Living with Parkinson’s disease is undeniably challenging, not just for those diagnosed but also for those who support them. During a recent panel discussion from Parkinsons UK, experience of care experts including Matthew McKenzie and volunteers shared their insights and experiences on managing these challenges, offering valuable advice for fellow caregivers. The discussion highlighted key aspects of being on the supporters journey, from communicating diagnoses to seeking support and handling medication concerns. Here, we summarize the essential points covered during the session for a comprehensive guide.
Parkinson’s UK is a leading charity dedicated to improving the lives of people affected by Parkinson’s disease in the United Kingdom. Established in 1969, the organization provides vital support, information, and resources to individuals living with the condition, as well as their families and caregivers. Parkinson’s UK also funds groundbreaking research aimed at finding better treatments and ultimately a cure for the disease.
Parkinson’s UK held a Panel interview to highlight and educate those who are new to the caring role and want to find out more about supporting someone with Parkinsons. Below is a small summary of the panel interview, although if you want to watch the Panel discussion, please click on the video below.
Welcome to another blog post on carer / caregiver awareness from carer activist Matthew McKenzie. To see the video of this blog post, watch below.
Recognizing the Need for Help as a Caregiver: 10 Signs to Watch Out For
Caring for a loved one is often a rewarding experience filled with deep connection and personal satisfaction. However, it can also become overwhelming, exhausting, and challenging. Acknowledging that you need help is a crucial step in providing the best care for both your loved one and yourself. Here, we’ll explore 10 important signs that indicate it may be time to ask for help in your caregiving role.
Feeling Overwhelmed with Your Caring Role
Caregiving involves juggling numerous responsibilities, which can lead to constant stress and anxiety. If you often feel like you’re unable to cope, it’s a clear indication that you need support. Feeling overwhelmed is not a sign of weakness; it’s a human response to a heavy load. Remember, it’s perfectly okay to ask for help and share the burden.
Physical Exhaustion
The physical demands of caregiving can be immense. Lifting, moving, and assisting your loved one can take a toll on your body. If you find yourself frequently fatigued, or if you experience chronic pain or other health issues, it’s important to seek help. Ignoring these symptoms can lead to caregiver burnout, which ultimately benefits no one.
Emotional Strain
Caregiving can also be emotionally taxing. Signs of depression, irritability, or frequent mood swings may indicate that you need emotional support. Friends, family, or professional counselors can provide the necessary outlet for your feelings and help you manage the emotional strain that comes with caregiving.
Changes in Your Loved One’s Needs
Your loved one’s condition may worsen over time, increasing their care needs. When this happens, don’t hesitate to ask for assistance. Professional help can be crucial during periods of significant change, ensuring your loved one receives the best care possible while you adapt to new demands.
Neglecting Personal Needs
It can be easy to lose sight of your own health, relationships, and hobbies when you’re focused on caregiving. However, neglecting your personal needs can lead to serious health and emotional issues. Seeking help can give you the space to take care of yourself, restoring balance and allowing you to be a stronger caregiver.
Isolation
Feeling lonely or disconnected is a common experience among caregivers. This isolation can exacerbate stress and make the caregiving role even more challenging. Reaching out for support, whether from family, friends, or caregiver support groups, can help you reconnect and remind you that you’re not alone in this journey.
Crisis Situations
In times of emergency or when faced with making tough decisions about your loved one’s care, seeking help is essential. Attempting to navigate these moments alone can be risky. Professional advice and support can provide the guidance you need to make the best possible decisions during a crisis.
Lack of Knowledge or Skills
Caregiving often involves tasks that require specific knowledge or skills, such as medical care or managing medications. If you encounter tasks you’re unsure how to handle, it’s crucial to seek guidance. Professional help can ensure that these tasks are performed correctly, safeguarding your loved one’s health.
Inability to Maintain Routine
Maintaining a consistent daily routine is vital for both you and your loved one. If you find that daily routines are regularly disrupted and you’re struggling to manage time, consider asking for assistance. A little help can go a long way in restoring structure and reducing stress.
Need for Respite
Everyone needs a break occasionally. If you feel the need to take time for self-care or to recharge, don’t hesitate to ask for help. Whether this comes from family, friends, or respite care services, taking the time to rest is essential for maintaining your well-being and being an effective caregiver.
Conclusion: Seeking Help is a Sign of Strength
Recognizing and acting on these signs doesn’t mean you’re failing as a caregiver; it means you’re taking necessary steps to ensure the best care for your loved one and yourself. Asking for help is an act of strength and responsibility. Take the initiative today to reach out and seek the support you need in your caregiving journey.
Welcome to the November 2020 update of the Lewisham BAME carer forum. This forum is aimed at diverse carers in the borough of Lewisham, although carers and forum members from outside the borough are more than welcome to attend. When I am talking about carers, I mean unpaid carers who care for someone suffering mental illness.
For the Novemeber 2020 forum update the presenters were the following.
Professor Frank Keating – BAME community experience with the mental health system. Dr Emily West – The challenges on Dementia, Palliative and end of life Dr Laura Cole – Care home research Sherone phillips – NHS England Palliative and End of Life Care
Usually all of my carer forums tend to have speakers or those who engage with carers attend locally, however due to the corona virus and social distancing, the option is now available to increase networks to wider regions. The BAME carer forum for November had a dementia and end of life theme to it.
Dr Emily West presents
First to speak was Dr Emily West from UCL Division of Psychiatry. She spoke about a project called DeCoDe-H – Improving dementia care in acute hospitals.
Emily mentioned that they are looking at ways to basically make it easier to recognize and treat discomfort in people with dementia who can’t communicate, and then work a little bit on nutrient, which is one of the studies on caring for with people with dementia. The project also looks into how can they can best support family carers. Dr Emily also spoke about another project called Endemic, which was their COVID specific project, which kind of brings the two projects together.
Dr Emily mentioned to the forum that she inherited the project from a fellow researcher I think her name is Nuriye Kupeli. Dr Emily gave credit on the amount of work researcher Nuriye did. Dr Emily has also been working with Dr Nathan Davis, who’s a senior research fellow and is also was very interested in dementia, palliative care, and decision making, which together is called “Rule of thumb interventions”.
The most well known version of this is the “stroke intervention” and how it helps you to recognize and remember a very easy way of recognizing a stroke and getting help.
Dr Emily mentioned that Dr Nathan’s work is very carer focused and he’s looked at supporting family carers of people with dementia who are at the end of life, as well as helping dementia sufferers own decision making abilities. One in 14 people over the age of 65 have dementia, which is over 850,000 people in the UK, and almost half of carers have a long standing illness or disability themselves. So you have to be particularly aware of the needs of the people that are looking after the people that have dementia.
Dr Emily mentioned 36% of carers spend over 100 hours a week caring. And as well as this general context, they have been looking at how it affects BAME community specifically. So about 3% of people with dementia, which is about 25,000 people are from BAME communities and this number is expected to double by 2026. It’s predicted at the moment that South Asian communities are going to have the highest increase in the total number of people with dementia and current research tells us that BAME communities have a lot of challenges in dealing with dementia, almost every step of the process.
It was also mentioned that there can be delays in getting diagnosed with dementia and that sometimes this can be difficult to access. We know that BAME communities find it harder to access the services and we know that people from BAME communities report poorer quality in end of life care and as found in theMarie Curie report in 2014.
A big national drive on the end of life care strategy study in 2008, found a number of related inequalities and there’s a general feeling within policy or aim within palliative care that the UCL researchers are working towards that palliative care be seen as a human rights. Its also something that’s really enshrined everyone who has the right to have a good and well provided for death and dying process. It was stressed that it’s more important than ever to address the kind of base inequalities stopping a part of the population.
Dr Emily continued that it’s also increasingly recognized that the role of families and carers and members of the public in medical and health research is invaluable. Emilies research use a lot of what are called PPI panels. So public and patient involvement. And so PPI panels helped us throughout the research process to make sure that the way that we’re communicating is appropriate, and at the right level for the people that need to access the information. And they help us to design research processes, so that we’re not asking too much, or on the other side, we’re not assuming that people can’t do things aren’t willing to do things, but they are.
Those affected on those illnesses are usually involved in steering groups, so they help to shape the research agendas. This is something that’s open to everyone. Dr Emily did point out that if anyone’s interested, she can show people how to register for these kind of things. Dr Emily was happy that people are more widely being involved regarding dementia and end of life. This is especially on those with direct knowledge of certain illnesses and situations, they can help researchers develop more knowledge on such situations, and also knowledge how things have been across the span of weeks or months or years regarding those illnesses.
Dr Emily was aware that as researchers people can inform them and maybe tell us when things are okay and when they’re not. It was mentioned that the people that carers spend every day will observe what has previously been seen as an observable and can help facilitate voices of diverse populations. Researchers can’t reach everyone but they do try to reach and involve carers, patients and networks of people. So their aim is to represent all of the voices that should be heard, when researchers doing things like making clinical guidelines, or policy decisions.
Dr Emily West moved on to talk a little bit about a recent study that they have been doing. It’s a kind of case study, that she would be really interested to hear the kind of themes that they found when they talked to people. Emily resonated with people’s experience here. she knew that there’s a lot of experience in this group, and caring for people with lots of different illnesses, lots of different social setup, social challenges. Dr Emily was really interested to hear if this kind of applies the situation that members have been living in recently, too. COVID-19 is of course has a huge effect on health and social care systems.
Dr Emily continued by saying that they have had to do some rapid response approach to care planning and decision making because hospitals have been overrun regarding the virus and GP surgeries have been locked down and everything that people relied upon as normal has changed. So systems are having to respond to changing needs all the time, just as everyone else is responding to change in government guidelines, changes in where we can and can’t go and what we can do. COVID-19 has affected older adults much more seriously and a lot of these older adults have dementia, thus carers are having to make multiple very different care decisions in this situation.
Dr Emily said that they developed a decision aid and which in practice was kind of a little booklet, and just 20 sheets of a4. They wanted to do this to help carers of people with dementia to make decisions in these very difficult and very uncertain circumstances. We know that helping people make good decisions when things are unclear, can help grief after bereavement. It can also help people to feel like they know the situation more and it can even have an effect on things like arguing with your family about Which decisions are made and which decisions are being made. So there’s a good kind of basis for why we should help people make decisions.
Researchers have looked at doing this from a combination of different data sources, they wanted to hear as many voices as possible. So they interviewed helpline staff from from assignments UK and from Marie Curie, we looked at academic literature and newspapers and things for things that have been written about already. The researchers also looked at the online forums for as long as UK as well, where people kind of go online and talk to each other. The forums are not professionally led at all, it’s just people with a common interest talking about this. Dr Emily told us about what they found from looking at the literature the publisher already exists. So this review was looking at place of care in place of death and older adults.
Dr Emily then talked about things that specifically related to BAME experiences in what exists already. So they found the decision making seemed to be key, particularly within the role of the family. It was found that generic planning initiatives didn’t work well at all and that there was a much more positive response to truly tailored decision making schemes that took into account the way that people, for example, practice religion, or day centers, or community centers or festivals and things that people went to.
In an American study that the UCL researchers looked at as part of this, there weren’t any differences between ethnic or racial groups, in terms of how much they wanted to discuss end of life options with their doctors with hospital staff, but there was a difference in how much they ended up doing. So the problem is clearly on the side of the medical world here, because people want to discuss this, but for whatever reason, they’re not getting the opportunity to do So. As well as these general findings, they found some specific things that related to people with dementia and carers. One of these was the involvement of proxy carers and decision makers. Dr Emily mentioned a lot of people at the forum were familiar with this, that when a person lacks capacity, and they can appoint or can have appointed somebody who can make decisions on on their behalf.
Professor Frank Keating presents on his research
Professor Frank Keating was to present to the carers forum on social work and mental health in the Department of Social Work at Royal Holloway, University of London.
Prof Frank talked a little bit about some of some of the things the myths around stigma and the black community. Prof Frank perfers the term black because I don’t like the word BAME as it doesn’t sit with him. plus he wanted the audience to think a little bit about empowerment and think a little bit about the role of carers in supporting an individual who’s experiencing mental health issues.
Prof Frank’s research started mainly since 2000, and has focused on a very tricky relationship between the African and Caribbean communities and mental health services, which has been his concern to try and point that out and try and find out why this relationship is so intractable.
In the report that Prof Frank did in 2002 “Breaking circles of fear” they identified that there was fear on all sides fear from services, fear from communities fear from errors, hear from families. And and that sort of seems to drive a wedge between these various groups. So his work is trying to see how can we improve? That as he carried on his work, he became more acutely aware that there’s a group of people who are really significantly disadvantaged in this. So his work then shifted from looking at the African Caribbean communities in general, to specifically focused on black men.
He continued to focus on African and Caribbean men because he found that this is a group of men who were most significantly disadvantage, and also don’t see seem to have more difficulty in relation to the recovery and more and a difficult path in terms of recovery.
So his most recent project, where Prof Frank mentioned Estella from Community Wellbeing who was involved in the project, aimed at trying to talk to black men. Prof Frank wanted to know on his argument was that there must be men who are in recovery or have recovered from from mental health issues. So he wanted to talk to African and Caribbean men who self identify as being in recovery. This was not a definition imposed on them, the men had to identify themselves as being in recovery. So in the research they talked to 30 men, and these were men in London. They also used Leeds because the funder asked them to explore other areas as well as London, But basically, what they wanted to know from the men was, what, what’s their understanding of the recovery, and they also wanted to know what support covered recovery.
What was really interesting was what the men were talking to the researchers about, first and foremost the men wanted to talk about their mental health experience, and their early life experience and this was really important for the men. Some of the men Prof Frank talked to was actually out to the interviews and this has been empowering for them, although Prof Frank was just doing his research. The thing is Prof Frank mentioned we just don’t get a chance to talk about our stories and so his message to us as carers, is really to find ways of talking to the person about their story. Because sometimes we get so concerned about their medication, we get so concerned about their support in hospital. But oftentimes people don’t get their stories heard and their stories to listen to, and find ways of getting to documenting their stories.
Sherone Phillips – NHS England and NHS improvement palliative and end of life care program
Although Sherone works for NHS England and Improvement her main interest for engaging in the carers forum is because she is a carer. Sherone explained the difficulties of being a carer in which members were impressed and related straight away with her caring experience.
Sherone mentioned that we all know the figures, carers save the NHS and save the system a lot of money and energy, heaps of money, by the work that carers do, but carers do it because they love the people they care for and because they are there to support them.
Due to the theme of the forum Sherone spoke to us about how palliative and end of life care in the NHS as a partnership picture fits across the whole of the country. This isn’t just about London specific. The program for palliative end of life care sits around six principles about people
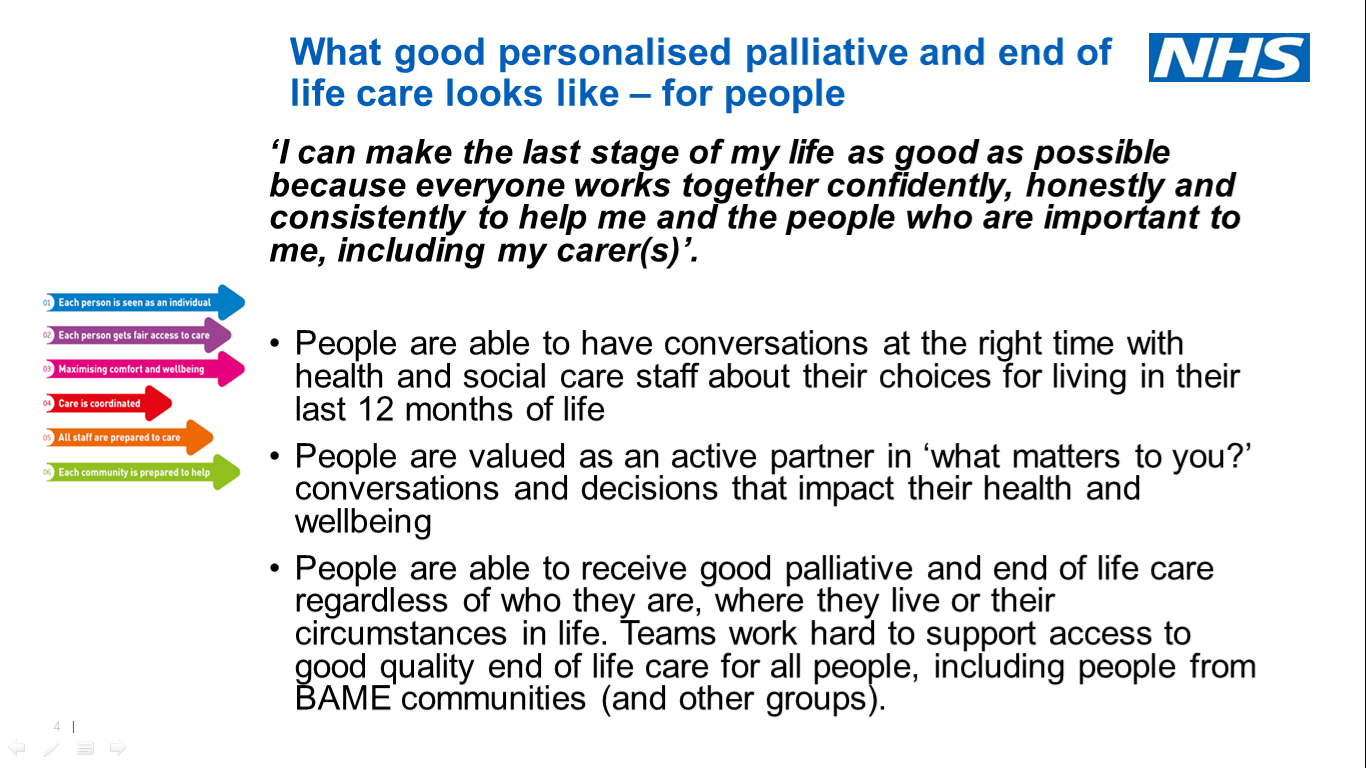
1 – That each person is seen as an individual. 2- Each person gets fair access to care, that there’s 3- maximizing of comfort and well being for the person who’s at end of life. 4- Their care is coordinated. So everybody involved, knows what they’re doing, who they’re talking to. And information is flows freely. 5- That all staff involved prepared to care. 6- That each community is prepared to help.
So the above are the six points that come out of the ambitions framework on life care regarding the NHS long term plan, universal personalized care comprehensive model, they ought to be six points for people. Where we work together and it’s not just about one team.
Sherone pointed out that the program includes all ages, from children who are palatable ends of life to adults and older people, everybody. Sherone also talked about NHSI (short for NHS England & Improvement) about program, to make sure that people with lived experience, so carers, people who have got a condition, which means they’re going to die soon, people who are at the end of their life with just a few months or a few weeks to live, NHSI will try their best to involve those viewpoints in what their developing. NHSI are not doing it alone they want to make sure NHSI are talking about equality, and making sure there’s minimizing or reducing and removing discrimination from all the different groups of people they can think about.
NHSI wants to focus on health inequalities from people who have got the poorest outcomes, the poorest health experiences who die sooner than they should, because they’re not getting the right support. NHSI are making sure that they are championing and pushing those discussions of those conversations through as they continue.
However what does this mean for people? What does it mean for you? What does it mean? For the people you love, what does it mean reality?
NHSI are talking about what personalized palliative and end of life care looks like. So in other words, what does it mean, at the individual level? Then the ambitions about the person seen as an individual and all those points, the six points mentioned, that this is about making sure that every stage of life, e.g the last stage of life is as good as possible, because everyone works together confidently, honestly and consistently to help the people who were important to us, including their carers. So that’s the statement, or does that mean in reality? Well, that the staff and the people that work with you, and with us and with our loved ones, have conversations at the right time and they have conversations at the right time with us, as well as with the whole the health and social care staff involved in in their choices about what they want to do, that people, including the carers have valued as active partners in the conversations.
It was exactly their findings that people want to know about what matters to them to be seen as an individual and that you have people who have good access to care and treatment at the end of their life, no matter who they are, where they live, or what their circumstances are, they should be supported with dignity, with care with compassion, and not with someone looking down their nose at you, that is a standard NHSI want people to experience.
NHSI want people to get the specialist care they need when they need it, and that their views and their preferences, what they want about the future care is known. These principles apply to care generally and support generally. So that’s the overview. As an organization that is part of the ambitious partnership, lots of different health and social care organizations are part of the ambitious partnership together with NHS England and NHS improvement, it is everyone involved in health and care, that design and talk about and plan for the services that make a difference
Dr Laura Cole presents on Care home research
Dr Laura from Kings College London wanted to tell carers at the forum about a study that they are conducting at the moment. Dr Laura is looking at residential respite for people with dementia and their carers. Basically Dr Laura meant a short stay in a care home. So not when somebody lives at home, and then they just have a breaks and maybe they spend a week or two or maybe more, but they come back home so they don’t permanently stay in a residential respite in a care home.
So the researchers know that respite may be quite beneficial for some people, because it provides a change of scenery, it provides the carer with a little break, and then the hope is that with that brake, the carer can continue caring for longer, and obviously, they’re able to do the things that they want to do, they can go on holiday, but also it is kind of a way of building resilience and getting strength back. Sometimes it can be something to look forward to as well. So it’s case of, I’ve just got a few more weeks to go and then I’m gonna got this lovely thing to look forward to or a break. And, and it can be beneficial for people living with dementia as well and as they have a break.
That is the reason for what the researchers are trying to do as they know that many people with dementia and their carers don’t access this service. So what they would like to do is interview people who have had the service, and then interview people who also have declined the service so that the reseachers can marry the two up and see what the the pros and the cons of residential respite are. Dr Laura had planned to do all this pre COVID so they were going to interview people in their own homes, and from from these two groups, so obviously, they still continuing with that, but they are doing it using zoom, over the telephone, though. They want to interview people living with dementia, and family carers about their experiences.
Welcome to the August update of the Lambeth Mental Health Carers forum. As a reminder the Mental Health carers forums are not primarily focused on discussing mental health benefits, but are aimed at carers supporting those with mental health needs. The forum usually has organisation who either provide mental health services, commission them or oversee the services e.g. Lambeth Council, South London & Maudsley, Lambeth CCG and Lambeth healthwatch besides others.
For the August forum we were fortunate to members and representatives from Maudsleys Older Adults and Dementia Advisory group. They presented to the forum what the group does over at South London & Maudsley and how they work with unpaid carers who are caring for those suffering Dementia, Alzheimers, Parkinson and so forth.
Before I continue on with a brief update of the work of the older adults Clinical Academic Group, we also had on the August agenda the following.