The recent Carers Forum brought together unpaid carers, health professionals, and community organisations from across South London to share updates, experiences, and ideas for improving mental health support. The event, chaired by Matthew McKenzie, created a safe and open space for carers to connect, exchange information, and have their questions heard by local health leaders.
Setting the Scene
Matthew opened the session by welcoming carers from across Lambeth, Lewisham, and Southwark. He spoke about the importance of providing carers with dedicated time to hear from service providers, particularly those supporting someone with mental ill-health and to ensure their voices shape local mental health strategies.
On December 14th, a carer engagement peer event took place at Sydenham’s Ignition Brewery, creating a vibrant and inclusive space for unpaid carers in Lewisham to connect and share experiences. The event, which was carer-led, was hosted by Wendy, who is passionate about strengthening the network of support for carers in the borough. Wendy was joined by her son Jamie who as a young carer was awarded “Young Resident of the Year” in 2022 by Lewisham Homes.
The gathering named Sydenham’s Ignition Peer Support “SIPS FOR CARERS” provided an opportunity for carers to engage in meaningful conversations.
Welcome to a brief update of my Lewisham mental health carer forum aimed at those caring for someone living with mental illness.
The carer group discussed the importance of involving carers in the planning and improvement of services, with a focus on creating a carer family involvement network and improving carer information. They also addressed concerns about the lack of involvement of black carers in Council initiatives and the need for better communication and support for carers. The conversation ended with discussions on effective communication in caregiving for mental health, the importance of self-care for carers, and the need for professional help when communication breaks down.
Welcome to a brief update of my Lewisham mental health carer forum aimed at those caring for someone living with mental illness.
Forum update for October
Matthew Mckenzie led a meeting for mental health carers, introducing new members and discussing essential questions for service users’ care and treatment. The group explored various aspects of mental health care, including diagnosis, treatment plans, medication, legal rights, and the importance of carer involvement in the recovery process. The conversation ended with a presentation on the challenges faced by unpaid carers and a discussion on the importance of peer support and knowledge empowerment for carers navigating the mental health system.
Mental Health Carer Group Organizing
Matthew Mckenzie, who has lived experience of being a mental health carer was the group organizer. He led a meeting with various carers and professionals. Matthew introduced himself and his various groups, including one for South West London.
He also mentioned his carer website and the previous meeting’s link. Matthew then proceeded with introductions from various attendees who also are unpaid carers. Matthew then introduced Nadine, the new Lewisham Mental Health Carer’s social worker, who shared her role and responsibilities. The conversation ended with Matthew planning to present on what carers need to prepare for if they’re going to end up in a role with mental ill health.
Carer Support Worker’s Role and Plans
In the meeting, Nadine Denniss-Baker discussed her role as the new Lewisham carer’s support worker, emphasizing her commitment to understanding and addressing the needs of carers. She highlighted her involvement in various groups, including a carer’s group and carer’s champions meetings, and her plans to update and expand these initiatives. Nadine also shared her personal experiences as a carer and her professional background as an approved mental health professional. She discussed the importance of transparency and the need for better communication and collaboration between different organizations and groups. Also discussed was the potential for Nadine to attend national meetings and share best practices with other trusts. The conversation ended with a discussion on the importance of sharing good practice documents and resources to support carers and staff.
Introducing New Members and Questions
Matthew led a meeting where he introduced two new carer members group. Matthew then presented a list of essential questions for carers to ask regarding service users’ care and treatment, which he plans to blog about in the future. He also mentioned that he would record the meeting for those who couldn’t attend. The meeting was part of a carer’s forum, and Matthew emphasized the importance of carers being aware of these questions to better support their loved ones using mental health services.
Understanding Mental Health Diagnosis and Treatment
Matthew discussed the importance of understanding the diagnosis and treatment plan for a loved one’s mental health. He emphasized the need to ask about the current diagnosis, treatment plan, and the effectiveness of the treatment. Matthew also highlighted the importance of monitoring side effects and the potential for medication adjustments. He stressed the need for carers to engage with the multidisciplinary team, including primary contacts, and to inquire about the roles of specialists like occupational therapists. Matthew also mentioned the importance of understanding the medication’s purpose, dose, and potential side effects, and the need to clarify with the loved one if they can refuse medication. He concluded by emphasizing the importance of education regarding medication and mental health
Discussing Relapse and Care Plans
Matthew also highlighted the importance of asking about signs of relapse and what to do in emergencies, as these should be included in the care plan. Another member of the carer group, Faith mentioned a carer’s emergency card discussed at a recent forum, which Matthew agreed was a valuable tool. The group agreed on the need for a two-way conversation about relapse signs and for these to be recorded for quicker response times.
Carer Awareness, Training, and Rights
Matthew emphasized the importance of carer awareness and training, urging carers to ask questions and seek clarification when necessary. He also highlighted the need for carers to know their rights and how to make complaints if they’re not satisfied with the care provided. A carer suggested adding a section on how to make a complaint, which Matthew agreed to include in his future lectures. A carer stressed the importance of knowing the names of the care team and their managers to ensure effective communication and support. Matthew concluded by discussing the need for carers to understand what information can be shared with them, and the importance of obtaining consent from their loved ones to be involved in their care.
Involving Carers in Recovery Plans
Matthew discussed the importance of involving carers in the recovery plan of their loved ones, especially when they are living with them. He emphasized the need for a comprehensive care plan, which should be shared with the carer and the service user. Matthew also highlighted the importance of establishing specific goals for the service user’s mental health and social well-being. He suggested asking essential questions about the discharge plan, support after discharge, and the involvement of the community mental health team. Matthew also stressed the need for carers to understand the goals set for the service user’s recovery and to ask for practical advice on how to support their loved one. He concluded by mentioning the need for carers to know the roles and responsibilities of the care coordinator and other team members.
Challenges of Unpaid Carers in Borough
In the meeting, Matthew presented a detailed account of the challenges faced by unpaid carers in the borough, highlighting the what type of support and resources available to them. Carers discussed the need for better advertising and involvement of carers in services. A carer raised a question about encouraging carers to be more involved in services, to which Matthew responded that it’s a challenge due to the carers’ heavy workload. Matthew agreed to share his presentation in PDF format and to write a blog on the topic. Several carers expressed appreciation for Matthew’s presentation, noting that it provided a clear guide for navigating the complex network of resources and services.
Challenges of Carers and Peer Support
The carer group discussed the challenges faced by carers and the importance of peer support. A carer shared their experience of dealing with the mental health system, highlighting the lack of support and the invisibility of carers. Matthew emphasized the need for carers to be equipped with knowledge to ask specific questions during meetings to avoid being lost in the system. A carer asked another member about her experience of caring for her loved one regarding psychosis, and the carer responded by shared her journey, highlighting the importance of peer support and retaining hope. Matthew ended the conversation by encouraging the use of triangle of care and inviting everyone to attend future meetings.
Hello visitors and those providing care or caregiving to someone close. Here is another carer awareness blog from Matthew Mckenzie, carer activist, poet and author from Lewisham.
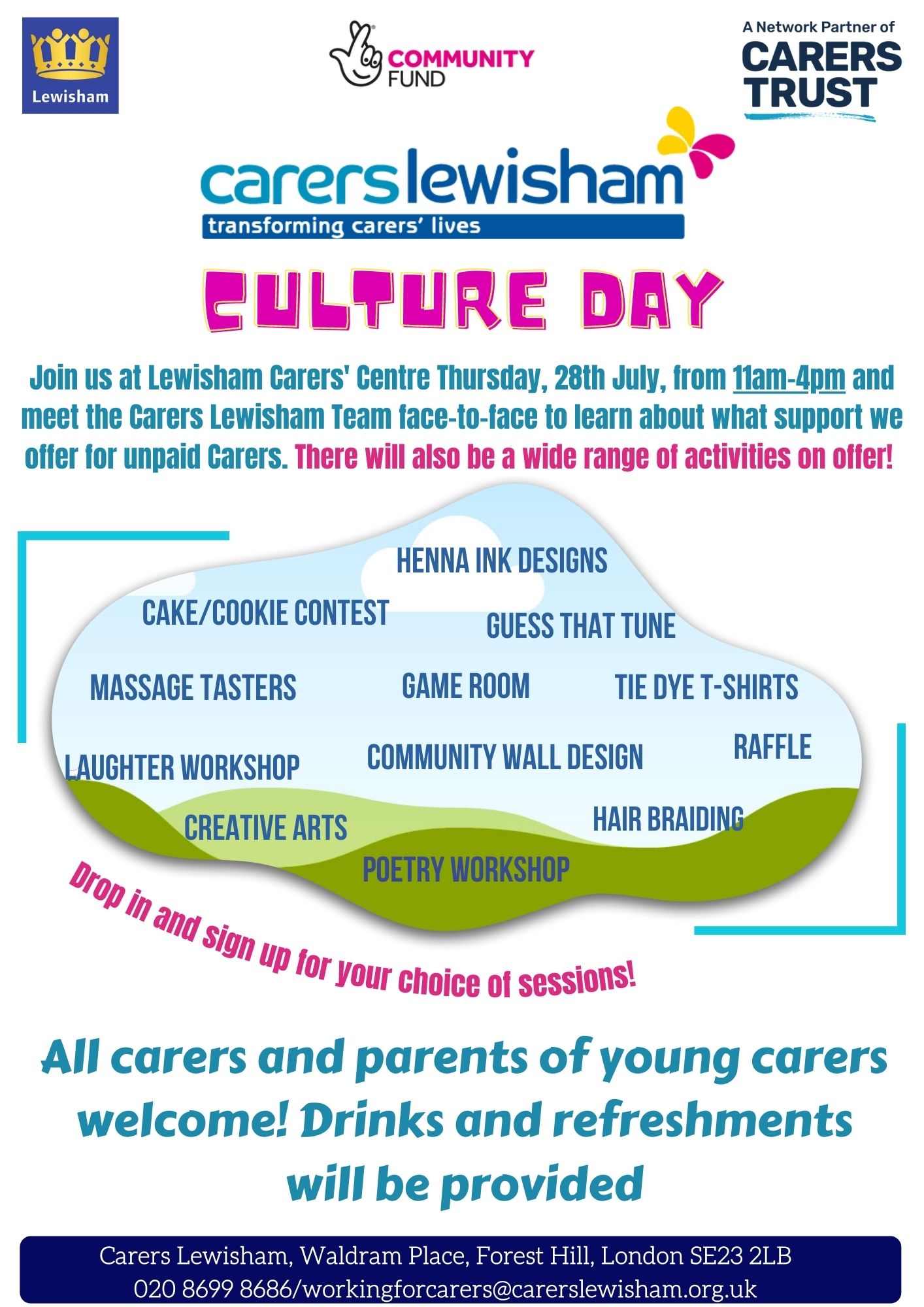
This blog is about Carers Lewisham Hub’s culture day. Carer centres are a vital part of providing support and services for those giving unpaid care. Carers Lewisham fights hard to identify carers, advocate for them and give as much support as possible.
I often visit the carers centre for their forums and support groups. On the 28th of July 2022, since the borough of Lewisham was the borough of culture. Carers Lewisham was hosting their culture day at their carers centre. A list of activities, networking and events was provided for carers who wanted to feel valued.
We had the game room and Raffle ticket event. Massage for those who have stress, aches and pains. Creative art sessions for those wanting to be……well creative. We also had laughter workshop, book readings and also my poetry reading (more on that later.)
I think most of all, carers who came along to the event wanted to network with others. They wanted to reduce isolation and link up with carers, staff and advocate to get support, information and to feel valued.
Since my poetry book “The Poetry book of mental health caring” was released in July 2022. Carers Lewisham was kind enough to offer me a poetry workshop. It is well known that over time, poetry can contribute to forms of culture. Most if not all my poems focus on the aspect of the caring experience. The poems look to raise the awareness of those providing mental health care. That means providing unpaid care to someone suffering mental illness.
At the book reading and poetry workshop, we had other carers reading from their poems which they have developed. Tess read a wonderful poem and also Brenda.
I ran my workshop by reading a poem and then asking others to also choose a poem to read. We then reflected on the meaning and definitions of those poems. You can see the video of my poetry workshop below.
Hello, everyone!! Merry Christmas thanks for joining me here today to explain a bit more about future projects that I’m going to be working on. Some of them actually, almost practically finished. So yep, my name. As you can see from the title here, my name is Matthew McKenzie, Carer campaigner, Mental health carer activist who facilitates several carer groups around half of London.
what I want to do is just explain a few things regarding some books that I’m working on. I’m going to start developing audiobooks, I will of course continue to work on paperbacks, one of them is in draft at the moment. I’ll talk about that in a bit.
If you want to see the video version of this blog, please watch below.
Special edition of my poetry Audio book – The Poetry book of mental health caring
So during summer 2022, I published my first poetry book. This was my first attempt at what I felt would be focusing on the experiences of providing mental health care. One of the reasons of doing poetry is that you don’t have to really read a whole book to just sort of reach out to those who perhaps understand, in a sense of what’s it like to provide care for someone with mental ill health. Plus to also reach out to those who’ve never experienced it.
So I’m doing an audiobook project on my poetry, but with the added benefit of contributions from other carers who are activists or are poets who want to produce poetry on the carers experiences. So I’m hoping to publish in early 2023, January, February, by that time, that audiobook will be coming out.
Race, caring and mental health
The next book, which is not an audio book, will be in paperback form. I felt it was due time to come out. This is because I have been writing books close to two years now. I have also been running as carer groups, but two of them focus on ethnic carers coming from ethnic minority background, so obviously, they are providing care and support to someone experiencing some form of mental illness.
I’ve been meaning to develop a book like this for some time looking at how mental illness can impact on the family, on friends, not from the patient side. Let’s look at this new book closely. The book titled “Race, Caring and Mental Health”. From it’s first chapter, I often say to many people that it’s important to tell your story. With this book, I felt it even more important due to some of the tragic consequences that can happen to ethnic minority groups providing unpaid care. This is it’s not just within the mental health system as the book’s second chapter will be looking at discrimination and racism, and links to mental health, for the other chapters, they will focus on health inequalities and the structures. The book will explore the deadly roundabout regarding the repeat situations of those going in and out of the mental health system. Why does this occur?
I don’t have the answers and can only share my ideas of what I’ve seen and what I’ve heard, but I know what I’m learning about. I’d be really interested on people’s views of my new book, which is in draft form at the moment and I will probably change a couple of pages in the hope to release this around January 2023.
Providng Care and other Short Stories
Lastly my 6th piece of work will be an audiobook, similar to the project of the poetry audiobook. But this time I want to work towards fiction. Now, I’ve been writing two years now. Most of the books that I’ve been doing are not fiction at all. I mean, I suppose you could argue in some sense that poetry is looking at certain topics that may or may not happen. So this new audiobook will be my first attempt at fiction, including 20 short stories about unpaid care, here are some of the stories below.
This audio book will explore some of the following carer themes.
Providing Care Story about a woman finding out her husband has developed a form of mental illness, she now has to battle to become an unpaid carer.
Digging out of a hole A young man caring for his sister, but this time there are horrible things that make his life difficult.
A family Affair Story of a main carer feeling isolated by the family, everything is thrown at her and no one wants to help.
Never thought it would be me A female carer whose partner is caught in a serious accident, her life is turned upside down as she battles to provide care for him.
Angry A carer thrown into anger and despair as she is let down time and time again, leading her to becoming angry.
Just when I needed you A story of carer peer support and why it is needed, a story that is more hopeful than previous stories.
Anyway, thanks for stopping by. Hope you have a lovely holiday break.
Hello fellow mental health carers and readers, been a while since I have been blogging due to working on my new book called “Race, caring and mental health”. This book will be my 2nd release for 2022, the book will reflect how mental illness impacts on carers from ethnic minorities especially black people. I hope to get that book out for November 2022.
Going away from promoting my new book, this is just a quick blog for my Lewisham mental health carers forum. A forum aimed at those caring for someone suffering mental illness.
The speakers for October 2022
Marie Cooper RGN BSc MSc (Florence Nightingale Foundation) – Pallative care “walking the walk” Evelyn Sample (South London & Maudsley NHS Trust) – Approved Mental Health Professional / Mental Health Act presentation
Marie Cooper presents on Palliative and End of Life Care
Marie Cooper who is also the Project Lead for Palliative Care Nursing at St Christopher’s wanted to understand the experience of the carer when its come them supporting a loved one coming to the end of their life. Marie mentioned when it reaches that stage, the term for that person becomes more personal as they see themselves more than just carer. They are perhaps a family member, a loved one, anybody of importance to that person.
Marie mentioned it is really important to hear the voice of the relative or person experiencing their loved ones end of life care. Marie started off by showing a few pictures of hospital rooms.
In her talk it was stated that in hospitals, where someone was visiting a loved one or someone who had died. The experience of walking through the hospital or the bereavement suite makes a big difference in someone life, this will stay with them forever. So the project Marie mentioned was “Walking the walk” as Marie and her colleagues would become the carer as they walk through the wards. They travel right through the hospital into understand the entrance, the experience of what that family might be going through as they visit a loved one who has died. Marie focuses on emotions of that time, some people are rushing to get to where their loved ones are, or the people being there for days waiting and attending to their loved one and what support is there for them.
The overall aim of the project is to improve the experience for the family and the friends, anybody. What they did was they worked with 25 hospitals, those being 25 acute trusts over the past and pre COVID period. They have just done the Evelina hospital for Children with parents, which has been a very powerful experience. That hospital is formed from Guys and St Thomas NHS FT.
As mentioned in her talk, Marie literally walks through the hospital, they do the walking, and this would be a team of four of them. They would visit all the public sites, look at the toilets, look at the phones, look at the cafeteria. They would take photographs and eventually they report back to the hospital to get feedback on improvements. In the end it just gives them a chance to speak to the nurses, the doctors on what their experience of people coming to the hospital in their last days? What’s working well, what would they like to see different.
Marie and her work partners look at four areas, they look at the environment to practical facilities, is it clean? Is it comfortable? Is it hostile? Is it something that they would want to sit in which is accessible? They also talk to families to get their experience e.g. caring for my loved one for many years? Can they still care for them? How much can they be involved in the care of their loved one? Then thirdly, what support is there for that person? Have they got Wi Fi access at that hospital site? Can they get access to food? Can they park? Can they shower? Can somebody be their key person? tell them what’s going on so they can support their loved one? Plus what about the care after death? What care is there for the person after that loved ones dying. So they look at all those four elements as they traveled through the hospitals.
Marie should has a picture slide of waiting rooms at a children’s hospital. The experiences when children die, the memories and all the incredible work in children’s hospitals and hospices around trying to contain those lost memories, and about how to show a child are still being cared for after their passing, through the use of fabrics and cots and other furniture. So that in keeping the personhood of that deceased person relevant and respected that the family might be find helpful and comforting in future.
QUESTIONS FROM CARER MEMBERS
Is there capacity for cultural improvement for the experience of pallative care regarding ethnic minority carers.
Do You get any push back from Chaplin services as hospitals?
I run a carer stall at several hospitals, What can you say to someone who’s going through a difficult time when their loved one has died or is dying?
How can mental health trusts take on the programme? People do not die as in a planned state, but pallative care is a concern due to sudden death or complications from mental and physical health.
One person mentioned that their are two end of life care situations that comes around in different ways. For some people it’s planned that they’re goning to die. Often in certainly adult mental health services, we don’t always know when people are going to die. It is usually quite traumatic and when they do die, either through suicide or premature death, because they’re physically unwell, we are not sure if we have a sort of clear cut response. Often, there’s lots of practical things that we might help families after, but from the presentation there are a lot of things to query.
It was raised that the way carers centers respond to end of life, is that they would not normally stop someone’s membership when they cease to become a carer. Because they know that that’s a really difficult time, and they’re going to need help, sometimes they might keep them for like 18 months after to help them, especially if their caring role has been their full time job and their identity, they would help them sort of replace it with other things, volunteering, getting back to work, that sort of thing. It would be bad pratice to tick a carer off membership if their loved one passed away, but then it is also a decision for the carer.
Are pallative care policies updated at mental health trusts compared to accute trusts?
One person responded I don’t think or I’m not aware that we do have a brief new policy, we have a certain minimum as unfortunately and tragically, a very high disproportion of our service users die prematurely. The experience and impact of death has a huge strain and trauma on the carers health.
As in the past there are a number of our service users who commit suicide and when there is an incident then there is an investigation process that goes into reviewing the care that was provided to that individual.
Evelyn Sample presents on the mental health act
Evelyn looked into the role of the nearest relative under the Mental Health Act and how it’s changing in the coming years. She is aware for a lot of carers that the Mental Health Act and the functions of the nearest relative are quite confusing. So she thought that she would talk to us about what the nearest relative rules are and why some people are nominated as the nearest relative. Plus how and what are the rights and responsibilities of the nearest relative and how that might be changing.
Evelyn reminded us that she is a mental health social worker, which means she is an “Approved Mental Health Professional (AMHP)”. Now the approved mental health professional historically has been as A role that was exclusively for social workers. Since 2008, it has been possible for non social workers, nurses, occupational therapists, psychologists to have that role.
Evelyn feels what is really important is that people have information about the role of the nearest relative, because what happens as an AMHP is that you are assessing someone under the Mental Health Act, either you’re planning an assessment that’s going to take place in the community or you’ve been asked to assess someone who’s already an inpatient in the mental ward. This could be because they have come in as an informal inpatient, and they are now having a mental health assessment on the ward.
The function of the nearest relative is to provide a safeguard under the mental health act. So in order to ensure that people have person/patient interests and also they have the person’s well-being considered. The nearest relative has an important role other than the doctors who are involved in making recommendations for detention, or the amp who is employed by the local authority to also act as a safeguard.
The idea is that the nearest relative is intended to be the person who is thought to be closest to the patient, and who therefore knows them best, and is able to, to act in their best interest.
When the Mental Health Act was originally devised in the early 80s (1983), the current Mental Health Act, used as a sort of table for identifying new relatives. That table now seems quite outdated so therefore there was a proposal to change the act so that people can actually choose the nearest relative. Evelyn mentioned they have a system where the nearest relative ( Section 26 of the act). says if you are the husband or wife or civil partner of a person, then generally you will be the nearest relative. Then the table goes on from there.
Husband, wife or civil partner Son or daughter Father or mother Brother or sister Grandparent Grandchild Uncle or aunt Nephew or niece
The issue is that it is a rigid order that is set out in the law that determines who is the nearest relative? And currently, the amp and the patient have little to no say over that.
The proposal is that under the Under the new Mental Health Act that’s coming in; Mental Health patients in advance of mental health assessments, when they have “capacity” to do so will be able to nominate their OWN nearest relative and choose the person that they think will best reflect their their wishes, and will act in their interests.
So this change is going to be significant in the legal situation, assuming that the The bill has not yet gone through Parliament, which is about increasing the patient’s choice, and enabling patients to be more involved in the decisions around there care and treatment.
QUESTIONS AND STATEMENTS FROM MEMBERS
Sometimes the nearest relative is usually the carer or friend. So when it comes to the nearest relative, could it not be changed to “The nearest relative or carer?”. Because sometimes the nearest relative might be 100 miles away.
Can the nearest relative refuse because of bad history with their parents, whether they’d been abused and they just they just basically have cut links can they refuse if they were contacted?
Do you have any like sort of queries or concerns regarding the new changes to the mental health act? and the second question on is there like a list somewhere on like the duties an AMHP that could be tailored to how they deal with unpaid carers?
Welcome to an update from my unpaid carers blog. Recently I attended Lewisham Carers Hub event. They are relaunching their carers forum, which is a great way for unpaid carers to connect, network and voice their feedback.
Lewisham Carers Hub provides a range of services including advice, information, emotional support, short breaks, opportunities to meet other carers to reduce isolation and build resilience.
The event was chaired by Sue Stockman – Director of carers services. Sue listened to carers carefully and responded very well to queries and concerns. With the relaunch of the carers forum, Carers Hub Lewisham wants to be more inclusive and give carers a chance to co-chair the meeting.
I was excited to hear about work to promote a carer’s charter developed in conjunction with unpaid carers. A carer’s charter helps carers and others know about carers rights. I also learned about IT development support for carers struggling with digital literacy and upcoming services at the carers centre including carers counselling service, health and wellbeing activities and cost of living workshops.
At the forum was Tristan Brice from Lewisham council. Lewisham council wants carers to feed back on recommissioning and also wants to hear from carers about carer identification, carer assessments and other things.
Lewisham Carers Hub are also going through a rebranding process and I have included part of the branding below. There will be more to come.
In the end I thought that well attended with many carers contributing their thoughts and suggestions. I feel having a carers forum shows how a carers centre can give carers a voice and a say on what helps them overall. So even though it is early days, we can see how the carers forum develops.
Welcome to a brief november 2021 update for my Lewisham mental health carers forum. The forum is an online forum and provides engagement for those caring for someone suffering mental illness. The speakers for November 2021
Li-ying Huang – South London & maudsley Pharmacist Raymond McGrath – Lead Nurse : Integrating our Mental and Physical Healthcare Systems (IMPHS) for Mind & Body Programme
Li-Ying Haung presents on the importance of medication.
As we all known medication and mental health can go hand in hand, there are times when patients struggle with medication and unpaid families and carers feel there is a lack of information and engagement regarding medication.
Welcome to the September update of my Lewisham mental health carer forum 2021. As a note, the carer’s forum is an engagement group aimed at those caring for someone who suffer’s mental ill health.
Since the carer’s forum focuses on carer’s from Lewisham, we tend to get engagement from mental health services of South London & Maudsley NHS foundation trust. I am grateful for the support our local NHS trust gives to families and carers. It is important that families, friends and carers remain that strong link in coping and recovery.
The speaker’s for September were
Leonie Down – Lewisham Head of Occupational Therapy and Partnerships Lead from South London & Maudsley
Ros King – Regional carer lead for London from NHS England
Charles Malcolm-Smith – People & Provider Development Lead from NHS South East London CCG (Lewisham)
Leonie Down presents on the importance of Occupational Therapy
As mentioned earlier, South London & maudsley prides itself on the engagement and involvement of those who use it’s services and those who care for patients. It was great to have Leonie engage with our carer group on the importance of Occupational therapy.
Leonie stated her talk on how occuptional therapy can help people manage their routines at home, and also occuptional therapy helps look at the physical health component and ways for people to adapt to disability. Leonie presented an example from The World Federation of occupational therapists (WFOT).
“Occupational therapy is a client-centred health profession concerned with promoting health and well being through occupation. The primary goal of occupational therapy is to enable people to participate in the activities of everyday life. Occupational therapists achieve this outcome by working with people and communities to enhance their ability to engage in the occupations they want to, need to, or are expected to do, or by modifying the occupation or the environment to better support their occupational engagement” (WFOT 2012)
Leonie admitted the defination was a bit wordy, but it does encompass the fact that it’s about activity and occupation and that’s the medium through which Maudsley NHS deliver their interventions.
Leonie has worked as an OT for around 30 years, a lot of people ask her, what’s an OT do? So she often responds that it’s about supporting people to do the things that makes them feel better. So it’s very much about what people spend their time doing, what people feel, what activities that make people feel feel better, make them stronger in themselves, plus setting their direction towards recovery. As an OT, it’s a degree that they have three years in training as an occupational therapist, which ultimately equips them to be able to understand the needs of each individual. These could be what strength and barriers might be around the person or being able to access activities that make me feel better, and that could be multifaceted.
Leonie then presented on the following, where how can service users benefit from OT. The following points were explained.
How OT promotes self-expression, creativity and the development of hobbie
Where OT can improve / develop
feelings of self-esteem and confidence
level of self-awareness, understanding and insight
ability to manage health conditions and ADLs
social interaction and communication skills
coping strategies and self-management techniques
How OT supports the development of roles, responsibilities and routine, as well as identifying and working towards goals
Promotes healthier lifestyle choices and greater levels of physical activity
Increases the chances of an earlier discharge and the likelihood of them being able to remain safe and independent in the community
Improves the patient experience and wellbeing.
Leonie then moved on to present the work being done in Lewisham regarding OT, where they are trying to work with as many social inclusion partners as possible. So one half is Lewisham community connections, where people are helping those using the services navigate through to something that they can be doing to help their health.
The other aspect of OT in Lewisham, is very much about trying to co-produce and co-deliver a program of groups. Which is for people that that may benefit from the environment that involves other people. This is because other people, from the same environment can learn or hear different insights, which can lead us to start making sense of our own experiences and possibly develop tools to become self reliant.
There was then a Q&A session from carer members of the Lewisham MH carer forum.
Ros King from NHS England speaks about ICS changes
Ros King kindly engages with my carer groups when she can, so today she was invited to speak about the important of Integrated Care Systems. Ros started explaining about NHS England and how it is a huge organization and can be very complicated. Ros mentioned how NHS England is basically the body that sets health policy with the department of health and social care. Such policy helps plan for what the health service will be focusing on where It also holds allocated budgets. The budgets are then allocated down to CCGs where Ros explained that there has been quite a few changes.
It was explained that a couple of years ago, the responsibility was around Clinical Commissioning Groups, and NHS improvement was concerned with providers, so acute trusts and some changes were implemented which led to a merger to become NHS England & Improvement.
Ros then explained a bit about The national teams and the regional teams. Where there are seven regions across England. As in other countries just NHS England we have Wales, Scotland, Northern Ireland, which have different arrangements.
Ros talked about the London region and what sits within the London region, where there are five integrated care systems. These being Southwest London, southeast London, North Central London, northeast London and northwest London. Ros joked that she really hopes nobody has any questions around which CCGs sit within such ICS because that would take some time. Ros talked about how the CCGs have merged to cover such regions around London.
Ros moved on to talk about how NHS England & Improvement would demand lots of information, especially very complicated information about how the CCGs and providing trusts were performing in all sorts of areas. Such requests for information could be at a very short notice because those at NHS England & Improvement have to feed this info back to the organisation.
Ros felt there has been a lot of changes as to whilst regions do still have accountability, So if an acute provider in Lewisham, has really serious concerns and risks about performance of the quality of the services they’re providing, then it is still very much NHS England regional team responsibility to manage and try and work with the provider to improve.
The idea is rather than an acute provider struggling with performancing issues, they should learn from other providers and network together. Still, NHS England has commissioned a lot of things, but now only comission small amount of services which are specialist services. These will be transferred out into ICS.
Ros then talked about how they manage complaints around a primary care service. So GPS, dentist, ophthalmologists, pharmacists and so on. Such complaints would come in to NHS England depending on the complaint e.g. if you have a complaint about any of those services, it would come through to NHS England, or if you had a complaint about a service that was commissioned by your ICS, or your CCG, that would go into the CCG or directly to the organization that’s providing the service.
Charles Malcolm-Smith presents on ICS at a local level.
I had a lot of support from engagement representatives of NHS South East London CCG where Greenwich, Southwark and Lewisham CCGs had organised what to present to carers and also who can support Ros Spink’s presentation.
In the end Charles who is the people & Provider Development Lead from NHS South East London CCG (Lewisham) continued the presentation.
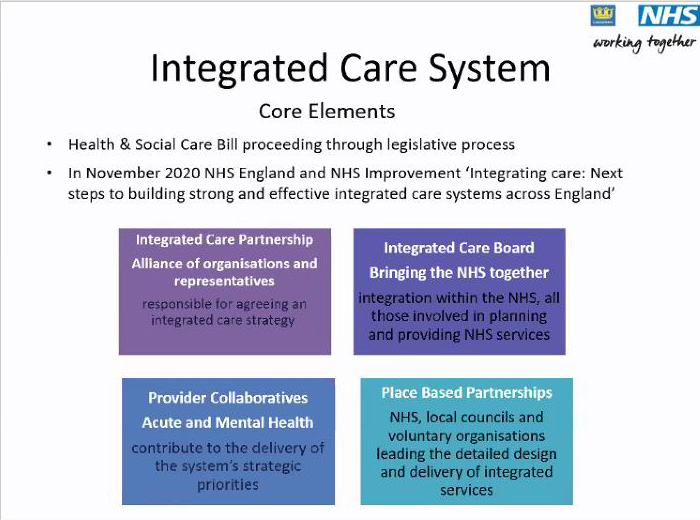
Charles talked about what integrated care system changes that are in the pipeline and how they are designed to work together better. With all the talk about health and social care needing to work better with physical and mental health services, community acute services and primary care, it’s all about the different parts of the system working together and this is about structural change.
It was explained that we have had integrated care systems for a while, but their status had changed from the sustainability and transformation partnerships, where they became ICS even though it is still a partnership status, with the health and social care bill now making ICS statutory organisations. Charles explained that there will be four building blocks to do an ICS. So the ICS for southeast London will have an integrated care partnership board and this is the alliance of organizations that represent across southeast London. These will include the NHS organisations, local authorities and made up of the chairs of the trust.
Elected representatives and elected leadership from each of the local authorities as well as the representative director from Adult Social Care, children, young people services, Healthwatch and voluntary and community sector organizations. Charles reassured us that in southeast London, there aren’t any private sector organizations involved in the partnership since there were a lot of questions from members about privatisation creeping in.
Charles talked about how the Integrated Care board brings the NHS together so it brings commissioners and providers around the table. Charles mentioned it was an important development because the last couple of decades, it has always been a commissioner and provider that were split causing queries with contracts. although there will still be commissioning and providing but the approach to it will be about joint planning. So there will be working together more closely than before.
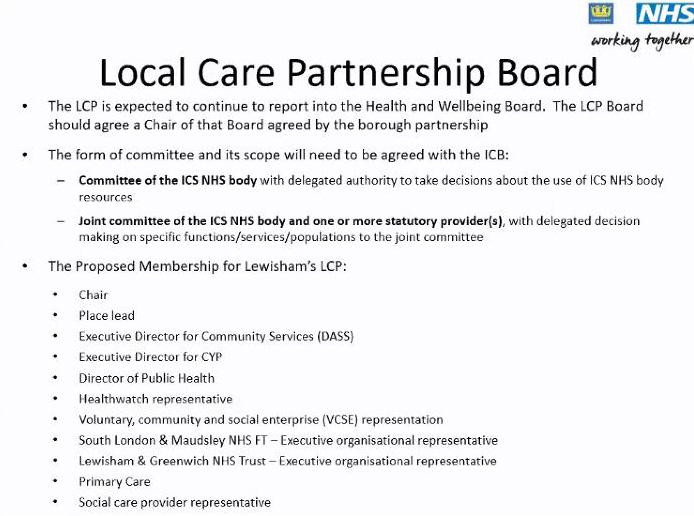
There were many questions from carer members on if the Local Care Partnership board will debate the importance of unpaid carers and include them in their decisions.
This concludes the brief update of my Lewisham mental health carer forum for September