
Welcome to the July 2021 update of my Lewisham mental health carers forum. The forum focuses on engagement for families and unpaid carers who care for someone suffering mental ill health. The ‘cared for’ does not actually have to be using mental health services, but it is important there is a platform for unpaid carers to learn about mental health support, understanding mental health and what is available for carers themselves.
Speakers for my July carers forum were:
Phoebe Averill – PHd Student at Kings College
Polly Pascoe – Lewisham CCG
Carla Fourie – SL&M director of social care
- Phoebe Averill presents on her latest study.
First to speak was Phoebe Averill who is a PhD student at King’s College. She is working with South London & Maudsley NHS Trust (SL&M) on a research study and she wants to hear carer member’s thoughts and also invite anyone that might be interested in taking part in the research study. She is looking at safety of care in the community mental health services. Phoebe gave my forum a bit of background information about what the problem is. Basically safety in general hasn’t really been given much attention in mental health services. Historically, when you compare it to kind of physical health care services, where we’ve now got quite a good idea about how we can make care safer, what types of interventions and strategies might be needed. Still, there is a small kind of body of research and interventions coming out more recently. These are mainly focused on inpatient mental health services and unfortunately community mental health services have been a little bit left behind, even though that’s where the majority of people who are actually receiving care.
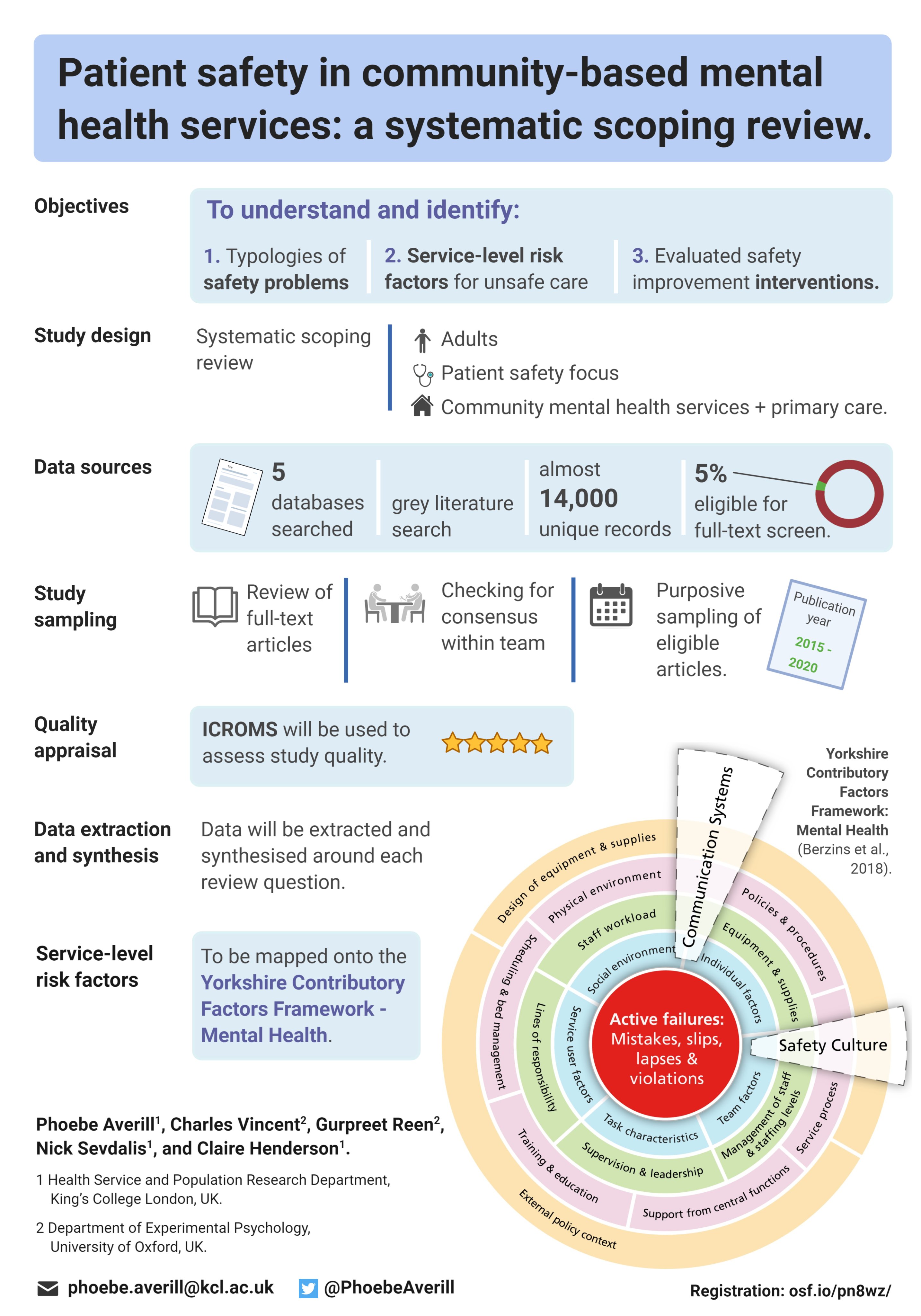
In recent figures, people were using community mental health services rather than inpatient services. So it’s really important that safety is kind of better understood in the community context, so that strategies can be developed to make the services safer. And that’s what she is trying to get started with this research research. Pheobe is currently trying to speak to family members and carers of adults who are using community based mental health services, to find out a bit about what they think about what safe and unsafe care means in this context, because it’s not really well understood. This is due to the types of safety issues that the carer is worried about in relation to the person that they support.
The way the study works involves speaking to her in a either a one to one interview or group discussion with other carers if there was interest from several people in taking part. And there aren’t really any right or wrong answers. It’s really just about hearing carer’s point of view. Carers have so much knowledge about the person that they support and their experiences of care. And it’s just really important that their views are incorporated into any efforts to, to make services safer.
- Questions from carer members.
One question was focused on the issues of patient’s age. The carer felt that a 75 year old patient does not have the same issues you’d have with a 25 year old and they were curious to know, what Pheobe would be doing for older adults when it comes to community work? Especially for the carer because there’s a lot of issues with older carries with physical issues. How will the research be monitoring those patients or those carers?
Pheobe responded that unfortunately for this study, we’re only looking at sort of general adult services. So we’re Other than older adult services, like you mentioned, it’s not because it’s any less important. It’s just that at the moment, there’s the most kind of research knowledge in adult in adult safety. so future studies would be needed to look at older adults, because there’s like you mentioned, there’s lots of really important safety problems there.
- Statement from myself
After some debate I mentioned that one thing in regards to research is that whatever is found out could lead to recommendations, usually, most research initiatives tend to recommend some findings that will have this influence services. A lot of people feel research is done for either funding on does not solve service issues, but I pointed out researchers are not in charge of mental health services.
- Polly Pascoe – Lewisham CCG Presents
Polly spoke about her work within Lewisham Borough Council and southeast London CCG. Her role is it was called integrated Commissioner for mental health pathways. In essence, one of her key roles is getting us to use future systems across mental health care, while it’s occurring across healthcare in general, her focus is on mental health especially within Lewisham. This is kind of where we’re hoping to head moving forwards. The previous system, that being health and social care worked separately regarding statutory and voluntary. Such as Provider sectors were working separately and sometimes even competitively where age groups were handled separately, and such services provided different levels of focus and funding. Conditions were often handled separately, and there was a strong focus on outputs as in numbers, rather than changes necessarily. So there used to be a strong focus on reaching particular targets, on how many people were seen and how many people were funded by CCG.
Now Lewisham CCG have made some definite headway in Lewisham to becoming much more integrated in the way we do things. Of course it’s a journey. So we’re certainly not there yet. Still, Polly was sure a lot of people will have experienced a number of different frustrations around how the system’s working. She feels we are becoming a more integrated health and social care system. Where we are working much more closely with our sector providers. It’s not just the big players e.g. (SL&M), Lewisham CCG is also connecting into our community organizations and age groups do remain relatively distinct. Often the way we do things will mirror that which isn’t always appropriate until the impacts of concurrent issues are understood. So we do have a clearer idea of how different conditions work with each other, but they are still seen often as separate conditions.
At Lewisham CCG they are certainly moving towards a focus on improving outcomes, but they do still have quite a heavy target focus. Those targets are becoming more appropriate as Lewisham CCG move forward. What they are heading towards is a future system where health and social care workers one, and Lewisham CCG are focused on the individual rather than on our kind of organizational boundaries, let’s say, Lewisham CCG want to move between statutory and voluntary services. So between the NHS Trust’s and then any services working in community to be visible, Lewisham CCG don’t necessarily want people to feel they’re being handed off to different places all the time. And they want people to have their personalised journey where movements between that journey feels very seamless. They also want to move to an all age approach where the CCG see the individual as experiencing certain things throughout their lifetime.
So this is also moving beyond comorbidity, not just recognizing people’s potential health issues, but understanding wellness, and looking at their life, and how the CCG can ensure that the way of living and that the way people around them, treat them and work with them ensures optimum wellness, rather than just the absence of ill health, which is one of Polly’s key findings on commissioning and delivery. So this is the way that the CCG design and make services happen. Lewisham CCG deliver those services to people where it is outcomes based and focused. So we want to move away from numbers of people, and move towards the difference we make to people. So that’s the kind of very much that future system Lewisham CCG is working towards. Polly admits she has one very small part to play in a really huge system. And, in essence, this is kind of where she sits in and amongst everything else. Her area is primarily adults and older adults. So she continues to do look at these two areas, predominantly for herself and her team.
- Carla Fourie – SL&M director of social care presents
Carla started off talking a bit about herself and when she was appointed in February this 2021, although some people will say that they sure they saw her prior prior to this year and that’s true. She started on secondment with the trust last year literally just a few weeks before the initial lockdown. Eventually the role was made permanent, and she applied for it. She was then formally appointed in a full time role in February this year. Carla looked at putting the slides together and thinking about how she could describe what her role is at the trust, she decided, looking at kind of the role to group it into four key categories. As the most senior social worker in the trust, she works closely with NHS trust board and she works closely with SL&M senior managers, to bring a social work perspective, to the NHS trust. So when we look at our multi professionals within the trust, we’ve got our doctors or nurses and OTS, etc.
In the end Carla’s role is to bring the social worker perspective at a the senior level, she has also the responsibility to work across the trust with the different local authorities, and to ensure that SL&M avoids working in silos, so there is partnership working, and to ensure that the Social Work offer is provided to people with mental health needs, and to help people become in terms of prevention. Her other role is also that trust wide responsibility for safeguarding so the heads of adult and children’s safeguarding reports to her including the areas for domestic violence and abuse, prevention agenda. She also has a trust wide responsibility for the mental health laws that include areas such as mental health capacity, Human Rights Act, etc. In terms of just tying back to the social work, leadership role, apart from working closely with a board, she also has the responsibility to ensure that our social work workforce, social workers that’s directly employed by the trust, are also professionally well supported.
Carla spoke in terms of support to carers and families, where she thought, were important just to highlight again, on a slide where the work at that the trust is doing overall, in terms of manpower strategy, and that’s very much also founded on the triangle of care, where SL&M sees the carer very much as a partner in the care that SL&M provide. There’s a lot of information that SL&M has developed as a trust and under the leadership of Gabriel Richards, who leads strategically on the carer’s agenda. SL&M has got a carer’s charter that is highlighted. SL&M also provides information in their families and carers Handbook, and also information leaflets, posters shown in the blog regarding carers rights under the care rights, writing, carers assessment. SL&M also has information about confidentiality and sharing of information.
SL&M also provide information to nearest relative where we have useful nearest relative leaflets as well on what is provided to carers. One of SL&Ms duties is to try To ensure that ‘cared for’s relatives are informed and consulted with, particularly when there was a Mental Health Act assessment under Section two of the mental health act. The approved mental health professional has a duty to inform the nearest relative under Section three, where the relative has the power to object to someone being detained to a loved one being detained under the Mental Health Act. The nearest relative can also ask for an IMHA, which is an independent mental health advocate to see the patient and the nearest relative can request a mental health assessment, which she thinks sometimes nearest relatives not everyone is aware of that in certain circumstances where it’s been really difficult or challenging to access for whatever reason. So whilst the local authority is to consider the assessment under the Mental Health Act, or the rights and powers of a nearest relative. The nearest relative can write to the associate hospital managers to request for discharge. Sometimes that’s out here too, but in circumstances where they’re responsible clinician disagrees from a clinical point of view, they can roll that request up to the hospital managers who will review that decision as well.
An nearest relative can also appeal to mental health health tribunal, and they’ll set up some circumstances where nearest relative feel that they are not able to take on this role, because it does have a lot of power and responsibility with it. And sometimes some families feel that if someone that’s been identified as a narrows relative that may impact on relationships with their loved one.
This concludes our Lewisham MH carers update for July 2021






