, and sustainability, it is absolutely vital that ethnic minority mental health carers are at the center of this conversation.
What is an AHP and Why Do They Matter to You?
Allied Health Professionals (AHPs) make up the third-largest workforce in the NHS. They aren’t doctors or nurses, but they are the specialists who focus on recovery, independence, and keeping people healthy.
There are 14 distinct AHP roles, many of which are essential in mental health and holistic care, including:
Art, Drama, and Music Therapists: Helping individuals express and process complex feelings.
Occupational Therapists: Supporting people to regain life skills and independence.
Dietitians & Physiotherapists: Improving physical health, nutrition, and mobility, which heavily impact mental wellbeing.
Speech and Language Therapists: Assisting those with communication or swallowing difficulties.
The new 2027–2032 framework will dictate how these professionals operate, how easily you can access them, and how they support families over the next five years.
The Six Key Pillars of the New Strategy
The NHS is currently running a national consultation (open until 18th September 2026) to find out what matters most to patients and carers. They want to hear your views across six key areas:
Pillar
What it means for Carers
1. Safe, High-Quality & Accessible Services
Ensuring your loved ones get the right care, quickly and safely, without facing unfair barriers.
2. Keeping People Healthy
Shifting the focus toward prevention and early support before a crisis hits.
3. People and AHP Workforce
Building a skilled, inclusive, and culturally competent workforce that understands diverse communities.
4. Working Differently
Delivering care in more appropriate, comfortable settings—like community centers or at home.
5. Research, Improvement & Innovation
Turning real-world evidence and carer experiences into better everyday medical practice.
6. Data, Digital & Technology
Using digital tools and tech wisely to improve care access without leaving people behind.
Have Your Say: Join Our National Ethnic Mental Health Carers Forum
We have a massive opportunity to speak directly to the people writing this strategy. You are warmly invited to join our upcoming virtual forum to share your experiences, learn about groundbreaking new carer research, and hold a direct Q&A with NHS leadership.
Event Details:
Date: Friday, July 31st
Time: 10:30 AM BST Start
Platform: Zoom
You can also feed back on the strategy using the QR code
What’s on the Agenda for National Ethnic MH carer forum July 31st?
Our packed morning features incredible advocates and policy makers who want to hear from you:
10:35 AM | Local Carer Insights:Dr. Ida Doherty (King’s College London) will present vital new research on supporting ethnic carers in South West London.
10:45 AM | Health Equality Focus: A special guest segment featuring Ruby Neish (UCL) discussing healthcare experiences regarding cancer and Black women.
11:00 AM | Direct NHS England Engagement: Steve Tolan (Deputy Chief AHP Officer) and Barry O’Donovan (Senior Programme Manager, NHS England) will join us to discuss the new strategy and listen to your feedback.
11:20 AM | Mental Health Trust Updates: Real-world updates from local mental health trusts, including insights from Linda Thomas from West London NHS trust
11:40 AM onwards | Regional Perspectives & Systems Change: Discussions with Julia G. (Carers East Kent), the Carers West Sussex study team, and Bren McInerney representing the Race Equality Observatory.
Your Voice is the Missing Piece: If we want an NHS that is truly anti-racist, co-produced, and accessible, we have to show up and speak up. This forum is a safe, supportive space designed to amplify your lived experiences.
How to Join: Please check your email for the secure Zoom link, or visit the link below. We look forward to seeing you there on July 31st at 10:30 AM!
By Matthew McKenzie – Carer and Carers UK Ambassador
As unpaid carers, many of us know what it feels like to operate in the background. We juggle complex health systems, care for our loved ones, and manage our own lives, all too often feeling invisible.
That is why I am excited to share a major milestone for our community.
The Department of Health and Social Care (DHSC), alongside the Departments for Education, Business and Trade, and Work and Pensions has officially launched the Unpaid Carers Action Plan: Recognize, Refer, Reach.
This is England’s first-ever cross-government action plan dedicated entirely to supporting unpaid carers.
I was honored to attend the official launch event to represent our community, meet with Minister for Care Stephen Kinnock MP, and participate in the official DHSC launch video.
This isn’t just another policy document; it is a commitment across multiple government sectors to drive real, practical change.
The plan is built around three core pillars:
1. Recognise
Carers must be identified early. One of the most exciting digital updates is a new “MyCarer” section being introduced on the NHS App, allowing us to easily register our caring role so healthcare staff know who we are from the start.
2. Refer
No carer should have to navigate the system alone. This pillar focuses on making sure we are directed to local carer centres, financial advice, and emotional support early on. Crucially, it aims to ensure we are formally included in major healthcare decisions, like hospital discharge planning.
3. Reach
Caring shouldn’t mean giving up on your own future. For working carers, the plan explores paid carer’s leave and will require large employers (250+ staff) to publish carer support plans from spring 2027. For young carers, it means stronger support within schools so their education doesn’t suffer.
A Message to My Fellow Carers and Carer Centres
For years, we have argued that caring is not just a “health” issue, it impacts our jobs, our education, our finances, and our mental health. Seeing four government departments finally come together to address I feel is a massive step forward.
To my fellow unpaid carers: Please know that using your voice gives you a chance at being heard. It is important to get carers “on the map” to be recognised, and this plan is a direct result of carers sharing their lived experiences.
To Carer Centres and Forums: This action plan is a powerful tool for us. It gives us a framework to hold local services accountable and ensure the “Recognise, Refer, Reach” goals are delivered on the ground.
Of course change doesn’t happen overnight, but this plan gives us a vital foundation to build on. Let’s keep pushing, keep connecting, and make sure every single unpaid carer gets the recognition and support they deserve.