By Matthew McKenzie – Triangle of care chair
Below is a brief update of the group meeting, which was set as a national engagement space for carers to share experiences and influence Triangle of Care implementation and wider system change
1 “What’s Changed for Carers” Discussion
Carers shared real-world experiences, highlighting both small improvements and ongoing systemic challenges.
2 Triangle of Care Update
Presented by Mary Patel: Update on national progress, including growth in membership, quality improvement work, training, and ongoing efforts to embed carer involvement across services.
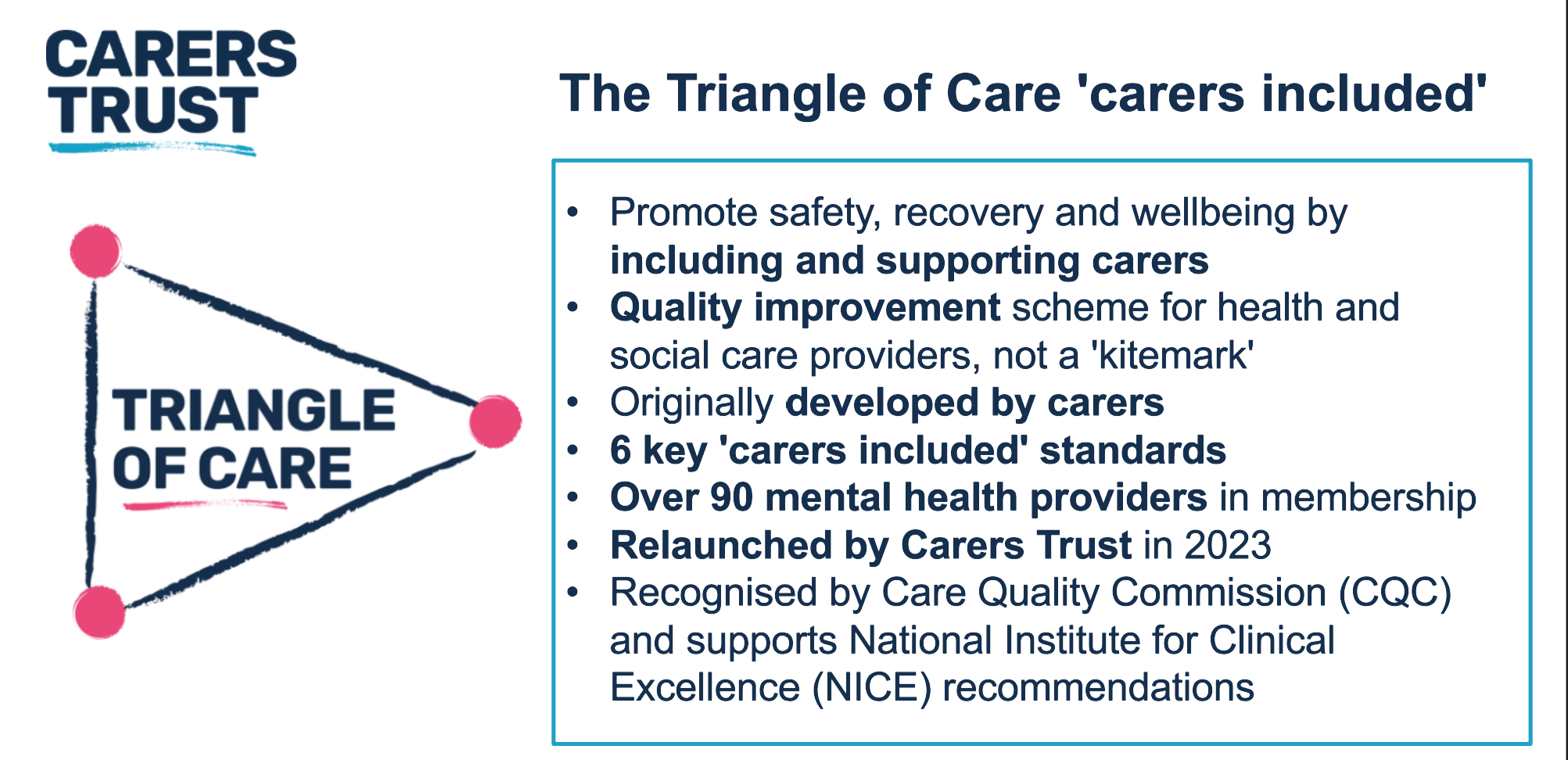
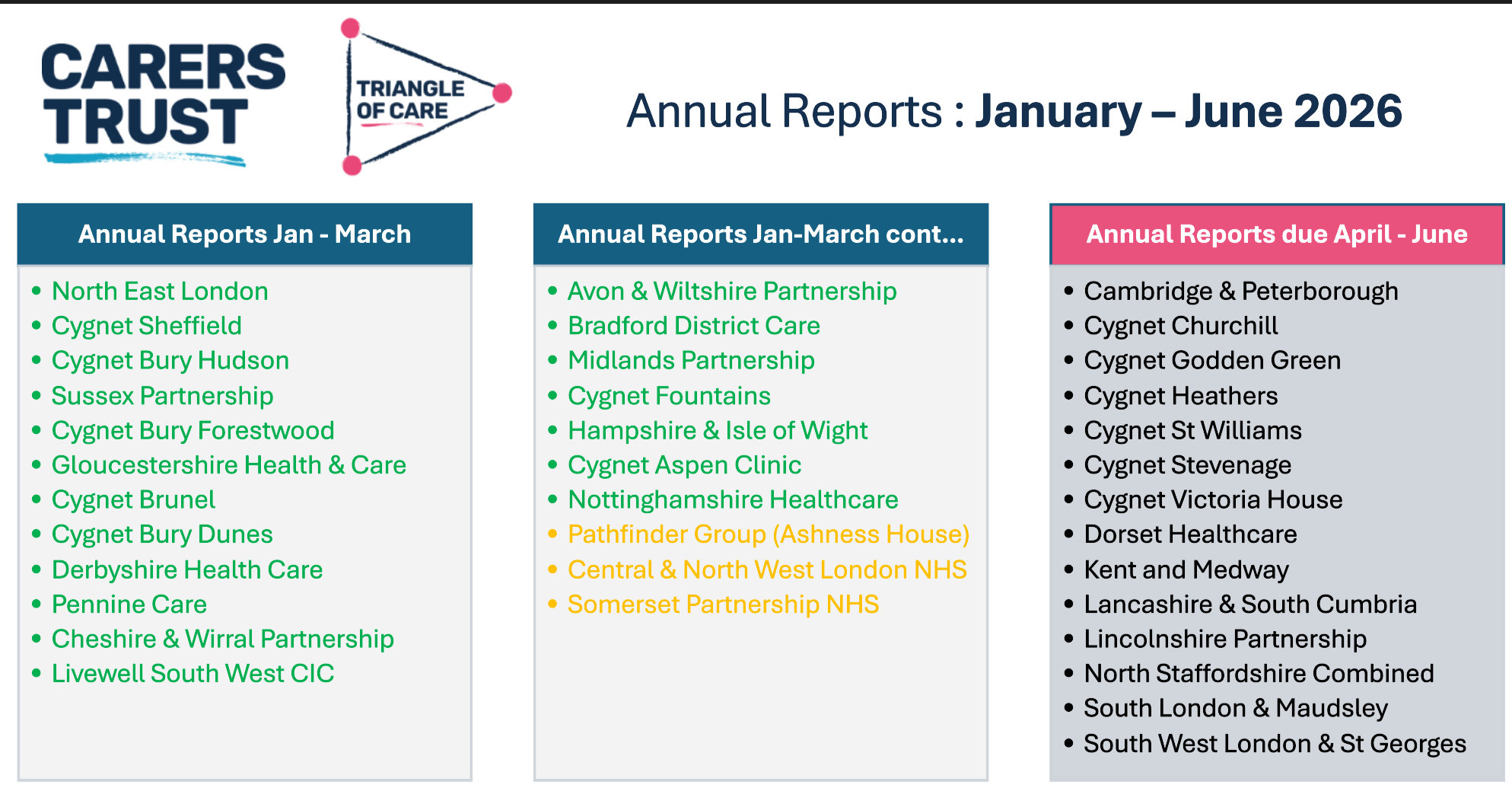
Membership growth: Over 90 mental health providers are now members, with new applications from East London Foundation Trust, North London Foundation Trust, and several private providers, demonstrating a steady expansion of the scheme. Quality improvement process: Providers submit annual reports, self-assessments, and evidence for review.
Mary highlighted the STAR award system (STAR 1: inpatient/crisis teams, STAR 2: community teams, STAR 3: additional health services), celebrating recent awards to Leicestershire Partnership Trust (STAR 2) and Merseycare (STAR 3), noting the significant carer involvement in these assessments.
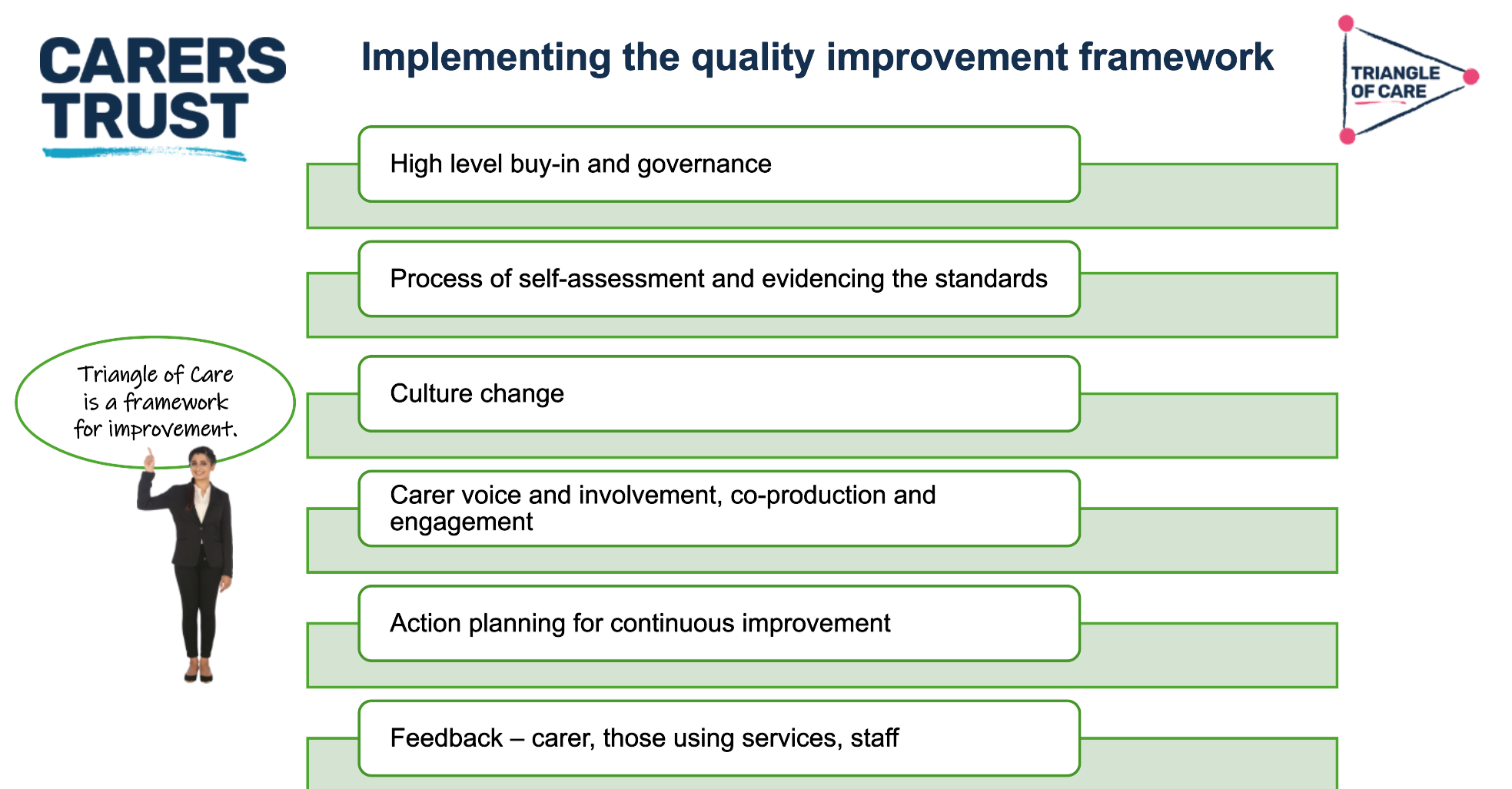
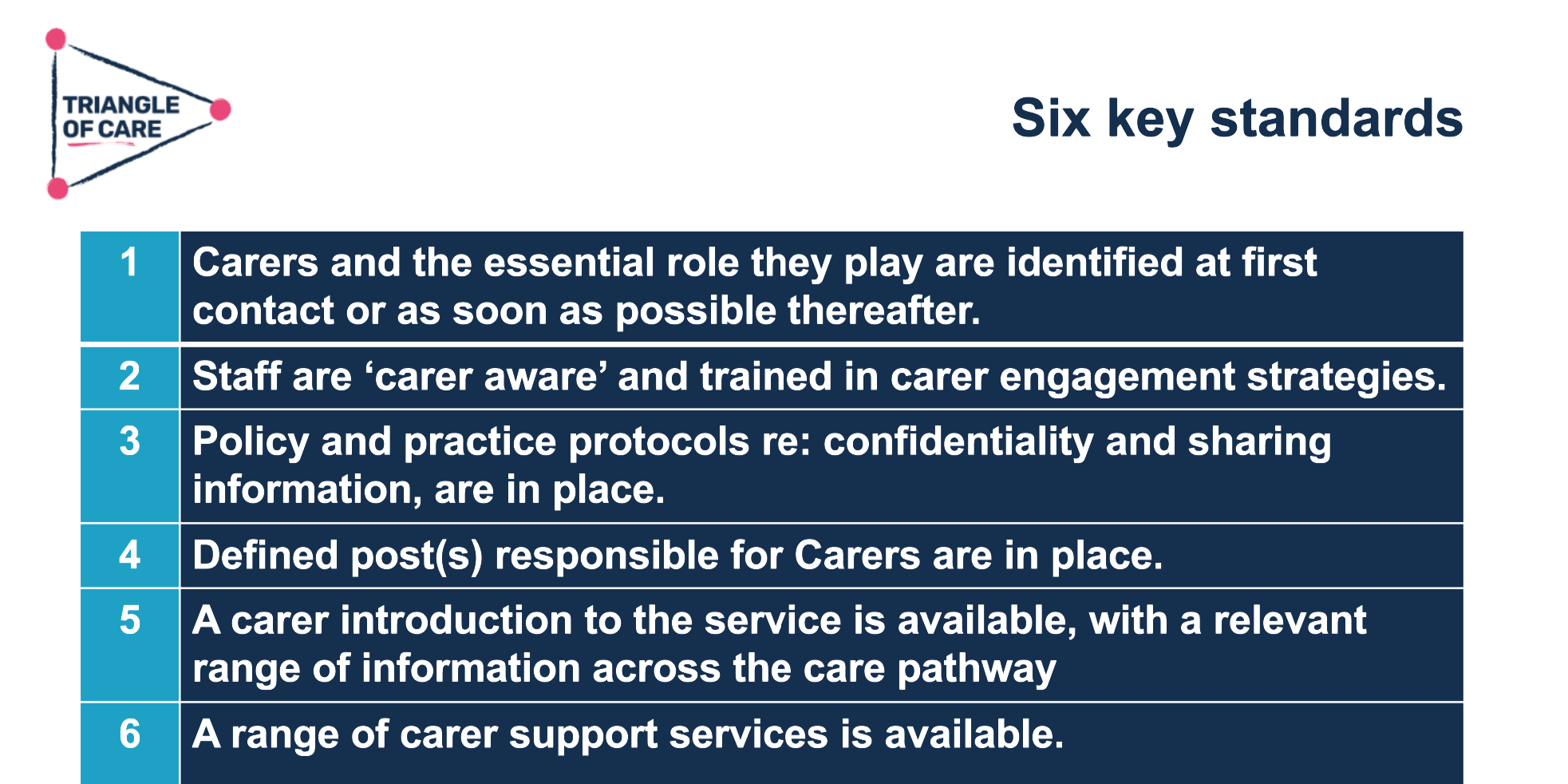
Embedding standards: Triangle of Care standards remain the six core standards developed with carers in 2010, underpinning governance, carer involvement, action planning, culture change, feedback mechanisms, and co-production. Mary emphasised that self-assessment is a reflective improvement tool, not a quality mark. Culture change initiatives: Focus on carer awareness training, senior leadership engagement, and the “golden thread” of carer involvement throughout services. Support for members:
New initiatives include:
- Community of Practice forum for sharing best practice
- Online self-assessment training module
- Ongoing webinars, events (e.g., Young Carers Action Day, Caring Across London)
- Draft social care guidance and upcoming Triangle of Care + PCRIS pilot
Policy engagement: Mary highlighted alignment with the Care Act 2014, Health and Care Act, and attention to equity, inclusion, and workforce development.
3. Influencing & Accountability (GPs / Commissioners)
This section was led by Matthew McKenzie, with supporting input from Mary Patel. The focus was on moving the group beyond discussion into practical influence and system change, particularly around primary care and commissioning. Matthew outlined the intention for the community group to act as a bridge between carers’ lived experience and decision-makers, identifying key issues raised by carers (especially around GP services and discharge pathways) and using the group to bring in external stakeholders such as GPs, commissioners, and national bodies.
4. NHS England – Modern Service Framework
This section was presented by Anne Heneghan from NHS England. She provided an in-depth overview of the 10-year Modern Service Framework for Severe Mental Illness, describing it as a “moonshot” designed to improve outcomes for people with severe mental illness by 2035. The framework focuses on three overarching pillars: improving health and wellbeing (including reducing physical health inequalities), delivering high-quality, person-centred, and integrated care, and supporting independence and social inclusion through housing, employment, education, and community connections.
Anne highlighted that integration across services is central, bringing together mental health, primary care, social care, the voluntary sector, and justice system interfaces. A key focus is co-production, with people with lived experience and carers involved in shaping interventions, standards, and service delivery. She explained that the work has moved into a call for evidence phase, inviting stakeholders, including carers to provide input on the interventions and best practices that should form the core of the framework.
Anne also addressed ongoing systemic challenges: there is currently no confirmed new funding, workforce pressures are high, and fragmentation between health, social care, and primary care persists. She stressed the framework’s role in tackling inequalities, including racial disparities in care and outcomes, and ensuring that carers’ perspectives are central to the design of services. Anne outlined the phased approach, including stakeholder engagement, evidence review, intervention prioritisation, and eventual quality standards development for three care settings: community, crisis/urgent care, and inpatient care. She emphasised that the framework is designed to be ambitious, evidence-based, and flexible, with iterative updates over the next decade to reflect learning and emerging best practice.
Questions from carers:
- What happens if political priorities or government structures change during the 10-year plan?
- Will additional funding be allocated to support these interventions?
- How will integration between NHS, social care, and other sectors be achieved in practice?
- How will carers be consistently involved throughout the framework’s delivery?
- What mechanisms will ensure long-term accountability and follow-through?
- How will racial and other inequalities be addressed, including treatment disparities?
Carer Peer Support (Guest Speaker)
This section was led by a carer, who shared a practical, grassroots example of setting up and sustaining a carer-led peer support group in Bristol. She described how the group evolved from a time-limited programme with Rethink Mental Illness into an independent, ongoing support network run entirely by carers. The group meets monthly, is built on trust, confidentiality, and mutual understanding, and operates without formal funding highlighting both its value and the limitations of relying on voluntary effort. She emphasised that peer support groups can be highly impactful but are often poorly attended or unknown, despite large numbers of carers in the community. She also highlighted the importance of flexibility and inclusivity, noting that groups may work best when tailored (e.g. by age, gender, or cultural background) to build trust and relevance. A key message was that carers themselves often need to be proactive in creating support, as services do not consistently provide it, and that there is an opportunity to grow and connect more informal, community-based networks.
