Welcome to the July edition of the Lewisham Mental Health carers forum. This is one of the carer forums I run in order to help families and carers understand, engage and query mental health services. This can help services become more carer aware and aides in a working relationship with carer’s.
Welcome to the July edition of the Lewisham Mental Health carers forum. This is one of the carer forums I run in order to help families and carers understand, engage and query mental health services. This can help services become more carer aware and aides in a working relationship with carer’s.
For the Lewisham MH carers forum we were joined by regular carer members, plus Damian Larkin a nurse working on clinical systems. The forum was also joined by Karen Machin a carer peer network campaigner and researcher, plus the communications rep from mental health organisation SANE, Public Health in Lewisham, Maudsley’s complaints department manager Edith Adijobi.
Also in attendance was Beth Brown who is SLaM’s Patient Experience and Quality Manager. We were also joined mental health lead of the Lewishmam & Greenwich hospital trust and lastly the involvement lead for Lewisham & Croydon from maudsley NHS trust.
The Lewisham carers forum runs every last Tuesday of the month and is usually run from Carers Lewisham, but due to the covid-19 outbreak the forum has been running online.
Public Health Lewisham research
First to speak and update carers in Lewisham was Lisa Fannon from Public health in Lewisham. Lisa gave us a brief update on the work that she talked about at another forum I run. Lewisham council is undertaking in a research partnership with Birmingham City Council where they are going to look into health inequalities faced by black, African and Caribbean communities within the borough. Public health Lewisham are part of this process and will be looking at the evidence which have been some of the key issues affecting the community.
Their intention is that they will provide some solution focused approaches which will enable us to tackle such health inequality issues wherever possible. Lisa also wanted to let us know that they are this week opening applications to people within the community to support an advisory board. Lisa mentioned it’s a unique volunteering opportunity to be part of a groundbreaking piece of research that will inform the work that Public health are doing within the local community.
Carer Peer Support
Next to present was on carer peer support networks. Karen who is a peer network speaker spoke about her personal experience of being a carer. She also spoke about the challenges she found on the mental health system and felt being able to sort of stand back and reflect on things.
She did value the networks that she had made when experiencing mental health systems be it locally, regionally and nationally, she had some networks where she could share them with people and hear about what other people have been up to. Karen found those networks really helpful.

The last 10 years or so, her interest has been around recovery and peer support in a way of focusing on healing and discovery. She mentioned that she doesn’t really like the word ‘recovery’ when compared to carers. Even though it is a word that everybody uses, but she is still interested in recovery because it’s always about the people that we support.
She felt that the focus on recovery is always about the person who’s using mental health services. It’s not necessarily about carers. So she did a write up some years ago about it, but she still think it’s a topic that signals whenever there’s recovery then it might not be for carers and everything could be patient focused.
Karen wants carers to query things by asking about the nature of carer support. Questions like ‘What is it?’ What does that look like for carers? And how do we get current skills involved in that? Her main interest is around peer support, and that’s about people supporting each other.

She feels that even with all these new initiatives around peer support, that carers sometimes still get ignored. Around 20 years ago, we were asking for what would now be called a carer peer support worker. Unfortunately she does not see many carer support workers, although there’s lots of initiatives and resources and money going into developing peer support workers which are roles within mental health trusts and voluntary sector organisations.
This is not the same issue around carers. She always wanted to hear from somebody who’d been in a similar position when she was caring, who could kind of use their own lived experience to the listen and support carers. Perhaps somebody who was actually paid in such a role and also was valued and supported themselves.
It’s not just about peer support, it isn’t just about volunteers. It’s also about the resources going into paid roles. We in a situation today that we are trying to avoid the new pandemic. She feels that it has created a really abrupt change. It’s been a very serious and traumatic time for many of us carers. That means everybody even those not accessing mental health services. For the whole population it has been very difficult time. The pandemic certainly has highlighted places where there’s been poor services or poor access to services. Karen felt some criticism at the NHS, but she is usually very supportive of it, which has really highlighted some of the challenges in service provision within mental health.

Karen also wondered about bereavement services and support for carers among such services. She felt that people have looked for access and support, but Karen mentioned that people have also had to look to communities for support.
She does not think they’ve looked particularly to the NHS and because it has been so overwhelmed with other issues. So people have had to look for that mutual aid into communities.
She included in her talk the use of remote access on how communities now can be national and international, and that is certainly a community that she wants to be involved with. She recently managed to speak to participants from around the world and heard from a lot of peer support groups where they’ve been questioned whether people can join them. There have been lots of people from the States and from Australia so networks and communities are getting bigger because of the opportunities of remote and virtual platforms coming from avoiding COVID-19.
Embed from Getty Images
Karen stated to the carers forum that perhaps maybe this is an opportunity to do things differently. She knows that commissioners and providers are all asking us those questions of how we’re going to provide things going forward. When she talked to them she keep repeating herself and saying we have to listen to people with lived experience and their carers. Karen felt that’s something that’s been high on the agenda for the last 10 to 20 years anyway and felt providers and commissioners know that they have to listen to communities, they know there’s a gap between what they commission and what people experience.
Lastly Karen spoke about how our communities can help us to get heard and questioned how do we build those communities? She felt it needs to go beyond local. She mentioned that those at the forum are in a great position in London because we have got opportunities that go beyond just our own Mental Health NHS trust into other mental health trusts. We have a chance to hear about how others are providing services and the different teams that are available.
She does wonder how we can expand this nationally because there aren’t any national networks of carers in the UK. She would like to hope in the future a way to develop national carer peer networks and once COVID-19 is over, then we can start to develop those networks ourselves.
Questions from the carer members
The carer members from the forum were inspired to ask questions to Karen. One member asked what was she doing for older carers in the role she is in at the moment, especially with ethnic minority cares? The forum member wanted to know who at the moment could explain the situation of suffering in silence because of stigma?
Karen mentioned that she has not got the expertise around older carers in her local area, But she has heard of lots of other organizations, not here, but around the country, where carers and communities are coming together to provide that support themselves. She understands about those worries about what happens if a loved one goes into a care home? And what’s that going to mean for us? And so people, it’s about, it’s what she has been hearing, it’s about communities doing that work. And that really worries her in many ways, partly because the sustainability of that, how do those local just groups of neighbors basically, and how do they sustain that effort? And how do we scale that up? How do you make sure that that continues?
Another question raised was from a carer who had read in The Guardian newspaper that Boris Johnson is considering amalgamating social care into the NHS. She felt in principle, I think it’s a good idea. But what what concerns her is that does that mean that’s another group getting that is going to push mental health out of the way? Because Health services has made mental health services a Cinderella service and now social care will make it even more irrelevant.
Karen responded that we got to keep an eye on such things and she felt it’s through networks and making sure that we’re all connected within that we can keep an eye on. Karen did agree with the carer and felt perhaps the change could potentially be fine. It could have potential. Still she thinks many will be worried about that gap between health care and social care.
SANE new campaign and project
Next we heard from Emma who is the media and communications officer at the mental health charities SANE. They are a national mental health charity. Emma felt it was a real privilege to hear from carers and to learn from us as well. She thanked us for having her in this space.

Emma introduced herself as the media and communications officer for SANE and they are working on some exciting projects although she could not go into detail at this moment in time because it’s still in the planning stage. The campaign will be launched around autumn time and they are looking to collaborate and work with caregivers, mental health caregivers who care for someone with serious depression.
Emma continued that supporting mental health care givers is also a core campaigning area for the charity and she knows it’s something which SANE’s CEO Margie Wallace is really passionate about. So if there’s anything that SANE can do to support us or if we know if anyone’s interested in reaching out and working with SANE then please do get in contact.
Patient Experience and Quality Manager presentation
Next to speak at the forum was Beth Brown who is SLaM’s Patient Experience and Quality Manager thanked me for inviting her. She was here to talk a little bit about what she does as patient experience and Quality Manager. She then talked a little bit about one of her work streams, which is the patient and carer feedback surveys. She mentioned her role has kind of two main aspects to it. The first one is around patient experience, so she manages the trust wide patient care experience survey program, which some of the group might have heard of which is called PEDIC. Beth also look after the Trust’s participation in any national surveys which are run by the Care Quality Commission. So that’s the means that they participate regularly each year is the National Community Mental Health Survey.
It is her role to look at the themes that come out from all of these places and, and try and kind of track trust wide themes. And that can help inform our services, and to kind of look at their local improvement because the whole point of it is that we can improve services.
Beth moved on to talk about how she manages clinical audits and the effectiveness team. They look after a program called perfect Ward, which is a way of tracking clinical audits throughout the trust, which includes things around clinical safety, medicines, infection prevention control. They also have an audit around patient experience and staff experience. Plus they also have someone in the team look after NICE guidelines, so you can have best practice for trusts and national clinical audits which are run by the Royal College of psychiatrists.
At this moment Beth’s team are just preparing for a upcoming National Audit on early intervention in psychosis. Beth started showing the forum presentations from her slides. Where she showed how centrally important that audit team works with the patient and public involvement leads and on complaints.
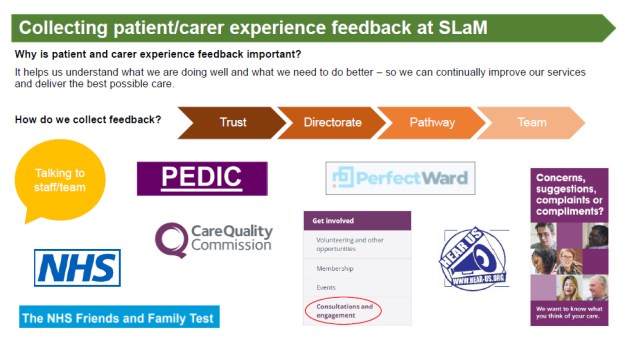
Beth tends to have a large spread of different people to work with, she went on to why a patient care experience feedback is important, because so they can see what we’re doing well and what we need to do better so that we can improve the services and deliver the as possible care. Plus they need to collect feedback in a lot of ways.
They have kind of lots of more systematic and structured ways of collecting feedback, where Beth showed the data the team collect it from a trust wide level right down to individual team level. From on the Ward and the NHS friends and family tests, through to kind of trust, consultations and engagement. The team also work through complaints, PALs, service formal and informal effective compliments, a kind of like individual project based feedback.
As Beth showed us her graph and she explained top left graph which is around on the friends and family test score in Lewisham. There was also the national indicator for patient experience. The aim of the graph is what extends as and so what this chart is it tracking the number of positive responses to that to the people that say they’re extremely likely or likely to recommend the service they’ve received.
And there’s tracking over time from April 2017. And you can see from around January 18, to may 2020, if you put a line through it, it’s a very gentle increase in performance. And that reflects trust wide performance. However there has been a significant change, due to this massive dip in June 2020. That is the impact of COVID-19 on our data collection. They had two of our data collection methods suspended due to infection infection control. And now got two out of three open and but we had a massive drop in response rate. So it’s the two that means that the fewer responses you have, the more the data is influenced by extreme responses.
So the forum was shown data for Lewisham over the past year and the members were told that the team had overwhelmingly positive responses, and those numbers of 1169 and 21015, their response rate, so that’s the proportion of positive in comparison. Beth reminded the forum that I was interested in hearing about the FFT school, by ethnicity and by ethnic group. So at the end of our PEDIC surveys, they asked a number of demographic questions and the purpose being that they could see whether any particular groups are reporting different experiences. And that can help inform different work streams.
So for example, there’s just been a piece of work that we found in Lambeth where LGBT patients were reporting poorer experiences. there’s also a trust wide quality reports, which you can get on SLaM site website, which talks about FFT scores.
A piece of work that Beth is doing at the moment, is to allow her to look at positive and negative test results by ethnic group over around 25,000 participants so that they can make more data and say something more about the database quickly to see what it is telling them.
Questions from the carers forum
One carer who is often interested on where mental health services get delivered queried the actual number of people accessing treatment. If it’s a positive outcome, obviously, it’s very good. But that doesn’t necessarily mean that mental health services are delivering good services. The carer felt that SLaM are missing delivering service to the people who struggle to access services via their GP. because sometimes there’s subjectivity as to who goes through and who doesn’t. And as we all know, there’s also financial constraints. And also people who, who don’t feel comfortable with a GPS, therefore can’t get a referral, even with their carer is trying to get their relative to access services.
Another carer agreed and felt it was one of the most stressful things that they found as a carer and that they belonged to several carers groups noticed several people have said this, that it’s it’s especially with children anyway, as well. It’s not so much having the child or the person with the mental illness.
Beth responded on member’s experience of their loved one’s difficulty accessing services and the impact that has been. She continued to mention that they are hearing about that in our patient surveys.
So even the people that are accessing our services are talking about the difficulty that they’ve had to get it and the impact that’s had on them. That is kind of growing in prominence as the you might have seen over the past couple of years. It is an issue and it’s it’s an issue that the trust is aware of, and there are lots of workstreams and programs going on across the trust to tackle access to services, not least Since COVID, so since since before that as well.
BETH application presentation for service user and carer input
Next speaker at the Mental Health carers forum was Damien who spoke about the revamped online patient system called BETH. BETH is an online app and what it does is connect patients or service users peers and staff, they can communicate, they can collaborate. And it’s not an app because it works through a web browser.
Still BETH does it look and behave like an app what’s known as a web app. To access BETH the address is beth.slam.nhs.uk . Since this is a new digital online platform it connects us and it supports the service user’s the treatment that SLaM provide. Damien mentioned that because of COVID-19 that we all have to try just try and communicate in different ways not because it just hasn’t been possible to do what we have done previously, its just BETH really supports this.
BETH takes its name from bethlem and which is the Bethlam hospital that SLaM have in new Beckenham and also the museum of the mind. SLaM’s vision is that BETH will support the care treatment that people receive. Damien then showed the forum some presentation slides of BETH in action. Damien showed the carers how it looks like on a mobile phone. BEETH can be used on a mobile phone, it can use on a tablet and it can used on any kind of device like a laptop, or a desktop.
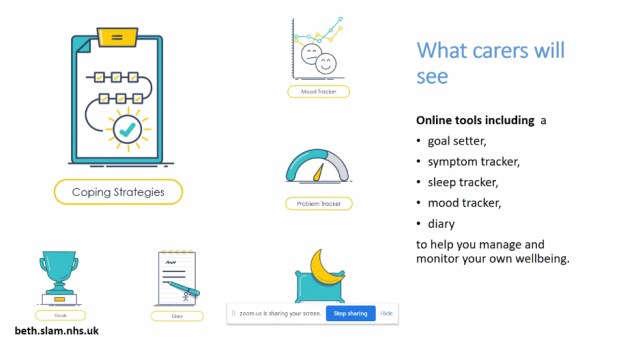
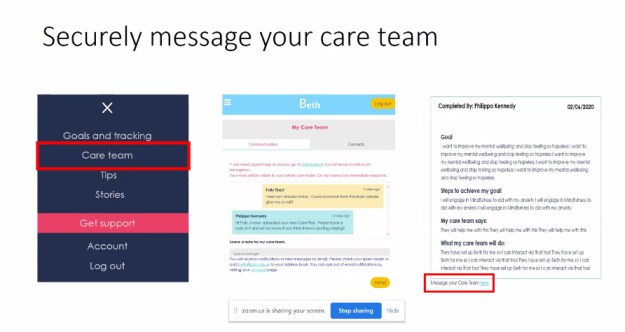
Damien also showed how service users or patients signup to BETH and how they can securely message the care team, they can also get access to their care plan or consider upcoming appointments. Patients can keep track of mood and sleep and they can use the free online resources that SLaM have included in the BETH online system.
Service users can choose to use certain functions and also carers can choose other BETH functions. There’s more in there for patients at the moment although SLaM want to do obviously develop on this. Damien then showed us how to register for the BETH system in instructing on where to sign in if your patient of services by you putting your first and last name as it appears on SLaMs records.
You would then just put in your email address and you create a password and that becomes your login details for everything. But then in the middle you see that red box there’s two tick boxes, one to indicate if you’re patient one to indicate if your carer, family or friend.
if you’re a patient, the two other boxes appear saying asking for date of birth and NHS number and then they accept the terms and conditions all of that and you get access. If you click on the second box there to be a carer or friend. Once you hit on create account, it’ll ask you if you want to connect the care team of the person that you care for. And you just need to put in the person’s name full name as It appears.

Complaints department Presentation
Next we had Edith Adijobi who is SLaM’s complaints manager to engage with carer members at the forum. When you think of complaint’s carers tend to grit their teeth, but I noticed the members were happy to get engagement from complaints because people feel complaints tend to hide away and defend services. Edith opened up her talk by stating that she genuinely love complaints. I noticed one or two carer’s laugh about this, but then they warmed to Edith.
Edith mentioned that she has been working in the field of complaints, panels, patient experience and bereavement services in the NHS for about 21 years. She is very passionate about complaints. So in the trust people sort of have to stop her talking. Edith mentioned that she is also known in the trust for a lot of pushback, because one of the things that frustrates her deeply is if she ever hears somebody say there’s nothing they can do, then Edith feels that carers have to complain.
Edith feels that people shouldn’t ever have to complain to feel heard, she feels people shouldn’t ever have to complain to feel that services are going to do something about something they flag to SLaM. That doesn’t mean services stop people complaining. But if we’re telling people that the only way we’ll hear their voice is if they complain then something’s gone very wrong, and that really frustrates Edith.
Edith does staff training on complaints, So one of the things when she does on training their staff is she is officially their worst nightmare at times. She mentions that officially she acts as a worst nightmare as a patient. Edith then took us through some brief data. She talked a little bit about why we take complaints as a trust and the approach that she finds
She feels it’s about really encouraging and supporting ourselves to think about doing the right thing at the right time, really reflecting on on the information we get. And how do we learn from mistakes, because she thinks the moment you say the C word, as she says complaints, people get their backs up, people get quite anxious. How about we split it into a concern and a complaint? what is actually happening there? What are people trying to tell us? And these are some of the ways in which we get information.
Edith talked to carers about the different organisations that are interested in the types of complaints the NHS Trust gets. So they get reports from the Care Quality Commission, quite a lot of our patients will go direct to the CQC and to then pass them to us. We also get views from Health watches, SLaM’s CCG commissioners, we even get people tell us first What do we do and how do we did Last year.

Edith spoke more about the charts on the presentation and showed how these are the complaints they got as a trust. Although in one month the figure obviously dropped really sharply because of COVID. Edith showed us a closer look at Lewisham complaint figures and noted if we could see my mouse just scrolling under the Lewisham accounted for 88 out of 558 complaints pulled up through the Directorate.
She then looked at complaint, which was commissioned by Lewisham. So that will go across SLaM’s oldest adults and their CAMHs service, but this was just to give us a trust wide look. Looking across the trust, if you have a look at the Reds or the complaints and the blues are compliments.
Edith moved on to mention that they have tried a new system since last October. They are encouraging people to record directly so that we can actually capture information. So just that was an April to make a March this year. This is this quarter, and you’ll see that a bit had a real impact on just SLaM’s organizational numbers they receive.
Edith mentioned that sometimes it’s just somebody picking up the phone and not being able to get hold of a doctor, not being able to get hold of a nurse, or, in some cases, people wanting access to a service. But the commissioners haven’t actually commissioned us to provide that service. So how do we as an organization feedback to the CCGs or how do we actually tell somebody that what they want is what we Provide that’s not being provided by a third sector partner, or the CCG has different arrangements.
Edith concluded that sometimes we’ve got those type of issues going on and sometimes someone is to blame. Sometimes when something is wrong, it is because of there is a reason. So one of the things maybe we want to look into is culture of the trust. Is it that we’re blaming that member of staff, and that member staff is the one who’s accountable because an appointment failed to be booked? Is that staff member under too much pressure or not supported? What is the cause?

Carers from the forum were surprised, but happy to have a presentation from the complaints manager since the forum has existed for many years and the subject of complaints is often raised.
 Welcome to another blog post by Matthew Mckenzie, a former carer and carer activist from South London. I usually focus on carers who care for someone with a mental illness, but at times I delve into health and mental health.
Welcome to another blog post by Matthew Mckenzie, a former carer and carer activist from South London. I usually focus on carers who care for someone with a mental illness, but at times I delve into health and mental health.



 Hello, everyone, welcome back to another carer blog from former mental health care Matthew Mckenzie.
Hello, everyone, welcome back to another carer blog from former mental health care Matthew Mckenzie.
 Welcome to the July update of the Lewisham BAME mental health carer forum. I’ve been doing this forum for many years now. As a reminder I run carer forums aimed at carers who are looking after those with mental health needs challenges or mental illness.
Welcome to the July update of the Lewisham BAME mental health carer forum. I’ve been doing this forum for many years now. As a reminder I run carer forums aimed at carers who are looking after those with mental health needs challenges or mental illness.

 Welcome to the July update of the MH carers forum.
Welcome to the July update of the MH carers forum.