By Matthew McKenzie – Facilitator of National ethnic mental health carer forum & Triangle of Care – Community group

The National Ethnic mental health Carers Forum (chaired by myself) met for September bringing together various stakeholders, including carers, healthcare professionals, and community representatives, to address issues related to race, equity, and care services. Key discussions included technical setups, addressing ongoing challenges in healthcare for marginalized communities, and emphasizing the importance of incorporating diverse perspectives in developing solutions for better patient experiences.
The importance of data collection, representation, and systemic change catalyzed by community engagement were recurring themes. Presenters highlighted various initiatives, including the Patient Carers Race Equality Framework (PCREF), aimed at improving services for ethnic minority populations. Questions from attendees focused on ensuring inclusivity and effective communication within the healthcare framework.
Improving Ethnic Minority Healthcare Access
The meeting introduced participants to the Patient Carer Race Equality Framework (PCREF) initiative, focusing on improving outcomes for patients and carers from ethnic minority backgrounds.
Wayne Farah, an associate at the Institute of Race Relations, presented resources available to support understanding and addressing racism in healthcare, including statistics, healthcare access issues, and practical resources for carers.
Wayne Farrar opened his talk by drawing on both professional expertise and personal experience. He explained the history of the IRR, its focus on amplifying marginalised voices, and the resources it provides such as IRR News and the Calendar of Racism and Resistance. His main theme was the persistence of institutional racism in the NHS and wider systems, which he linked to the legacy of “race science.” He argued that current approaches, like dashboards, metrics, and inquiries, often mask the real problem by treating health inequalities as technical or biological issues rather than outcomes of racism and discrimination.

Wayne used examples such as the Windrush scandal to show how bureaucracy allows injustice to persist, describing this as the “banality of evil.” He also shared personal stories about advocating for his wife in the healthcare system, emphasising that carers need to be strong and assertive because no one cares more about their loved ones than they do. He concluded with reflections on resilience, including how he has reframed being stereotyped as an “angry Black man” into a form of empowerment to push harder for change.
The discussion that followed showed how deeply Wayne’s talk resonated. Carers praised the presentation’s directness and asked if Wayne had worked with PCREF (Patient Carer Race Equality Framework). Wayne said he had some involvement through the NHS Confederation and noted that PCREF could more strongly address issues like “racecraft.” Len raised a challenge about Wayne’s framing of race as a social construct, pointing out that racism feels very real to victims. Wayne clarified that he meant race has no biological basis in medicine, but racism is a social process with very real consequences. Another carer shared her experience of being stereotyped by NHS staff about her risk of diabetes despite not following the assumed “Asian diet,” saying Wayne’s points about race-based assumptions resonated strongly with her. Another carer also reflected on how stereotyping affects healthcare, while other participants spoke of how powerful and validating Wayne’s talk had been.
Overall, Wayne’s session combined history, critique of systemic racism, and practical advice for carers. The Q&A highlighted both curiosity about frameworks like PCREF and the need to address the tension between race as a social construct and racism as lived reality. Many participants expressed gratitude, saying the presentation was direct, powerful, and reflected their own experiences of stereotyping and inequality in healthcare.
Carer Questions:
A carer challenged Wayne’s statement that race is a social construct, saying that while it may not be biological, racism is very real for victims and has a lived history.
- Wayne’s Response: He clarified that he meant race has no biological or scientific basis in medicine or anthropology, but racism is very real as a social process. He emphasised that health disparities (like hypertension in Black communities or diabetes in South Asians) are not caused by race itself, but by racism, discrimination, and lack of access to appropriate services. He wanted participants to be cautious when institutions frame disparities as inherent to race rather than outcomes of racism.
Matthew’s Question (Forum Lead):
I asked what role the Royal College of Psychiatry should play in countering race science, given its influence over professionals and carers.
- Wayne’s Response: He said that was the aim of PCREF, but royal colleges were historically rooted in race science, which is why good intentions are not enough. He criticised the frequent use of “inquiries” into deaths of Black men in mental health care as ways of delaying real change. He argued that systemic neglect persists, and professional bodies must take responsibility rather than congratulate themselves for minor improvements.
Addressing Racism in Healthcare Systems – Norfolk and Suffolk NHS Foundation Trust
As usual Mental Health trust representatives including involved carers update the national ethnic carer forum on developments.
Cath explained that race equity is now a strategic priority for NSFT, which serves a largely rural and non-ethnically diverse population where explicit racism is still present in communities and services. Under the leadership of their Chief Executive, the trust has set out a clear strategy built on improving health, care, culture, and value. To deliver this, NSFT has launched 12 large-scale change programmes, one of which previously focused broadly on inclusion but has now been reframed specifically around race equity. Importantly, this work is being split equally between workforce development and PCREF, so that both staff experiences and service-user outcomes are addressed.
She acknowledged that NSFT is still behind other trusts in terms of PCREF implementation. Their original PCREF plan, approved in spring, has already been recognised as inadequate and is now under review. Cath noted that this review will lead to a more outcomes-focused approach rather than process-driven work. A dedicated health equity and PCREF team is also being created as part of the trust’s corporate redesign, reflecting a recognition that they lacked capacity and expertise in this area. The revised plan is due to go through governance for approval in November.

Annie, speaking as a carer representative, highlighted how important it is to be “at the table rather than on the menu.” She acknowledged she can be seen as “aggressive” or “demanding,” but stressed that Cath had helped give her the confidence to challenge constructively at board level. Annie linked IRR advice about building relationships with senior managers to her own experience, saying that having a place at decision-making tables empowers carers to make sure the realities faced by ethnic communities are heard. She also reflected on her personal motivation: as the mother of a mixed-heritage son, she feels a responsibility to speak up on what ethnic families experience in practice.
PCREF Implementation and Progress Update – north london nhs foundation trust
The next NHS trust to present to my forum was North London NHS FT, which covers 5 London boroughs due to the merger of 2 large NHS mental health trusts.
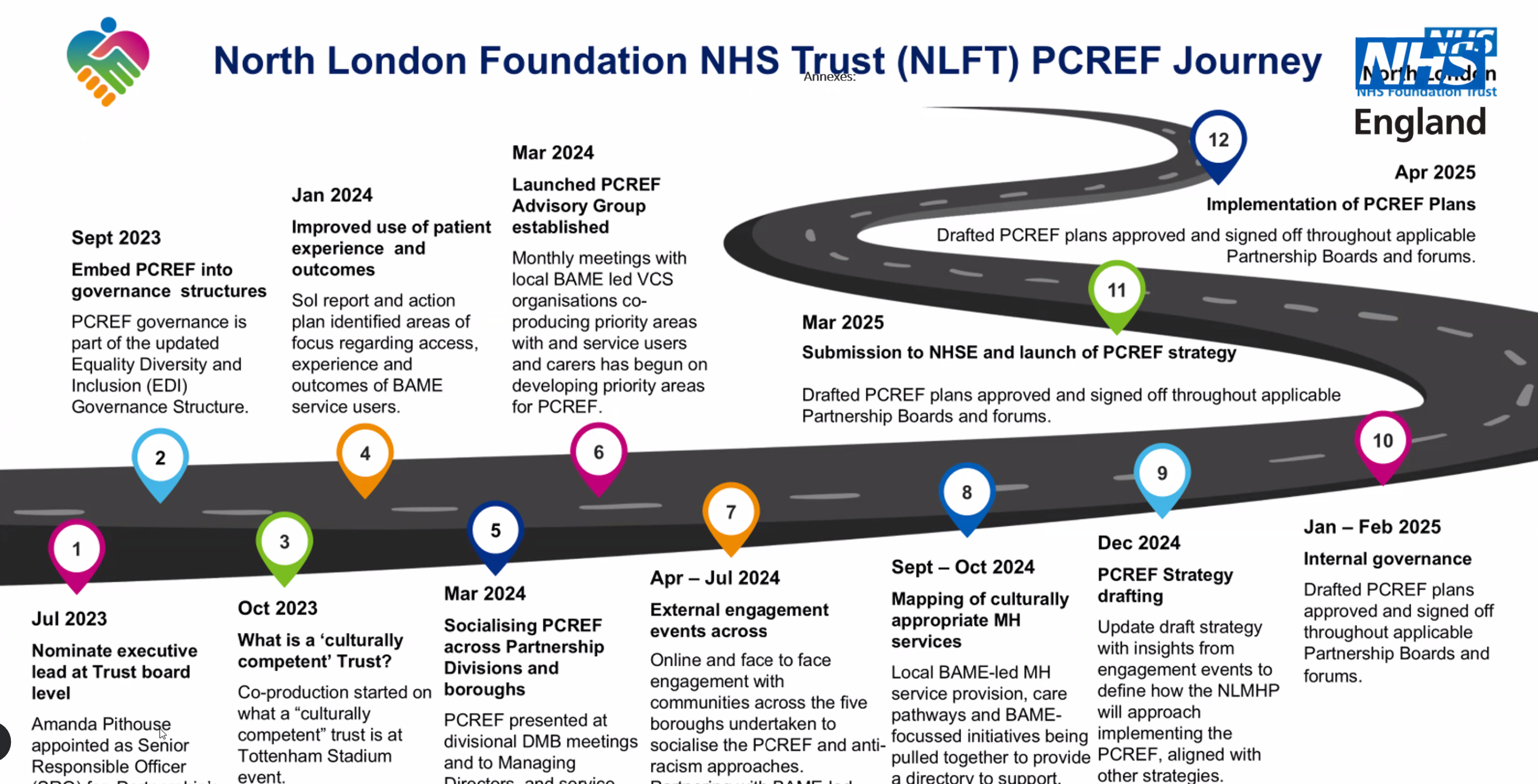
Samina Arfan, Associate Director for Equality, Diversity and Inclusion at North London Foundation Trust (NLFT), explained that her trust was created from the merger of Camden & Islington and Barnet, Enfield & Haringey trusts. Unlike some early PCREF pilot sites, NLFT only began its PCREF journey in late 2023. The first step was setting up governance structures, securing an executive lead at board level, and creating an EDI programme board. Alongside her colleague, Jordel Akinola, she led engagement events in local boroughs to ensure strong co-production with communities. These early steps gave the trust a foundation to begin shaping its PCREF plan

A major priority has been addressing inequalities in mental health detention and restraint practices. Samina shared data showing Black communities are disproportionately detained under section 2 of the Mental Health Act, while Asian people are underrepresented. Restrictive practice data revealed that Black men were more likely to experience prone restraint, which prompted a quality improvement project across wards. This included improving the accuracy of ethnicity recording, since too many patient records lacked this information. Workforce diversity was highlighted as well—NLFT has a diverse staff, but the data still shows ethnic disparities in care outcomes, making it vital to view restraint and detention through a racism lens
She also described broader initiatives: building a PCREF dashboard to apply a race lens to existing NHS targets; launching co-production projects with children and young people, including multi-faith engagement in mosques, synagogues, and youth boards; and expanding the role of peer workers, nearly half of whom are from ethnic minority backgrounds. However, she admitted feedback systems like the Friends and Family Test are not capturing enough voices from diverse communities, so peer workers and advisory groups are essential in bridging that gap

Samina emphasised the role of the PCREF advisory group, which brings together service users, carers, voluntary sector organisations, and staff to scrutinise trust data and guide projects. She stressed transparency by involving the people actually delivering the work, holding them accountable, and ensuring that community voices influence outcomes. She also acknowledged challenges: national NHS changes and funding cuts risk diluting PCREF work, so she is advocating for a North London PCREF collaborative to align efforts across local mental health providers and share learning. Finally, she noted that patients and carers with long-term involvement must be given a stronger seat at the table, as their lived experience is crucial for shaping change.
After Samina’s presentation, a carer spoke about her frustration at struggling to access clear information on the trust’s anti-racist strategy. She explained that despite being part of the Haringey Service User and Carer Forum for many years and emailing various staff, she had received little response. The carer felt this was a missed opportunity, as service-user and carer forums could be powerful spaces for embedding anti-racist approaches. She emphasised that these groups already hear many concerns from families and communities, so they should be central to shaping change, especially given the NHS’s recent shift towards more community-based mental health services
Samina acknowledged th carer’s concerns and agreed that stronger links to service-user and carer forums across the five boroughs were vital. She said the challenge since her colleague left was not a lack of will but a drop in capacity, as her EDI team had been reduced in size. To address this, she planned to personally attend service-user forums (even if only once a quarter) to ensure communication wasn’t lost and updates reached carers directly. She stressed it was about embedding the work into the system, not leaving it solely to her or the EDI team. Samina invited the carer to connect with her offline, exchange emails, and join the PCREF advisory group, ensuring carers and service users from each borough had representation. She also underlined that community connections must feed upwards into trust decision-making, rather than being siloed
Advancing Carer Equality Initiatives – Triangle of Care & PCREF, Carers UK Black History month
I closed the session by giving a short update on my wider work around carers and PCREF. I explained that I chair the Triangular Care Community Group, which meets every two months and focuses strongly on carers’ mental health. This group is working on how Triangular Care Standards can be linked with PCREF implementation, making sure that carers, especially from minority backgrounds are properly included in the conversation. I also mentioned that Carers Trust is circulating a draft for feedback, and encouraged participants to get involved and share their views within the next week

I also highlighted my role as an volunteer & ambassador with Carers UK, where I help on raising the profile of unpaid carers. I flagged upcoming events, including a Black History Month event on 13th October, organised by Carers UK, where I will be speaking at.
If you are a carer or minority carer, please book for the online share & learn session below.
Carers UK – Black History month event booking form
I encouraged attendees to use such opportunities to ask “the magic questions” about how influencial organisations will keep its focus and inclusion on minority carers
I then reminded everyone that collaboration across groups whether through PCREF forums, Carers Trust, or Carers UK, that it is vital to strengthening the voice of carers and ensuring equality.
I confirmed that the next forum meeting would be on 31st October and encouraged participants to spread the word so more carers, minority or otherwise, could join in the conversation.
Summary of the Ethnic Carers Forum Meeting – September
Multi-Angle Analysis
The meeting illustrated the deep-seated complexities of race and healthcare, revealing how institutional frameworks and practices intersect to affect service delivery and patient care. By advocating for the inclusion of diverse perspectives and leveraging collected data, participants aim to challenge systemic barriers that contribute to inequitable health outcomes. The call for community engagement underlined the need for actionable collaborations that transcend traditional healthcare models.
Technical Terminology
- PCREF (Patient Carer Race Equality Framework): A strategic framework aimed at addressing health disparities experienced by marginalized racial and ethnic groups.
- Race Science: Historical studies that claimed race was a biological determinant influencing health outcomes, which is now widely discredited.
- Weathering: A term that describes the cumulative impact of social, economic, and environmental stressors on health outcomes over time.
Key Insights
- The forum highlighted that systemic racism impacts health behaviors and access to resources, necessitating a reevaluation of how healthcare frameworks can better address the roots of health disparities.
- There remains a critical gap in understanding the complexity of health outcomes related to racial and ethnic backgrounds, underscoring the need for comprehensive retraining of health professionals regarding these issues.
- Actionable strategies for engagement with marginalized communities must be prioritized, as this will enhance the contextual understanding of healthcare needs.
- Collaboration between organizations, local communities, and health professionals is essential for effective reform in healthcare delivery systems.
- Continuous dialogue and reflective practice can lead to transformative outcomes within healthcare services.
FAQ
1. Why is the discussion surrounding race so critical in healthcare contexts?
It is essential to address the impact that systemic racism has on health outcomes, access to care, and the overall well-being of marginalized communities. Understanding this context helps healthcare systems provide more equitable and effective care.
2. What is the significance of the Patient Carers Race Equality Framework (PCREF)?
The PCREF serves as a guiding structure to ensure that care systems consider the specific needs of ethnic minorities, aiming to reduce health disparities and improve outcomes through focused strategies and policy implementations.
3. How can community engagement improve healthcare services?
Engaging with communities allows healthcare providers to gain invaluable insights into the unique challenges they face, leading to tailored interventions that address these barriers effectively.
4. What steps can healthcare professionals take to address institutional racism?
Healthcare professionals should actively engage in ongoing training regarding cultural competency, advocate for equitable policies, and ensure that their practices do not perpetuate discrimination.
