Here is the update for the February Lewisham Mental Health Carer forum. The forum is aimed at those who care for someone with a mental illness. Most who attend are unpaid family carers. For this forum we were joined by the CQC inspector for GP surguries and Professor Luke Clements from Leeds University who is an expert on carer’s rights.
As for the members of the forum, carer members were from South West London, Lewisham and Greenwich where I often host other carer forums or support groups. We were even joined by West London NHS trust staff who were interested in how a carer led forum runs, plus also SLaM early intevention staff.
The CQC inspector engages with carer members
Susan George the inspector from the Care Quality Commission mentioned that a few months ago I kindly invited some inspectors from the Care Quality Commission to join the BAME carer forum. Originally, I invited inspectors from the CQC’s hospitals Directorate, and also the Adult Social Care Directorate, howvever Susan is from the PMS primary medical services Directorate who inspects GP surguries. Susan is very interested in health inequalities and while she is an inspector, she did mention it has been a challenge doing inspections. She feels that they haven’t been able to listen to people, listen to patients and listen to people who are carers who use GP services for a while now. Its obviously because of the pandemic, it’s become more difficult for people to access services and also to express their experiences.

One carer member was concerned about how the GP surgery contacted the person she cared for about the COVID vaccine. The person she cared for received a text message for the vaccine. However she felt he should have also get a phone call. So in the end she phoned the GP surgery and they said, “Oh, he should have received the text message anyway”. In the end the carer had to check and make an appointment for him. She was wondering if service users who are slightly unwell get the mobile message, how do carers get involved if the patient does not respond?
The CQC inspector responded that their involvement in terms of the vaccination hubs and clinics, are through the contracts or agreements for those are with the primary care networks “PCNs” and the CCGs commissioners. So the CQC don’t regulate that side of things. But what the CQC do look at and regulate is patient safety and infection control. So for example, if a patient said that, there was too many people in clinic that people were queuing and it was unsafe, or that there wasn’t any hand gel then that’s where the CQC could intervene directly. So the way that GPS are running their hubs is for the PCs and the CCGs. To organize and arrange. Since the CQC don’t have responsibility in that area. The other area which the CQC would be interested in, is how carers are able to access services. So if there was negative feedback about such experiences, it’s something that CQC could feed back to the practice.
Another carer member asked about an issue regarding a symptom and they had to send a photograph to the GP to look at the area. They came back with recommending some kind of a cream, which was absolutely the wrong kind of diagnosis, The carer felt that they don’t think being able to diagnose or a photograph is sufficient when you are dealing with something like that. So the carer wascurious as to how to overcome such things, whether it be a video call or some other means of being seen
in a more realistic kind of setting to deal with those kinds of issues.

The CQC inspector responded by stating that as inspectors they are not able to comment on individual prescriptions or treatments because that’s confidential, it’s between patient and their GP although she does know that it’s a huge change the move to online only consultations.
Susan mentioned that there is difficulty for some people to take photos upload them from the doctor and her advice is always to be vocal and complain or raise the issue directly with the practice. They have to respond within 48 hours and they have to start a process of investigation. So if there is some aspect of your care that you weren’t happy with, please contact the practice, feed it back to them because they are obligated to respond and investigate the issue.
Another carer member mentioned about booking an appointment with a GP, they felt the experience needs to improve. They felt if they was to get the person they looked after to go on a phone to book an appointment, they would never get one, which is frustrating. Especially the wait times so the carer thinks there needs to be a better way of people engaging with their GP.

The carer member also mentioned that we do need to ensure that vulnerable people and people who are carers who are also patients of GP surgeries, or having their needs met, need equitable access to services. She felt that she thinks the pandemic has thrown up a lot of shortfalls in that area.
The CQC inspector felt that members should try be active and make sure to complain, if you’re not happy with something, e.g. being your treatment or care, please get in touch with the practice, and complain or give them feedback so in the end they are demonstrating that they’re responding to patient feedback and that is something the CQC look at as inspectors.
There was a great discussion about how receptionists or GP surgery admin needed to be trained adequatly on dealing with patients and carers, perhaps some sort of GP wide training curricum.
Professor Luke Clements Presents on carer rights
Prof Luke stated off explaining that as a lawyer he has been a solicitor for a very long time, but really most of his life now has been as an academic, he runs a research unit, which is funded by a charity, focusing more on disabled children and adults. He does write widely about disabled people and carers rights in particular, and he plans to go through some of this at the forum. Prof Luke mentioned he also was the Special Advisor to the joint parliamentary committee scrutinizing the Care Act.
Prof Luke Clements stated that for the carer forum he will respond to the question of who monitors the Care Act and discussing what carers can do to empower themselves regarding carers rights and their dealing with the council or the NHS. Luke pointed out his website for members to have a look at after the lecture
http://www.lukeclements.co.uk/
Luke stated that if you go to that site, you’ll see free to access some stuff. It’s just because he gets a lot of inquiries, so he tends to try and put stuff up on his site. So there’s a lot of stuff on the Resources tab about how you can challenge local authority or NHS decisions. On the right hand side there is a template that you can use and on the left hand side, there’s the just the general index. Plus lower down the website you’ll see information on challenging reductions in care packages.
There was more explanations on his website being that publication’s tab, there are all the books that are written most of them are freely available. People can get a book on carers and their rights, which is only a couple of years old. It’s the seventh edition. The book has got a chapter on mental health and it’s got a chapter on issues about 100 pages long, which you can download for free. If you click on that section of the website then book loads, and you can access that book and other books that are useful. Professor Luke warned another book isn’t the book that you want to buy since It’s a big book and it’s over 1000 pages long. However it’s the sort of in a leading book on Social Care Law it’s got everything, and it’s got far more than you ever need to know. But it’s useful to get a footnote or something like that.
He also has toolkit that was produce with the charity that funds him and it is a really useful document, which carer forum members can download that free from their website. Although it’s focusing largely on parents of disabled children, it’s just as relevant for carers of adults. It’s only about 35 pages long, but it’s got precedent letters at the back, it divides problems into different ways.
Professor Luke mentioned that he also has a new book he has just written, which isn’t free, and It’s a little expensive, but it’s about families. The people he tends to work with don’t have one set of problems. They don’t they’re not like the standard people lawyers deal with, e.g. such people do not want to divorce or buy a house, they dont have that single issue. The people that he has spent 40 years acting for, as a lawyer don’t have that one problem, they have a whole cluster of problems. So their life in a way, because they have these clusters or multiple problems. They live and bump into the law all the time and so it’s a sort of critique of the way the system operates, but it is also a critique of the way that public bodies operate as in the NHS and social services.
Professor Luke continued to mention that if you click on lecture series, then there is also a lot of YouTube stuff. Plus there is a much longer talk about carers and their rights. There’s also talk on carers and identity, which was done recently about the failure of equality legislation to deal with carers. There’s is also a talk he did a while back, but it’s just as relevant today on carers and human rights, because due to time he was not going to do anything more than touch on that subject today.
Prof Luke feels that the NHS actually has very few direct legal duties, while the social services have stacks and stacks of duties towards carers, but what all the evidence is showing is that’s its not really translating into practical benefits straight off. Although, in theory, carers have a lot of rights, but in practice that hasn’t really worked out. He thinks that’s an issue about access and thats an issue about being empowered, being supported, being assertive, and often having to complain. Carers can complain nicely in the toolkit, as in that toolkit they have a sort of touchy feely complaint process, but it is often having to put your foot down and to do that Prof Luke thinks you need support from the sort of support groups that we are involved in.
Research has showed that “Carer support groups” and particularly “emotional support” is just as much as the single most useful thing that families with caring responsibilities need. So the law says there’s a duty under Section 10 of the carers act to assess carers.
There’s a duty to meet the needs of this carers. If a carer sort of says that the way an assessment should go is that the carer would have an assessment and that would say, look, I need a break, I need to have time on my own, I need to have time to go back to work, I need time to go to college, I need time to have a leisure or all of those things. The law says carers have a right to do to work to do education, training leisure.
Of course, in practice, it’s very difficult to get that but the carer can say “look, I need to do that!” and then the local authority would say “well, you need a break, then you need some time to do that”. So they then assess the disabled person with the additional support that the disabled person will need so that the carer can have a break. Often that’s been called short breaks or respite care, but it’s basically providing a decent package to the disabled person, so the carer can resume an ordinary life. So a carers assessment might identify a need, which is for break, but the services tend to be given to the disabled person, because that’s the person that has to be supported. So the carer can have that break. So the duty to meet eligible needs would be off to the duty to provide care.
Prof Luke joked that even though he is from Leeds University, you don’t need to go all the way up to Leeds, you could actually go to one of your local universities and do a part time PhD on what is care. This is because care isn’t just physical and practical care. Clearly, it seems to be that some of the most exhausting care is actually emotional care, supporting people. The Care act accepts that that you may not need to be physically or practically caring but but the mere fact that you’re anxious and stress waiting for actively seeking to prevent the next crisis that’s caring, and that’s one of the most exhausting things you can do as a carer. So caring can be done at a distance as we’ve seen during the Coronavirus. A lot of people are caring and are anxious and supporting people in care homes. That’s the care that takes its toll that qualifies you for your carer’s assessment at the very least!!
The key thing about caring in this country is that there is no duty on carers to provide care because that was abolished on the fifth of July 1948. Luke mentioned that we are one of the few countries in the world where there is no legal duty on a family member to care for another family.
So the act, quite rightly says that whenever there’s any assessment whatsoever, and that’s a hospital discharge, or just an ordinary and social care assessment. So whoever’s doing the assessing mustn’t assume the carer is willing or able to provide a continued care they simply don’t have to do. Prof Luke thinks it’s still culturally very difficult for a family member to say I don’t want to care for my mother, my son, my brother, or whatever and he thinks that the better approach often is to say, Look, I’m just physically and emotionally not able to provide care unless you give me some a break or some support. So you know, maybe I’m willing, but I’m physically not able to do this emotionally.
The law says that whenever an assessor is assessing for care, then the assessor must consider the impact on well-being, which is what the carer wants to do with their daily life. And it specifically says that includes education, training, leisure and work. So carers shouldn’t have to go part time or give up work or make all those arrangements. They can just carry on because they don’t have to provide care. Or all too often care is provided because the response of the local authority is inadequate, and carers don’t want to leave the person for whom they care in a difficult situation.
When you get a care plan and normally that would be for a disabled person. What the Ombudsman is saying quite a lot at the moment is that care plan wouldn’t only say this support will come in on this day with people with these set of skills, doing these particular tasks and these arrangements being made, but it will also include a plan B, because inevitably, the best laid plans just don’t work. So there is a problem and then the local authorities say, well, that’s unforeseeable and of course, that’s not unforeseeable, it’s predictable. So in the end what’s going to happen when the unpaid carer that doesn’t turn up or when the care system doesn’t work out, or when the the carer center is closed?
The thing is as Prof Luke mentioned, the care plan has got to be carefully mapped. You can’t say, Look, I’m sorry, we’re short of money, we’re gonna have to cut the care package for this person, or would have to reduce the rate, the needs that have been identified must be met. And if that costs 3000 pounds a week, then it costs 3000 pounds a week, money is only relevant when there’s two ways of meeting a need. If the needs are met adequately, then the local authority can choose the less expensive and but just can’t set arbitrary limits.
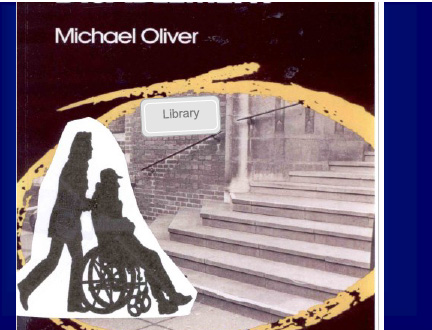
Prof Luke then looked to explan human rights and carers, which are not a protected category under the Equalities Act. So the Equality Act protects people on grounds of race and sex and age and religion, sexual orientation, and so on. But it doesn’t protect “CARE” as people who provide care. The Equality Act adopts the sort of social model of disability and the idea that says that people are not handicapped by their impairment, if they can’t walk, for instance, their problem is not that they can’t walk. It’s the problem that they can’t access certain support services, because of the way that we have created society. A good example was shown to the forum in the classic image of that is on the front page of Michael Oliver’s, seminal book, where you have a disabled person struggling to get up the stairs in a wheelchair, and he can’t vote. But he can’t vote not because he’s a disabled person who can’t use his legs. He can’t vote, because some idiot but the poling station at the top of a flight of stairs. So its the society that is what is handicapping him.
He’s unable to do these things because of physical barriers, not because of anything to do with him. They don’t always have to be physical barriers, they can be attitudinal barriers that you can’t do this because you’re a disabled person. Or they can be sort of administrative boundaries that you have to fill out forms and things like that. If you have intellectual impairments, you can’t do those sort of things or even visual impairments. So the Equality Act protects disabled people from adverse discrimination.
It doesn’t protect carers, however the social model does work or carers. So if you had a carer who was lets say, taking somebody and the carer wanted to vote, well, they probably could leave the disabled person at the bottom of the stairs, run up, vote and come back, and that would be okay. But what happens if the carer had to go for a longer medical arrangement like a CT scan, or radiology or if they had to perhaps spend an afternoon in the library, then they would be handicapped by their caring responsibilities, because they would have to make quite a lot of arrangements in advance to ensure that the disabled person was cared for whilst they did that longer term activity, so in that way carers are suffering because of their caring responsibilities.
So you could get a situation like if you want to see your GP, and you’d have to make an appointment today. You’d have to make an appointment on the morning. Well, that’s an arrangement that is probably okay for most people, except it’s not okay for carers because they’ve got to actually do all the mechanistic mechanics of arranging for substitute care for the the person that they care for. So that would be a process that adversely discriminates against carers. Its more difficult if the ‘cared for’ is mentally struggling and the system refuses to support the person doing the caring because it is deemed the ‘cared for’ is not in immediate risk. It is almost like a balancing act where anything could go wrong.
Now over 10 years ago, the was a key case of the European Court of Justice call the common or average law, and they held that treating a carer adversely, because of their caring responsibilities because of disability. This was a case where a woman was sacked Sharon Coleman, because she had to take on unexpected leave, or she had to take time off work because of emergencies to do with her son, who was disabled. The European Court of Justice said that she was being treated adversely because of the disability wasn’t her disability, but because of a disability she was being treated adversely. So a GPs appointment system that said everybody has to make an appointment on the morning is treating a carer adversely, because they are like everybody else, they have caring responsibilities. So there’s a limited amount of scope for using discrimination legislation in the equality act, to a degree section 13 of the Equality Act. But it’s been very little used. Prof Luke has written about that in his new book and the reality Luke pointed out is you’re not seeing lots of carers running off to employment tribunals.
In the end Prof Luke has been arguing that discrimination doesn’t really help carers very much, but it’s there to it’s to be that they have limited protection. There should be a lot more discussion, but there is academic discussion on what should be clearer to human rights. Professor Luke pointed out that there is a lecture on this, which people can download, if you really haven’t got anything better to do with your time where he actually talked more about this. Prof Luke has also written about this extensively. He thinks it’s quite extraordinary that we have lots and lots of cases about the right to express yourself or the right to do this and the right to do that. but there’s no more important activity for humankind then “CARING”. If we didn’t have caring, then we would die within hours of being born. So caring is the most fundamental human rights. We all have to be cared for and it must therefore be that there must be a “protected right”, surely for caring. Protecting the right to care is more important than protecting the right to anything else.
And yet, there’s nothing in any human rights treaty to have the right to care. There’s the right to private life, the right to family life, the right to express yourself, the right to religion and Association.
However there’s no question that caring is a HUMAN RIGHT and it would fall within what we call article eight, the right to private and family life. There is hardly any cases on this again, in the paper. Prof Luke mentioned he has just written in his book where he talks about this.
Some from the UN mentioned that it’s hard to think of the human rights that is not potentially affected in some way by the unequal distribution and difficulty of unpaid work. The failure of the states to adequately provide funds, support and regular care contradicts their human rights obligations and really what she’s doing there and really, of course, is its the issue with caring is the caring is gendered, because women do most of the caring then caring is looked upon as low skilled, which in itself is a discrimination.