Hello visitors and those providing care or caregiving to someone close. Here is another carer awareness blog from Matthew Mckenzie, carer activist, poet and author from Lewisham.
This blog is about Carers Lewisham Hub’s culture day. Carer centres are a vital part of providing support and services for those giving unpaid care. Carers Lewisham fights hard to identify carers, advocate for them and give as much support as possible.
I often visit the carers centre for their forums and support groups. On the 28th of July 2022, since the borough of Lewisham was the borough of culture. Carers Lewisham was hosting their culture day at their carers centre. A list of activities, networking and events was provided for carers who wanted to feel valued.
We had the game room and Raffle ticket event. Massage for those who have stress, aches and pains. Creative art sessions for those wanting to be……well creative. We also had laughter workshop, book readings and also my poetry reading (more on that later.)
I think most of all, carers who came along to the event wanted to network with others. They wanted to reduce isolation and link up with carers, staff and advocate to get support, information and to feel valued.
Since my poetry book “The Poetry book of mental health caring” was released in July 2022. Carers Lewisham was kind enough to offer me a poetry workshop. It is well known that over time, poetry can contribute to forms of culture. Most if not all my poems focus on the aspect of the caring experience. The poems look to raise the awareness of those providing mental health care. That means providing unpaid care to someone suffering mental illness.
At the book reading and poetry workshop, we had other carers reading from their poems which they have developed. Tess read a wonderful poem and also Brenda.
I ran my workshop by reading a poem and then asking others to also choose a poem to read. We then reflected on the meaning and definitions of those poems. You can see the video of my poetry workshop below.
Hello fellow unpaid carers, new blog from Matthew McKenzie carer activist. I have not blogged in a while, because I am so busy writing my books about unpaid care. The thing is, while I am writing stories about the experience of providing care, I could not help think about the term ‘carer’. I could be more clearer and say what does the word ‘carer’ mean.
If i Google the term ‘what is a carer‘ The following turns up.
Wikipedia states the following
“A caregiver or carer is a paid or unpaid member of a person’s social network who helps them with activities of daily living.”
NHS England focuses the word ‘carer’ as the following.
‘A carer is anyone, including children and adults who looks after a family member, partner or friend who needs help because of their illness, frailty, disability, a mental health problem or an addiction and cannot cope without their support’
Come to think of it, if I google the word carer then most if not all of the following links agree with NHS England’s definition of a carer. The following links (subject to change) are from
Bristol and South Gloucestershire carers centre on “What is a carer” Caring together – Cambridgeshire on – “who is a carer” Carers Trust on Caring as an Unpaid Carer Even the citizens advice site has a section on Carers: help and support
So ok, why am I blogging about the definition of carers? Well as you can see things are not all that simple. Get ready because it gets political, but that is nothing new here.
The word ‘carer’ is shared depending on who uses it and why they are using the word. As far as I know, carer workers use the term carer. I run a carers stall at some hospitals and people often come up to me asking the following.
“Do you have the number of a carer to help with looking after someone?”. I then explain the stall is for unpaid carers.
Others ask
“Do you have a job for working as a carer?” “How much does it pay to be a carer?” “Can you be my carer?”
Well, the above highlights there are some concerns, because to be fair paid carers / careworkers do care for people, but they are paid to do so. We also have to notice the word ‘carer’ carries with it a vast amount of prestige. It becomes political if people hijack the word to push out those who are providing unpaid care. There is a tug of war between those who want to be defined as carer. Do not get me wrong, as many in the professional sector are vocal that the word should belong to unpaid carers. Still, another problem I am aware of is that those providing unpaid care do not often recognise themselves as a carer. Some even deem the word as an insult because they are caring for someone as a family member and want to be recognised as that first. This is fine and there should be little arguements of this, except what happens if the person continues to struggle providing unpaid care? They are not recognised by certain health and social care systems as needed support.
With the blurred term of ‘carer’, it means not only the carer suffers, but the person needing the care might also suffer because the strain on the family member becomes challenging. We also now have the word ‘carer’ being used for those who work in the NHS. It is true nurses and doctors ‘care’ for their patients, but even that causes problems because what happens when a health professional has to provide care for someone at home or close to them? How would they be identified? Would the strain of care push them out of the health profession?
It gets worse, even if you someone become aware you are a carer caring for someone in the family, what are your duties? Another google search of “carer duties” or “duties as a carer” brings up the duties of care workers. So someone provding unpaid or informal care will get stuck, because sometimes they have no idea what to do.
This is all confusing, I do not have the answers and I am sure someone out there does. Come to think of it, The care act 2014 is under scrunity. The House of Lords adult social care committee released a report in December 2022. The report mentioned that the government’s white paper does not go far enough.
There is a risk more unpaid carers and those they provide care for will suffer. It was stated that more support from health and social care professionals is needed to identify unpaid carers. As too many carers lose out on support, even if referred a large number might not be able to access support. I did warn it would get political.
To be honest, my thoughts on solutions would be education, education and campaigning. The big hurdle is getting others to scream that they are carers and that they need support. The cost of living, strain on health services and pandemic have highlighted the need for unpaid carers to get support. If the NHS continues to struggle it can only mean one thing, the community has to pick up the slack. That means carers will have to do more and also understand the health and social care system.
You can read the House of Lords adult social care committee report below from section 123 – What does it feel like to be an unpaid carer today?
Coming out of hospital checklist – This will be useful for my carer stalls at hospitals. This helpful checklist on what should happen before the person is discharged into someone’s care.
Welcome to a very late update of one of my carer forums. These are updates of the groups I run whose members are those caring for someone with mental ill health. For my September SW London carers forum, we were joined by Professor Caroline Glendinning who is the Emerita Prof of Social Policy at the University of York.
Prof Caroline presents on Carers and personal budgets
Caroline thanks us for having the chance to engage with unpaid carers and a way to learn from them. She was interested in our personal experiences, especially from the experience of caring for someone with a mental illness. She was pleased to see there are carer led groups fighting to engage with services.
Professor Caroline spoke at length regarding how Personalisation and carer policies have developed separately. She mentioned what the choices are disabled people, being either direct Payments/Personal Budgets/Individual Budgets.
She then spoke a bit about Carer’s rights being the importance of having a carer’s Assessment, how Carers Allowance Support should work and also the need for carer respite.
Professor Caroline gave some examples regarding cash schemes, but also highlighted some problems. Comparisons were from the following.
Where schemes were designed to support carers (Germany / Austria) Plus some plans aim to increase choice for service users (England/Nlds)
Professor Caroline then moved into what trigger her research into these areas. These were “How do local authorities recognise/balance the rights, needs and wishes of service users and carers?”.
She wanted to find out what roles should carers play in assessment /planning support? Carers at the group were interested if there was there any consultation or involvement that was flagged up by her research.
Professor Caroline surveyed many Local authorities by running.
Lead officer interviews Focus groups with front-line practitioners Interviews with service users and carers
The results from her research lead to several findings, which Professor Caroline explained at length to the forum.
Joint/holistic family assessments desirable – carers usually involved
In practice assessments focused on service users – little attention to carers’ needs, apart from ‘willing and able’
Carers offered separate assessments but low take up
Even where separate carer assessment done, little consistent practice in bringing 2 together
Service user budget reduced by carer support
No guidance on carers’ role in planning service user support
Carers often involved in managing service user personal budget
Carers’ organisations not involved in developing personal budget policies/practice
Poor coordination of subsequent reviews of service users’ and carers’ needs
Discussion time from the group
Professor Caroline wanted to find out our experiences in regards to her research paper. There was a lengthy discussion on the following.
What were members experiences? Any feelings regarding Assessments How did people feel about Planning support When did Reviews take place?
Professor Caroline then spoke about the conclusions of her research
Carers not involved in developing personal budget policies/practice Failure to assess carer needs: Just asked ‘willing and able’ Too few separate carer assessments Service user budgets routinely reduced because of carer help Funds for carer breaks included in SU budgets
This was a brief update to my SW London mental health carers forum.
Welcome to the latest update of my Greenwich mental health carer forum. I run this with the support of Greenwich carers bi-monthly. The focus of the forum is to give unpaid carers a chance to query, understand and focus on the complex world of mental health provision, especially trying to influence mental health providers of the importance of unpaid carers. In a sense, carers can be service users as well, so services should take account families and friends supporting those with mental ill health.
Speakers for the October Greenwich forum were
Peter Ley – Oxleas Greenwich Service Manager Myles Thorpe – Voice & Engagement Officer for Greenwich Area Involvement Network Jason Mcculloch – Service Manager, Commissioning, Health & Adults Services for Royal Borough of Greenwich
Peter Ley Updates MH carer forum
Peter talked to our group regarding the work going on between Oxleas and Bromley, Lewisham and Greenwich mind in order to create a well being hub. Peter explained that basically, it’s a merging of those kind of services, to kind of provide something for people where there is an easy to access. So when you go to a GP service, or maybe you just want to drop some concerns, what they are developing is a hub of different types of interventions for people that can be accessed really quickly
The intention is to provide people with prompt access to things that will help on their mental wellbeing. The idea is that rather than go through a kind of long drawn out process of repeatedly being assessed for mental health, the idea is to get to something that’s helpful intevention and be quite quick about it, provide things to people in a matter of days, rather than months. This is opposed to when a situation gets worse, then more kind of time has to be taken to get service users back on their feet.
Peter then mentioned how the pandemic is still impacting the NHS. The impact certainly has been felt from a community mental health team point of view, so they coming back into a greater number of face to face visits at home, rather than using the phone or waiting for people to come to them. So people should notice where there’ll be more of contact that is actually face to face. There should be more home visits. Something new were put in place to help with that is something called “The Care Teams Approach”.
So across all the community teams in Oxleas e.g. psychosis teams, the intensive case management for Psychosis services, what they will be doing is getting two care coordinators together and supporting them two support workers. So the kind of caseloads will spread across four people rather than one. So caseload sizes that those four will be looking after will workout to, ideally 50 patients, but in some cases, is 65. The standard there is that each of those workers does at least 10 to 10 face to face visits each week, which should instantly increase the amount of face to face visits that people can expect to get across the month in the community.
QUESTIONS FROM CARER MEMBERS
I’m understanding correctly, your well being hub, I noticed that it’s still a trial at the moment. But the referrals, are you saying that the referral has to be done via the GP? From my personal point, they cannot manage the services that they’ve already got. I’ve got health problems at the moment, and I’m struggling for myself, if I had to reach out about the person I care for, then the chances are, for example, I call trying to get an appointment on an urgent need. When there’s no appointments, you get referred to the Greenwich hub, they call it a Greenwich hub. And all what they do is triage you over the phone, and then refer you back to the GP anyway
You said it’s two CCOs and two support workers. Are they permanent staff, or are they locums? Because Oxleas seems to me to be running on locums. At the moment.
Peter we have not seen you for a while, we do hope you can engage with mental health carer groups, so there is an understanding of how Oxleas supports and engages with carers.
I myself asked the following questions
Who leads regarding care coordinators and social workers? If a Medical director leads regardings psychiatrists, then does Oxleas have a director of Social care? Although I understand care coordinators can be a generic role, plus what sort of training do staff at Oxleas get regarding carer identification and engagement?
Bonus update from Debora Mo – Mental Health Commissioning Support and Engagement Officer at SE ICB
Debora updated that they are conducting workshops with clients in a range of supported accommodations in Greenwich. So mainly from bridge support, one housing and Sanctuary. They already had their first workshop but they would like a couple of mental health carers to join if they were able to. There was a contribution for lived experience people, which is London living wage level. The sessions are held at the “London Marathon playing fields” (https://www.accessable.co.uk/venues/london-marathon-playing-fields) and the next one is on the fourth of November. They can only accommodate about one to two carers because the facilitators they are working with are really keen that the group of people who actually have the lived experience.
Myles Thorpe on the focus of Greenwich Area Involvement Network
Myles introduced himself regarding his work with GAIN. Myles mentioned it’s a was Community Action Group that worked closely with Oxleas and various public mental health bodies to improve representation of seldom heard groups, this means lived experience of mental health users to engage with the service providers. So this is incorporated in the decision making and service provision. The goal is to improve access to mental health services.
GAIN recently registered as a charity, and Myles is their first member of staff. He is doing research essentially, in connecting with various communities. There’s a whole number of groups, networks and subgroups where all of the information that they gather, whether that’s on service users or members of the community, gets fed into a kind of working group. They try and bring the provision of mental health forward so that it’s fit and efficient based on the resources that they have in the community.
QUESTIONS FROM CARER MEMBERS
It’s good to hear that carers are going to be involved and I hope fully involved, not not just as an afterthought, which we feel we are at the moment.
Wasn’t there a recent event regarding GAIN? I was wondering that turned out?
So Myles and myself sit in different things together, apart from the fact we do communicate a lot, but we also sit in different meetings that involve others like Oxleas and BLG Mind. So we are trying to focus on a united front, in a sense of all the work that’s happening, and also share all this information and knowledge.
Jason Mcculloch updates on Royal Borough of Greenwich Carers Strategy
Jason talked about what his remit covers, which is a number of service areas, but unpaid carers is one of them. He has been coordinating the delivery of a new carer strategy for the borough of Greenwich, this is a joint carer’s strategy with health colleagues, which was launched formally a couple of weeks ago, down at town hall. The launch was followed up with an event at Greenwich carer center. They are now planning further events in the evening, where the date is to be confirmed.
Jason was at the meeting to let everybody know that they have launched this new carer strategy that they are now moving into the sort of implementation phase of that strategy.
One of the key aspects of the strategy for Jason is that carers should receive a consistent level of service regardless of where they connect with health and social care services across the borough. So whether it’s at the GP, whether it’s with a social care team, either at the carer forum or with Oxleas, whether whether it’s a hospital, and you should expect the same basic level of service, the same sort of consistent information and advice.
In the background to make sure that colleagues across the health and social care sector and are aware of the strategy. We need to make sure they are aware of the commitments within it and understand what services are available for carers, which you can access or can be referred to. So as of this moment they are starting that work now, talking to the various social work teams getting engaged with GPS, and so on.
QUESTIONS FROM CARER MEMBERS
I’ve done so much for my son in the last two years. And I sit my listen to all these promises, and all the research and projects that have been done. And I’ve heard it all before they come and they take information from us, and then we don’t see them again.
Were there any mental health carers on your working working group? I was on this for 4 or 6 years ago, I was part of the original carer and strategy working group that you were setting up, but it all fell apart and I never heard anything more about it. Will there be more focus on mental health carers this time?
Welcome to an update from my unpaid carers blog. Recently I attended Lewisham Carers Hub event. They are relaunching their carers forum, which is a great way for unpaid carers to connect, network and voice their feedback.
Lewisham Carers Hub provides a range of services including advice, information, emotional support, short breaks, opportunities to meet other carers to reduce isolation and build resilience.
The event was chaired by Sue Stockman – Director of carers services. Sue listened to carers carefully and responded very well to queries and concerns. With the relaunch of the carers forum, Carers Hub Lewisham wants to be more inclusive and give carers a chance to co-chair the meeting.
I was excited to hear about work to promote a carer’s charter developed in conjunction with unpaid carers. A carer’s charter helps carers and others know about carers rights. I also learned about IT development support for carers struggling with digital literacy and upcoming services at the carers centre including carers counselling service, health and wellbeing activities and cost of living workshops.
At the forum was Tristan Brice from Lewisham council. Lewisham council wants carers to feed back on recommissioning and also wants to hear from carers about carer identification, carer assessments and other things.
Lewisham Carers Hub are also going through a rebranding process and I have included part of the branding below. There will be more to come.
In the end I thought that well attended with many carers contributing their thoughts and suggestions. I feel having a carers forum shows how a carers centre can give carers a voice and a say on what helps them overall. So even though it is early days, we can see how the carers forum develops.
Been a while since I did a carer forum update, but felt I should do one otherwise I would be distracted by something else. Here is the brief update of my ethnic mental health carer forum for September 2022. The forum is aimed at those from an ethnic background caring for someone with mental illness.
The speakers for September are listed below
Madeleine Oakley on her Kings College London carers peer research group
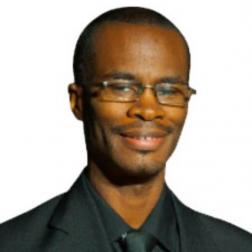
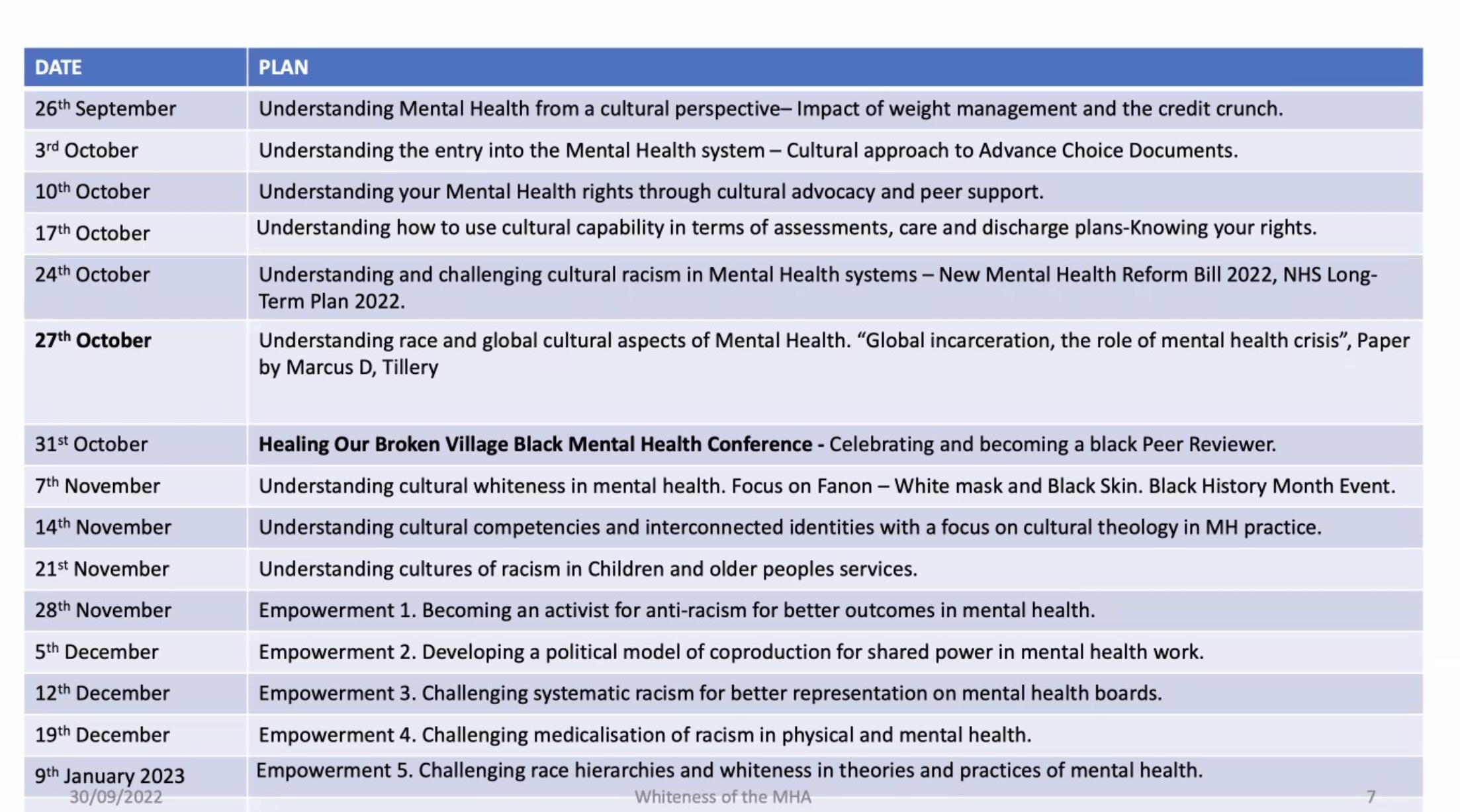
Colin King presenting on the Lancet report – Whiteness, madness, and reform of the Mental Health Act
Louise Goff on the Kings college London Health promotion Heal-D: a culturally-tailored diabetes self-management programme for adults of African & Caribbean heritage
Madeleine Oakley presents on her carers peer group
Madeleine from Kings College London has been using her skills as a psychotherapist to give people space to talk about their experiences, she has found that carers really appreciate connecting with each other. Madeleine also has the lived experience of caring for somebody with autism. Her groups have been for people who are caring for a family member who has got autism. So she started with autism and eating disorders, because there was a lot of research going on about that at the South London and Maudsley.
She is now doing an autism and psychosis carer group. Which is once every Friday morning, a month. Madeleine stated that unfortunately it does clash with my group one Friday morning, but basically, the next one is on the 23rd of October. The latest one has already started in September. Madeleine hopes members of my group can help spread the message.
Madeleine has also been interviewing family carers of people with autism and psychosis. So they’ve got both conditions that people are looking after. She is trying to explore the experiences of carers. How did they get the assessments? How did they get the treatments, how was being a carer affecting their lives?
Questions from carers
I started off asking “Is this group indefinite or is it just runs for a set period?”
Madeleine responded
The she wishes it was indefinitely. They are always looking for more funding, but it’s only until the end of March. So it’s a short thing as it is basically part of her PhD. But at the same time, she is applying for funding to sort of make the carers group permanent because the sad thing is all the work that she has done with carers since 2019, when she finishes her PhD, then where is the group going to?
Colin King presenting on Whiteness, madness, and reform of the Mental Health Act
Colin explained that he was sectioned schizophrenia within Maudsley many years ago, but what he was really concerned about was the whiteness within the theoretical and diagnostic framework was leading to historically the over representation of particular groups.
This led Colin to do an analysis looking at the start of something called cartwright 1851, which is the first diagnosis of race, which is when the black person ran away with slavery, they were diagnosed with, with depomania, and if you do the travel on the lunacy Act, at the mental health Act to the white paper Act to the White Paper review, Colin mentioned that we still got an over representation or of communities in the mental health system.
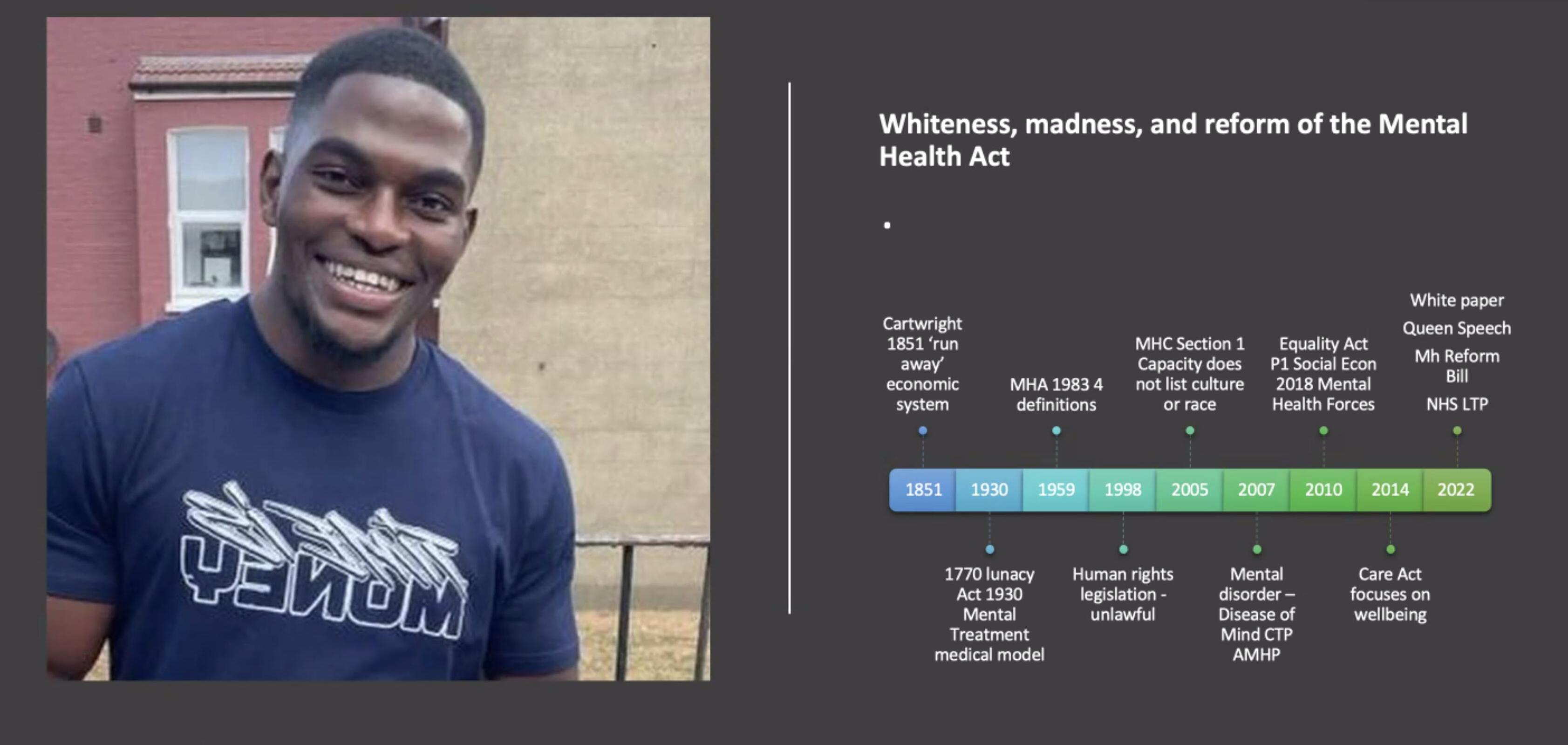
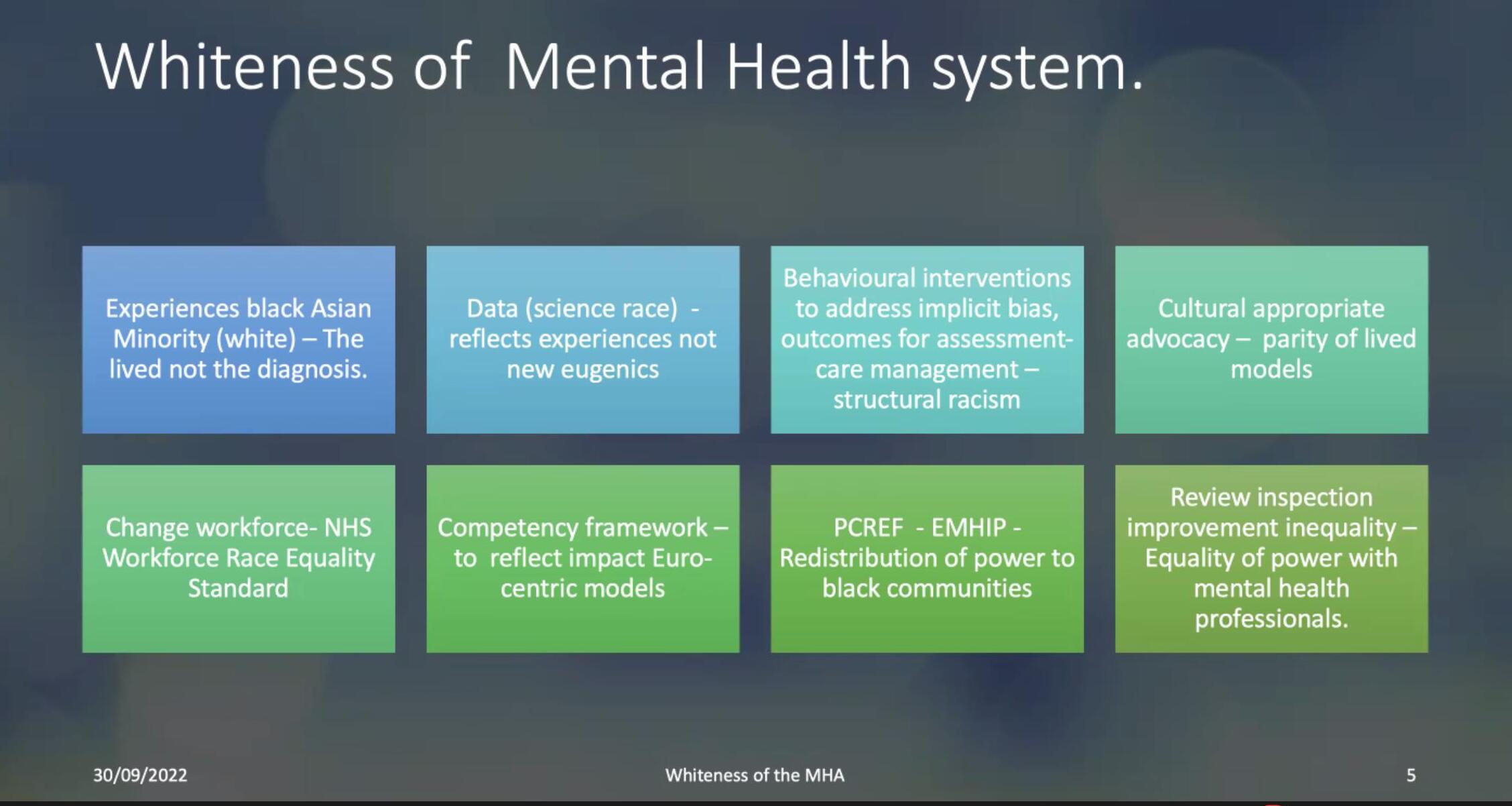
Colin wanted to understand what was whiteness, what why was whiteness, such a pervasive, intrusive and powerful intervention is in terms over representation.
Colin stated that some of it can be located in the history of theories of psychology and psychiatry that perpetuate eugenic theories about the black body and the black mind. And these theories emerged in the period of slavery, when there was a perpetuation of a division between what was whiteness as superior, and blackness as inferior. And these are some of the writers from Cartwright perpetuate his idea. Colin mentioned that even Henry Maudsley who ran the Maudsley had perpetual eugenic ideas about race.
Colin was really concerned about what the outcome this lead into in terms of particular types of whiteness, and the outcomes for diverse communities over the last 400 years, but particularly where we are with the activism for the PCREF (Patient Carer Race Equality Framework) and other campaigning groups.
So Colin began to analyze two diagnostic frameworks in terms of why they were leading to these race diverse outcomes, DSM-5, and also ICD-10. Colin mentions a book where whiteness contributes to the legalization of race as a diagnostic framework.
This leads to a problems with ideas that black people are much more naturally disordered, and what’s more psychotic. Colin felt that as activists, instead of trying to change the diagnostic framework, we should try to improve the system rather than dismantle it. THe main concern he was looking at, was community treatment orders.
And the data has continued to show that a particular groups are over represented are usually black Caribbean men, South Asian patients, women, but the biggest concern for him was why is it in 2007, when they introduced something called Community Treatment orders that 92% of them are used in relation to black men. And why is it with restraints show 75% of them have been used in relation to men. So Colin wrote a paper and it was really a plea for the abolition of community treatment order which he interpreted as a new type of slavery in mental health care and needed to be changed.
Colin spoke about the importance of being an activist, but also allowing lived experienced from the community to be involved in training and raising the importance mental health in the communities. Colin mentioned we all have something to contribute and if MH systems and beyond including schools, housing and communities services do not include minority lived experience then it hurts the community as a whole.
Louise Goff presents on a culturally-tailored diabetes self-management programme for adults of African & Caribbean heritage
Louise started training as a dietitian about 25 years ago, and then she went straight into a research career all focused around type-2 diabetes. This was on how nutrition and food affects diabetes, how it can prevent diabetes, how it can treat diabetes, She has been doing that for about 25 years now. However through her education, she was well aware that rates of diabetes were were significantly higher in people from African and Caribbean backgrounds, as well as in other minority ethnic backgrounds in the UK.
She then became really aware of contradictory messages from her professional colleagues compared to her own family and my social network. The messages that she had from her professional colleagues and network was that, people weren’t showing up for their diabetes appointments, and therefore, they didn’t care about their diabetes. This was particularly common in people of African or Caribbean heritage. And so there was this perception that diabetes wasn’t thought to be serious and wasn’t cared about. Speaking to her friends and family, particularly people who had diabetes, were so fearful of their diabetes, and so worried about their diabetes, and really wanted information about how to improve diabetes, how to avoid diabetes.
So that really led to her wanting to focus her research career more towards understanding that situation and understanding on what is going on in the health system. And what is going on in the communities. She has been using her research platform to try and unpick and work towards trying to improve that situation really. A while back she received some research funding to develop diabetes self management program specifically tailored to the needs of adults from African and Caribbean backgrounds
The project has the following skills
• Group-based • 7 sessions of 2 hours – 1-hr educational discussion & 1-hrexercise class • Delivered weekly • Delivered using video conferencing • Dietitian & community facilitators
The program is called healthy eating and active lifestyles for diabetes, or abbreviated down to heal D, but it’s a self management program that’s been developed to help people who are living with type-2 diabetes, to really understand what they need to do in their self management. In terms of diet and physical activity and other lifestyle components to improve the management of diabetes, all the while specifically tailored to African and Caribbean culture.
The program is called healthy eating and active lifestyles for diabetes, or abbreviated down to heal D, but it’s a self management program that’s been developed to help people who are living with type-2 diabetes, to really understand what they need to do in their self management. In terms of diet and physical activity and other lifestyle components to improve the management of diabetes, all the while specifically tailored to African and Caribbean culture.
Louise stated that this is about cultural health beliefs, cultural foods, cultural practices around food and physical activity and body weight. And all of the things that we know about medications and all of the things that we know that are related to diabetes management.
Louise continued she is actually following on from the really important messages that Colin was just sharing with us. when she went about developing this program, she knew that it was the people with the lived experience who were the experts through their lived experience that really needed to lead this project to understand what was needed in a program that would really support people.
So all of this work was done using a sort of community partnership approach, whereby they engaged with our communities, and this was conducted in southeast London.