If you have been a regular to visiting my blogsite then I am sure you have seen a few blog posts about the fantastic mental health forum over in West London. Taken from their website “We Coproduce CIC is an award winning social consultancy, owned and run by local people for people who care about the future of health care in the UK. They are commissioned to work with local communities to coproduce better and braver solutions to health and social care challenges.”
We Coproduce do a lot more than run their forums over in Hammersmith & Fulham, Hounslow and Ealing. Over many years they have worked closely with the mental health trust West London NHS trust on improving mental health for the community. For the October forum facilitated by both Jane McGrath and Natalie Louise there were many exciting speakers.
One of the speakers was myself where I talked about my new book “A Caring Mind”. You can see the talk I gave from the video below.
Matthew Mckenzie speaks about his new book – A Caring Mind
The book “A Caring Mind” shines the spotlight on the carer’s experience when caring for someone with a mental illness. Often carers stand in the background and carry on supporting their loved ones because of duty, love and just being there.
I felt it is about time I put my thoughts down in a book and We-Coproduce along with West London NHS Trust supported the work I was doing.
You can get hold of my book on Amazon either in Paperback or Ebook.
Welcome to September’s 2020 update of the Lewisham Mental Health carer forum. The forum is run via Zoom to protect attendees from the risk of Corona Virus. The forum usually runs from Carers Lewisham centre, but is now online. The carer forum gives carers in the borough a chance to engage with Mental Health and Local authority services. It is a form of empowerment for carers and a way to gain insight and knowledge.
The forum also gives carers a chance to work together with health providers as co-production often gets raised. For the month of September we had a special “Carer Peer support” event, where many other carers were invited from my other carer groups, especially some from Greenwich who were wondering what does it mean when a mental health trusts champions peer support. Carer peer support has a different focus though, as it is aimed at families and carers. It also must be mentioned that peer support does not have to be a service that comes from the mental health trust, but carers themselves can also practice it.
We were joined by Peer speciallist and carer Donald robertson from sussex NHS partnership over in Brighton, we were also joined by Shelagh Musgrave from Birmingham and Soulihil NHS trust. Both were at the forum to educate and explain the importance of carer peer support at NHS trusts and services. We were also joined by Rachel Ellis who is South London & Maudsley NHS deputy head of inclusion and lead for peer work.
As usual the forum was supported by SLaM Jane Lyons who is the Croydon & Lewisham Involvement lead, however our CQC member could not make the forum today and has requested an update. Some of the things mentioned by the other NHS trusts peer leads should be of an interest to NHS England as there were views regarding peer support pilots across 3 NHS sites.
Sussex Partnership NHS Foundation Trust Carer peer support
Donald Robertson spoke at length of his role over at Sussex MH NHS Trust. He started off as a carer who cared for his wife for many years before slowly becoming more involved as peer specialist at his mental health trust. He now works within the NHS. So he feels like he can inhabit all three corners of the triangle of care in different ways. Due to being a carer, going through difficult times and being a health professional. Donald was trained as a social worker based on his own lived experience.
Donald mentioned peer support is about using his lived experience as a resource. It’s about changing things and how he wouldn’t go back to some of the times his been through, he wouldn’t even give his worst enemy back to some of those times he had, but his glad it that happened, because it made him a stronger person for today. Don pointed out peer working is a bit special. and it’s not just about having the the lived experience, it’s about how you use it. Peer support is how you support somebody with without having to be competing to see who has got the worse symptoms.
HOW PEER SUPPORT WORKS
Donald usually meets or chats to carers reffered to the trusts peer support via video link or phone and asks them “What would be helpful for you” “We can talk regularly as one to one around 15 minutes at a time. He would then confirm that the peer support can be flexible for carers to engage with him or donald could even be in contact with carers by text.
Donald spoke about the carers groups. One of the main groups actually existed before the COVID situation. Don mentioned that he sort od reshaped the carers group and things started settling in their place. The peer group has good numbers where 10 to 16 carers attend. So the peer group is really became very successful. Don asked that people to come to that carers peer group first or to call because he understands that when a carer is struggling? especially if its isolation or if they feel like they are the only one in such situation. Then being in the group where people just get it and understand where you’re coming from almost without having to say anything.
Don was glad to see veteran carers take the lead and set up a workshop to showcase the aim of peer support and the peer support group. There were challenges and struggles as other means to connect were difficult, especially connecting through social media or trying to work out how carers connected through whatsapp, plus NHS England set up something that is aimed to protect people’s anonymity which is very important, but also reduces the chance for carers to connect with each other.
It was also reported that when COVID-19 arrived around spring time, it shook peer support up a bit, because Don was not fully comfortable providing peer support online. This was especially when someone is telling you a difficult and emotional story only for the connection to drop, plus it misses several aspects of peer support including reading body language and giving others the chance to speak. Donald wanted to make the most of his time as being part of the NHS team when it comes to providing carer peer support, he did not want to duplicate what was provided there already and wanted to focus on giving more options for carers.
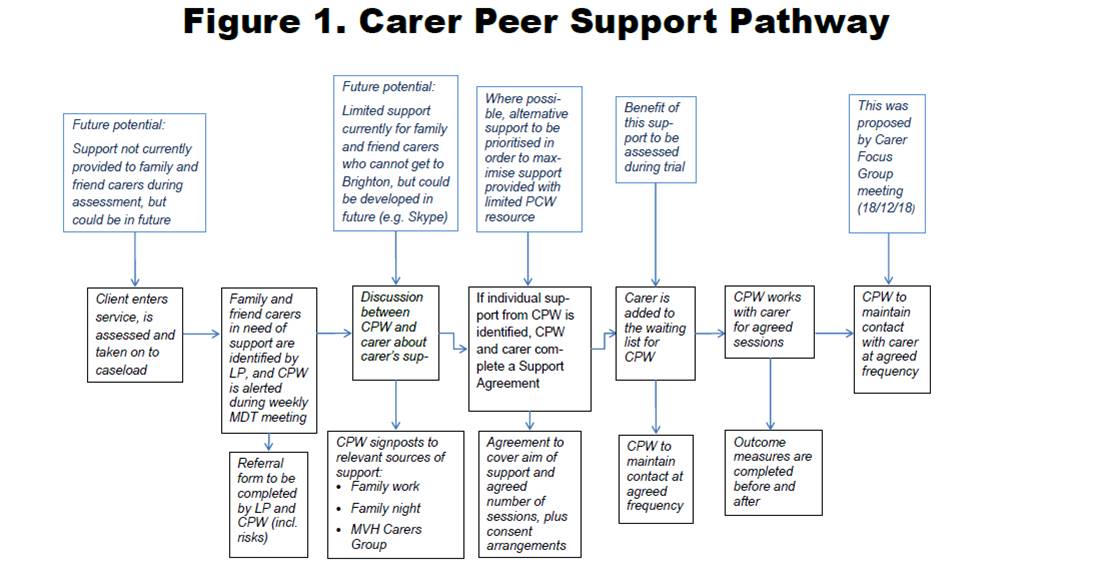
DESCRIPTION OF CARER PEER PATHWAY
I then took the oppertunity to ask Donald Robertson about his NHS Trusts flow chat regarding carer peer support. This was one way carers can examine how a mental health trust can provide support without having to read into any difficult jargon. It also gives an idea that the NHS trust is interested in carers and has a pathway on carers.
Donald told the forum that the chart is focused on carers supporting people having a first episode of psychosis, it’s about the evidence. So if you put some more intensive support in for some carers, that will mean that they will not end up in a long term service user. So the client service user is taken on and our standard assessment period is about six weeks.
There’s a lot of getting to know somebody before it’s completely clear, whether it is psychosis, or if there’s other factors, and Don actually gets involved earlier to help signpost to other services. Still, the lead practitioner identifies the carers and if the carer does not want support so close to the NHS Team then there is always independant carer support at Brighton’s carers hub. The mental health support team will always endeavor to keep the carer involved as much as they can.
You can find out more about Sussex NHS Partnership below.
I then opened up the forum for carer members to ask questions regarding carer peer support at Sussex mental health NHS partnership.
A question on Older adults was of interest to a carer member. He was interested on what information did Donald give out the to older adult carers who are caring for someone with dementia. The carer was wondering if the pathways were more of a one shoe fits all policy. The carer member was also interested in sigma from the BAME community over in Brighton and wondered if Donald had any connection to that group.
Donald responded that it’s important to avoid the one size fits all policy. He engages with carers more as a person centered approach. So Donald is asking what the person in front of me needs. In the Services Donald works in it is all about people who have experience psychosis for the first time, traditionally that’s dominated by people in their late teens or 20s. So there’s a lot of work to be done about helping carers to acknowledge that they are carers. Donald feels his stereotype of a carer is somebody who is helping someone getting dressed, and maybe spoon feeds them, but he himself has never done that. His caring was much more about emotional support. And, rather than kind of fairly practical stuff even though they’re both important, but they are quite different.
I mentioned to the carer that since Sussex NHS partnership was a large trust that maybe Donald was not involved in the dementia service or BAME engagement, but there can always be a forum where we examine how other trusts engage with the BAME community.
Another carer member wanted to make a statement rather than a question, she felt so much resonates with her on what Donald spoke about. She pointed out 3 things, the First point was on how Donald mentioned the typical age group, that someone gets psychosis and some of the other illnesses or some of the other mental health illnesses. Her son fell ill when he was in his late teens. She still is not sure that her son’s illness has been fully identified and what caused it. Her Second statement was how it affected her so much that she couldn’t move on with her life, it was very difficult for her to move on.
Her Third and last statement was on how she was assisting my brother and even though her mother had 10 of us, she ended having to be the one taking on the caring for her brother, while most of the other members of the family want to know what’s going on with him they are not offering to help.
Donald responded and agreed that when one of the carers who was in that situation he remembered them telling him to “help them is help the people around me to not come through me” Donald remembered that he did a work with about four or five different people from that family. He felt it’s quite natural, because people are scared, it’s easier to get it second hand in some ways, because the main carer is that kind of buffer.
Another carer raised the point about my recently released book and if the CCG would take the oppertunity to help promote the book due to my high profile of raising carer awareness. A recent update is SLaM has purchased my book to the library under their carer’s section, although the carer mentioned the book should be standard reading on training staff about carer identity.
Birmingham and Soulihil NHS Trust carer peer support
The forum was given a chance to hear from another mental health trust on carer peer support. We heard from Shelagh Musgrave who is the Family Carer Peer Support Worker on the Women’s Secure Blended Service Team.
She started in her role nine months ago, but she was honest that there are challenges as she felt there are still NHS collegues who do not embrace family/carer involvement in getting peer support. She felt there can be a lack of communication to the carer and it needs to happen more often. This is particularly a problem when confidentiality continues to block carer involvement and then causes families to back out of recieving any other means of support.
She mentioned it can also be quite challenging to encourage colleagues at the NHS to understand that actually families and carers have shared information with them so then it’s no longer confidential. So if they have shared something with us and I tried to speak with colleagues about it, I surely can talk about it to them because it isn’t confidential anymore. Yet, this is not often the case as if something keeps blocking that triangle of care regarding families and carers.
Another issue with confidentiality is Shelagh’s role is actually with a charity rather than embedded with the NHS trust and even then confidentiality can sometimes block her off from getting involved or finding out what is going on. For example because she is peer support worker she might have picked up on a self harm incident and would need to update the family on what could be happening. She felt it’s really hard to get information as a carer and they just have to sit with it. It is like the carer is left wondering what’s happened this time.
The reality is that the carer be informed of these incidents, because it’s relevant to the person that cares for them, but unfortunately the culture of care is that carer may get shut out, which leads to impact or the trauma that might be taking place with the family and carer is left, as it always has been.
Shelagh mentioned that the NHS Trust actually have a family/carer pathway modeled within the trust, although it’s in the very early days. Still there is a problem as there is a seperate service user pathway and that process has created challenges as well, because it has led to some of her works going on hold.
Still there has been good engagement where it has made a great difference for families. Shelagh mentions she goes on to contact carers and get feedback from them, which is incredibly positive. Shelagh stats that she has a very proactive approach to being in touch with families and carers and she essentially makes my initial contact with them introduce herself explaining what her role is.
Shelagh does ask carers, what would be helpful for them. But she also makes them aware that she will be touching base with them regularly. So her approach tends to be, and she will call and if you don’t want to speak to me, that’s absolutely fine. I will check in on a monthly basis and I wouldn’t take offense, if you tell me you don’t want to hear back from me going forwards. Oddly enough no carer has actually told her that they do not want to hear from her.
Still Shelagh does not speak to every carer that’s on the books and she does make contact with as many of them as she can, but is not permitted to contact some because there are some for clinical reasons that I’ve been asked not to be in touch with, which she felt was a shame, but she can’t argue with that because she does agree with that everybody should be entitled to access peer support, if they wish and she do think it should be your decision, I do think it should be a clinical decision.
So she has ongoing contact, which ranges from anything from every fortnight to every two months. What she also do is feed concerns that the family have back into the a clinician. So for example, we had a young woman who was being discharged. Her family had attended the discharge CTA section 117 meeting, but actually hadn’t been given any contact details for the community care coordinator or the accommodation manager. So I was able to feed that information in the team to get contact details from the team and was able to get information to that family.
As far as the NHS knows they were aware that she has ongoing contact with families, but what she finds really interesting is a professional at the NHS states to her that our contract has to be meaningful. What does this mean?
Well meaningful to who and when you drill down, meaningful contact seems to be viewed as contact that is going to provide information that’s relevant to the service user. So if Shelagh’s contact with the family is not going to provide the clinician with information that is useful and valuable to the service users care then there is little point in meeting the family, but Shelegh is against this culture, because in her role she is there to support the families and carers and I, if they happen to share something about services or have a team.
Shelagh does tell NHS professionals she works with right in the beginning, that she works for a charity in partnership with the NHS and has an honorary contract with the NHS. However she is not sure if it’s because she works in the charity or because the NHS hears the word peer that NHS professionals might stand back.
Shelegh feels the feedback she gets is the value of talking with somebody who has lived experience is “that you just get it” and the carer does not have to explain what things are like to me. Shelagh has lived through it. She feels because carers might be limited in communication if they are talking to an NHS professional, nurse or psychiatrist. There’s often a sense of well, what do you know? What do you know, you haven’t experienced it from my carer’s side? So how can you stand there and say this to me. Whereas carers sense if she says something to do them or listening to them, and they will often say to her but you do understand this, don’t you?
It’s like a shortcut has created in connecting with carers and families where you don’t have to explain to people, what it’s like to deal with your child who self harms and you don’t have to hide from people, or you don’t have to explain to people how heart wrenching it is to hear when your child says to you ” I don’t want to live anymore why dont you just let you die?”
You can find out more about Birmingham & Soulihil NHS Trust below.
Family Carer Peer Support Worker view on the future of carer peer support
Shelagh felt that there is a massive need for carer peer support workers. She is aware that carer peer support research is very limited. However, she thinks we have to look at is that the research into peer support itself shows its value. So why do we have to differentiate whether or not peer support is carer or service user we’re looking at here towards the value is of lived experience. Doesn’t matter what your lived experiences?
Personally, she don’t believe it does. And But clearly, there are people who work by the research. That being NICE (National Institute in Care & Excellence) works by the research, Shelagh mentioned that she is very upset wit NICE because of this and she think that’s really sad peer research is not extending to families and carers.
Shelegh feels when carer peer support is established and its on the ground then we can see the difference that it makes, she feels that does not matter, what the background of the lived experiences is and wonders is she the only person in the NHS trust, which has 4 and half thousand staff?
There is a definite barrier of some sort, by changing the way families and carers engaged. Shelagh thinks we need to be doing it. She thinks we need a top down and bottom up approach, which has to come together. Because if you don’t have the support from the senior management’s, you’re not going to have this sense of drive.
Shelagh hopes that over time, she hopes that more and more people will change and understand that families and carers are not just there to provide background information on the service user. Carers are the equal partners in the NHS and NHS professionals also have a responsibility to families and carers. Because if they don’t support the families and carers with somebody is in the inpatient setting and they just discharge them into their community that hasn’t been upskilled or that hasn’t been supported, then it’s good to keep that revolving door going on for decades.
South London & Maudsley Peer worker presents
Rachel who is SLaM’s lead for peer working thanked Don and Shelia for their experience and is eager to see what results in regards to NHS England’s pilot peer project. Rachel is interested in what worked and what didn’t work. She was also thinking very much about what was the feeling or thinking about peer support is it needs to be co produced. Rachel felt that we can’t just take the model from Birmingham or NHS England and then drop it down in South London and hope that it works.
What SLaM needs to look at is that we need to learn from what the carers want to help them relate and be involved and also engaging with the BAME community. We also want to make sure that we have something that we know works from the outset and avoid that one size fits policy, we need to be creative, and we hope to be working alongside our carers to make sure that we get it right.
Rachel feels the big questions and the elephant in the room is about money/resources and how state to the CCG or other people to make sure that kind of professionalized peer support is seen as important and something that they’re willing to fund that and I feel that’s where the carers forums like this really come into its own and making a guideline proposal around what you’d want from care with peer support.
Rachel mentioned it would be really useful for members to write something formal to the Commissioners about your needs and what you think professionalised peer support would look like. Rachel added what carers would think the benefits are to the CCG especially relating to the triangle of care.
So it’s not just around providing peer support and support for carers, but also making sure that that’s all linked in so we get a really good support for when someone’s discharged or someone’s community services. Its not only important support for carers, but it’s also seen as linking up care for the people who use SLaM’s services.
This concludes the September update for the Lewisham Mental Health carer forum.
Welcome to another Blog post from Author of A Caring Mind, carer activist and former carer Matthew Mckenzie. As of today being the 10 of October 2020. It is World Mental Health day and The theme set by the World Federation for Mental Health is ‘mental health for all’.
There are many organisations and charities promoting world mental health day. If you want to see the video of this blog, then see below
World Mental Health day is about continuing to raise that much needed awareness of mental health each year. This year’s theme set by the World Federation for Mental Health is ‘mental health for all’. When we talk about Mental Health, people tend to feel mental illness is about Mental health problems and how it affects around one in four people in any given year. Those illnesses such as depression and anxiety, to rarer conditions such as schizophrenia and bipolar disorder.
Mental health problems affect around one in four people in each year and since this has been a tough year due to lockdowns and loss that have had a huge impact on our mental health.
However we can all feel depressed, angry, stressed or frightened. This is why Mental health is everyone’s business. We cannot continue to state severe mental illness is someone elses problem to fix. Taken to the extreme, even anger can become a mental health challenge if it gets out of control.
It does not help that around 450 million people live with mental disorders that are among the leading causes of ill-health and disability worldwide (WHO’s World Health Report, 2001). The World Economic Forum (2018) noted that mental health disorders are on the rise in every country in the world and could cost the global economy up to $16 trillion between 2010 and 2030.
From job losses and uncertainty. We’ve all found ourselves under pressure and carers are not exempt from such pressures due to having to care and support someone suffering mental illness due to extra strain. It is important carers get a chance to support their own mental health and wellbeing, please its so important carers take a break and take time out even if only for a little while.
There still is mental health stigma leaves people feeling isolated and ashamed and not being able to access support, so this is one of the reasons for campaigning on World Mental Health day.
The good news is that you can do something for World Mental Health day and raise awareness, be it by talking about it, campaigning even if using social media or attending online events, it does not hurt to raise that awareness.
This is my first blog post of many about my new book “A caring mind”. If you have visited this site in the past, then you are probably fully aware that I promote the experience of caring for someone with a mental illness. This book of course is no different and promotes my cause even further.
There are several differences between this site and my book and that is I cover my carers journey when caring for my mother and supporting my brothers. I also cover more in depth the importance of carers getting involved and also networking with each other.
Some information has been taken from my website and added to the book, but I have also included new topics that can only be read from my new book “A caring Mind”.
For anyone caring for someone with mental illness this book can give many things including identifying with other carers, giving hope for the future, examining current carer themes, empowerment for mental health carers and plenty more
Here are the chapters of the book, but if you wish you can buy my book from Amazon
Welcome to the brief update of my Lewisham BAME Mental Health carer forum which is aimed at minorities caring for someone with a mental illness in the borough of Lewisham. The September forum looked at engagement from South London & Maudsley’s IAPT service (Ellen Heralall) and also engagement from the SLaM QI Peer Project Worker (Richard Mortan).
We were joined by the regular carer members and also newer members including some from my other carer group in Greenwich. There were also some members from community groups including African Advocacy Foundation, Bromley, Greenwich & Lewisham Mind’s community wellbeing group and others.
We were also joined by the comms rep from Birmingham Community Healthcare NHS Trust who was interested on BAME developments in the area. We were also joined by Leonie Down from SLaM who is developing partnerships across Lewisham as part of the transformation of mental health services. Part of her role is to bring together a community strategy for service users, staff and carers within slam.
Ellen explained more about the IAPTs service which means Increasing Access to Psychological Therapy. The IAPTs service has just been running over a decade. They are based in primary care. So they operate very closely with the GPs and operations within GP surgeries. The IAPTs is also now part of the national framework, which is provided by NICE (National Institute of Care and Excellence) which recommend treatments. The aim is to provide easy access for the community to receive psychological therapies for depression and anxiety primarily, but not complex mental health conditions.
The referrals would come up from the GP and people can refer online to go through the triage process. Then they’re offered either step two treatment, which is a Guided Self Help well-being option via online CBT and psycho-education.
Ellen explained that the therapy will usually last generally from six to eight weeks. She mentioned that as with a lot of NHS services, they are fully aware of the discrepancy in the quality of services for the BAME community, accessing IAPT services. Plus when they do access our services, we are also aware of the inequality of their experience and their outcome in poor experiences.
So SLaM have been working on their objectives, but they are resourcing and working hard to look at improving the access of IAPTs to the BAME community,
SLaM are working with our community partners. Which is the big drive for SLaM at the moment to work with community groups, especially with ones attending such forums e.g. community groups, wellbeing groups and fitness garden projects that already exist in the borough. SLaM are partnering up with such groups and seeing how they can work together to bring psychological therapy and mental health awareness treatment to the community in a way that is relevant for them.
Ellen reported that SLaM are also reaching out to step outside of the box and make themselves more accessible to provide such psychological treatments, but also to build more relevant services where to a greater racial understanding of how racism, and discrimination and inequality affects mental health. This helps in raising the awareness of triggers in such experiences. Racism is a trigger and discrimination can also be a trigger to mental health. It is important such forums like the BAME carer forum exist so these things can be talked about in safe spaces.
Ellen mentioned that it’s good to be at the carers forum to talk and network about how how we can continue to become a more accessible and more relevant service.
IAPTs will work with those from culturally sensitive support groups. So there’s lots of different projects IAPTs is involved in. They have become a sort of a broader service that is probably in excess of 100 staff on IAPTs alone.
Ellen felt it was time to open up to questions from the members and attendees from the Lewisham BAME carers forum.
Question and answer session at the forum
The first question was on working with grassroots practictioners on issues with racism, discrimination and some data triggers that effect on mental health.
They wondered how IAPTs is mainly dealing with practitioners and the community within that kind of setting and how does it actually work? Especially with the aim to raise awareness and to deal with the issues of the experience of racism in the community.
Ellen mentioned that there was someone who had been running these groups already. She runs the groups in culturally sensitive emotional support groups aimed at the black and African African Caribbean community, which were 12 weeks. Ellen quoted that the groups were safe spaces to talk about mental health and a convient way to develop emotional wellbeing.
Other questions were on staff and how many were from the BAME community. Ellen did not have the figures to hand, but is bound to bring them at a later date, although she did mentioned about 50% to be vague. Ellen actually leads on the counseling team and because they come through a different sort of training and different routes they tend to get a very diverse range of counselors.
The psychological well being of practitioner to practitioners are now become more increasingly diversity, Ellen might have to get back to exactly the figures, but SLaM are certainly visibly increasing numbers of young BAME psychologists coming into that work stream, where the mental health service have the biggest problem is in in high intensity CBT.
Although BAME therapists certainly are increasing, Ellen felt we’re not there yet. The service is still actively recruiting BAME therapists.
The impact of COVID and technology
Another question arised regarding COVID-19. The carer member queried about lockdowns going on for another six months, he felt carers will come to the organization in six months time, with the community suffering with depression, anxiety and stress. The carer was wondering how they’re going to cope with the extra load BAME carers who have suffered.
Ellen responded on why she is glad to be at the forum. She would like to speak with the group to be able to plan resources. She admitted it would be a difficult task. Within the Lewisham IAPTs she mentioned they have got two priority streams. One of the streams they call priority pathways where One of them is NHS and social care and the priority stream can be tailored to support BAME carers who have been hit hard by the COVID-19 impact.
The carer member responded back stating supporting BAME carers through the crisis is only part of the problem. He felt how can black people know what IAPTs is doing? Especially for COVID-19. So they feel they can come to you when they have a mental health issue and not waiting till they’re in a crisis.
Even the internet can be a problem in itself. If you haven’t got the internet, how do you get on onto a website? So I’m just looking about what IAPTs is doing?
Ellen did completely agree that they are also concerned about people who don’t have access to the Internet and digital services. The services are hoping to open up one of our sites, so that they can do face to face work for people who can’t access digital treatment. They even do telephone treatment which works quite. There is still a lot of work to do.
Other carer members were interest in the size of the Lewisham IAPTs team and how the core element works in diversity. The carer member was interested in how IAPTs is reaching the community. Other members gave some ideas regarding churches, supermarkets and leaflets. Some members mentioned there is a problem with GP referrals and there was criticism on social perscribing in where people just get endlessly referred and not supported.
One other question I felt was interesting was from another carer interested in if there is a body? Which has overarching responsibility for your services in terms of any mental health? This then led to another question from another carer regarding when IAPTs signposts people to the other services, social services and so on. Is there an effort made to check with how that signposting is working? How did they actually make a good connection? How long? How long does it take for that person to get an appointment.
Presentation from SLaM QI Peer Project Worker
Next up to speak to the BAME carer forum was Richard Merton whose role at South London & Maudsly NHS Foundation trust is to try and improve service user and carer voices into MH services. Richard started about how they had an event in July, where the aim was to talk about people’s experiences of meaningful contact during COVID and the sort of things that might help going forward.
From that event they took that away some themes and feedbacks. One of the themes or discussions that was touched upon in that event was of how the trust can support BAME carers. So Richard reminder us that there is another event on the 8th of October and it would be great if anybody wanted to come along to that. A lot of the things that was also discussed at the last event in July was around technology and access to technology, plus some of the things that the forum had been talking about.
Question and answer session regarding Quality Improvement
One carer member was interested in the speed of action from meetings as in how long when they have decided what the outcomes are of these meetings? The carer member continued stating how will Richard or the NHS Trust be able to really take to put decisions into practice? Because he does not want us to say, yeah, we’re going to do this and We’re going to do that. And then this time next year, we’re still working for the outcomes of these, because of the situation we are were under a moment.
The response from Richard was on how things are going to take some more of a structural change. However the event is kind of a listening event based on what communities asked initially. Richard suggested that he thinks it’s always important to come back to someone and annouce what could or could not be done based on what was requested.
Another carer member issued a request stating that if Richard be sure to send information about the October event through the involvement register. Plus to make sure to use ways and other means of sending the information out and spread it as widely as possible to the community.
Another member of the forum mentioned the situation with local government and the impact on BAME carers. She felt that people are not looking at financial aspect of that being at home and having to be connected digitally. Its like having to use the internet and there is no compensation because BAME carers are having to make sure they have to stay online, to be able to be in contact with all the things that are going on in the community, but the bills are going up.
The community support member continued to mention that she has lots of clients who are actually in financial problems. As in losing money in which they can’t have the internet, they can’t be able to be involved. So what aspects are they going to help people like that, she thinks this needs to be looked at the long term due to the high risk of people losing their jobs.
Richard mentioned that NHS England, have got a branch called NHS-X, which looks at technology. And so that’s slightly will take a bit longer, but they’re looking at questions like the community support member raised. Richard also raised the point that at the trust they had a response to COVID. They have a few what they call workstreams going on and one of them is remote consultations and how we can do that across the trust.
Another carer repeated the question saying this problem with technology and paying for broadband and so on, has been going on even before COVID-19. She had to support someone and still supporting that person after she had spiralled down into severe depression. It seems that one of the causes was the person she is supporting was in serious debt, partly because of phone bill.
One of the newer carer members pointed out that the financial issues have always been an issue. And it’s a mental issue. And it’s just the way it is, and it’s never gonna change any time soon. But the question really is how you change that. And when you use the word inclusion, or what we use when we talk about community, there was a way of taking that deficit and turning it into a positive. This is what is needed to be involved in a community. So if there’s a way of paying it back then it is a sort of benefit. Because then you’re giving help to that person who then learns as if it’s an education. I have no idea why this is not happening, but all businesses should have a social responsibility
Richard mentioned how there was support from Charity especially regarding the purchase of mobile phones to help mental health staff connect more with their patients. Richard admitted charity cannot be the complete answer. Richard also wanted to say that a few of people at the forum came to an event in June, which was a big broadcast, where SLaM plan on developing work streams linking the leaders of the council’s together, and and looking at some of these social issues.
Some of the members of the forum are also members of the Lewisham BME Network, one member of the group mentioned an initative from Microsoft that is currently investing in BAME communities. She felt that it is really significant if Microsoft is connecting with some of the groups, and maybe other providers are doing the same like Virgin, or one of those. She felt that perhaps we could ask them on what they do for charities. So there’s probably things we could do in the community that would impact the way we take on the digital platform.
Other carer member raised an important point on that there are many strands to what needs to be done within the community. But if we’re talking about the individuals, within the community, black and white who are experiencing poverty and no access to the internet and phones. He thinks there’s more of a structural in political resolution to this and not just community based solutions. So maybe talking to MPs and putting pressure on them in that sphere, to look at the whole wide community as a whole, not just particularized issues that we’re raising today.
This concludes the brief update of the September Lewisham BAME carer forum.