Welcome to another review post on lectures. This one is from the course on The Origins of the mind and I ll be trying to review lecture 18 called “Emotion Regulation And Mood Disorders”
The Course “Origins of the Human Mind” is taught by Dr. Stephen P. Hinshaw. Dr Stephen is the Professor of Psychology and Vice-Chair for Psychology for UC Berkeley. The course has 24 lectures all rich with information about the human mind, psychology and psychiatry.

Dr Stephen Hinshaw
Dr. Stephen on this lecture talks about mental health disorders mainly Bipolar disorders. He first looks at the similarities and differences regarding different types of moods. Dr. Stephen sums up moods as the capacity to regulate ones emotion. We need regulation over rage and other emotions otherwise our lives become uncontrollable.
He then examines how long an emotion can last, this is usually around up to a few seconds or more. The first emotion Dr. Stephen is interested in is the emotion representing disgust, as in spoiled food. Dr. Stephen references Paul Eckman idea that disgust transcends culture. Such as some other emotions.
Dr. Stephen questions how emotion is expressed from its begin, middle and end. He raises points on how emotion is recorded in our facial expressions, our reported feelings and also through psychophysiology that being our heart rate, sweating or breathing.
He mentions one of the core concepts of this lecture being the primary emotions, social self concious emotions that can be labelled as negative e.g. rage, sadness, fear. Dr. Stephen states that basic fears did help promote survival in our early ancestors. However now that we know a bit about negative emotions, what about positive emotions?
Dr. Stephen explains what positive emotions are and why they are needed. For instance love, bonding, happiness and also “CARING”. Positive emotions play a part in psychology where psychologists try to examine positive psychology, where people can be wired for good
Next on this lecture Dr. Stephen questions What is a mood?
This time he asks how longs do moods last? Well they can last longer than emotions, which is a few seconds, moods can last for hours to days, weeks and so on. Here Stephen feels moods change, depending on the situation. Dr. Stephen points out that it seems many of us are no good at predicting our moods, this being affective forecasting which looks at predicting how we feel, e.g. we predict our negative feelings.
Embed from Getty ImagesHe mentions another concept called “state dependency in mood” where we latch on to negative moods. Especially after a difficult event. This then leads on to how those who suffer from clinical depression.
Continuing with the lecture, Dr. Stephen explains the idea of “affective style” where people experience the world in simple characteristic ways. Too much of such experience can Lead to Neuroticism. Dr. Stephen feels it is important that such moods are not 100% biological and we need to consider other factors like environment and social influences.
The next part of the lecture looks at What is a mood disorder? Too many negative or positive emotions that can last for too long. Plus this is not only mood regulation, such disorders can affect us in other complex ways. We can suffer Sleep disorders, self perception problems and so on. Dr. Stephen Mentions “Albert Camus” reference regarding a philosophical question that we all ask ourselves at some point. This being “is life worth living?” So how long would it take for a negative mood to cause us to ask this serious question?

Albert Camus
Such a question has serious repercussions for sufferers of such disorders as the lecture will explain soon.
Dr. Stephen now begins to look at two mood disorders the first being major depression and bipolar disorder. What is Depression? Dr. Stephen explains a bit about Sadness and being pessimistic, in small lengths, we all get it, However we do not just experience sad moods, but such moods can greatly affect our sleep and food habits. This can lead to “All or none thinking” or “over generalising” or “internal and global stable causes“. Sufferers can fall into thinking where they can repeat to themselves “It happened because of me..me…ME!!”
The danger is if depression gets serious enough then sufferers can end up asking that famous albert camus question “Is life worth it?” There is a clinical term called “Major Depression”. With such a horrible dilemma, we soon are asked What are the triggers? Usually it can be things like a Major loss “death of loved one” or large failures. We all go through such events, but such situations can be dangerous if we are not supported.
Embed from Getty ImagesDr. Stephen raises an important question. When does “bereavement go and a major depression begin?” He feels this is not an easy one to answer, but if such moods goes on for a year, then something could be very wrong. Dr. Stephen then moves on to explaining “Unipolar depression”, where he talks about repetitive episodes of depression or mood swings. He explains the problem of sufferers who have experienced depressive episodes, which unfortunately will increase each time.
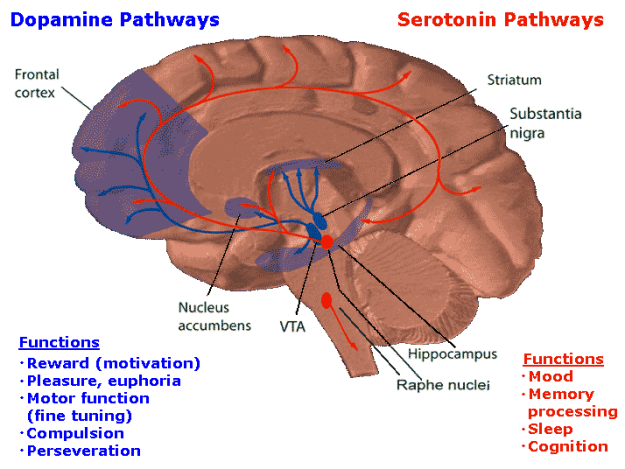
Here he examines the biology term regarding depression and its affect on our brain, where the levels of “Serotonin” and “Norepinephrine” tend to re-adjust, these will lead to changes in the “Hippocampus“. In psychological terms, we begin to feel that the world is a hostile place, this then leads sufferers retreating from the world.
Next Dr. Stephen moves on to discuss “Major Depression”. He starts out explaining the gender issue where a majority of females have higher rates, although before their teens both genders have same chances of depression, but after such ages the risk is twice for females, why?
Dr. Stephen Hinshaw continues the discussion looking at the gender statistics. He looks at the characteristics of females on their roles as Care givers and how they may worry about things. Dr. Stephen mentions how more woman and girls attempt suicide, but unfortunately more men complete suicide, due to using more lethal means to do so.
Interestingly enough, the suicide risk of those experiencing major depression is actually higher when they on the road of recovering from the disorder. A good reason for this is that the energy required to do the act is regained since depression tends to zap energy from sufferers, but once that energy returns then the risk to carry out desperate acts begins to rise.
Embed from Getty ImagesWe then look at how to explain depression, where the turning inward of anger or other negative emotions depending on how the event or situation had happened. This is called “Introjecton” a turning inward of emotion rather than display it because of social situations…e.g. leading to a form of “Repression”.
Suffers can lead to “white or black” thought patterns, “all or none” thoughts. To disfuse or treat such thought patterns, the use of Cognitive Behaviour Theraphy (CBT) can try to challenge such thought patterns. Dr. Stephen P. Hinshaw asks a complex question When can beliefs trigger depressed moods? or the sad moods themselves?
We all have Dorment or latent beliefs, but when something terrible kicks this into gear then we are at risk of such mood problems. So then how can we treat such conditions? Dr. Stephen P. Hinshaw feels that changing not only thoughts, but actions, medication (SSRI’s) can be effective, but they must all be fine tuned. Such treatments can help regulate “serotonin” levels.
Dr. Stephen moves on to describing “Mania” the mirror of depression. Mania are moods that are enhanced, where things speed up, expansive. “Hypo Mania” can be pleasant, but can get far worse if conditions persist. Here Dr. Stephen mentions the case where in 1973 Carlson and Goodwin describe the stages of mania. Here they Observed patients with and without medication, what goes on to stage 2 and 3.
Embed from Getty ImagesStage 2 leads to lack of control over ones situation, e.g. bad decision making and being bad management of money, outcast from work or society and so on. Next stage 3 leads to psychotic symptoms, hallucinations, hearing voices and delusions that can actually feed the mania. Here irritability sets in, plus physical strain and impulses begin to get out of control.
The lecturer explains that Bipolar disorder is now the new term for manic depression, hence the unfortunate chance a sufferer will get more repeated episodes of mania.
Embed from Getty ImagesThe last part of the lecture moves on to explaining how we try to predict depressive episodes, for instance how sufferers fall ill during winter or low or reduced sunlight, however “mixed states” are far more difficult to try to predict or prepare for. Suicide spikes are unfortunately very high for “mixed States”. Interestingly artists, poets, dancers and creative people tend to have higher rates of bipolar disorder or mania and if one studies sections of the news or magazines it is not uncommon to find celebrities opening up about mental health conditions.
What is more difficult to bear is that bipolar has also a very high genetic heritability, although relatives may also get the trait where they have high drives which can be a great advantage to success, although one might think twice if they had a choice to inherit such bipolar conditions.
Embed from Getty ImagesDr Stephen looks into how bipolar can be treated, although unfortunatly it cannot be cured. Lithium and newer generation of medications are of use. The big problem is non-complience as sufferers may wish for the old manic highs that they used to have without considering the repecutions. E.g. how dopamine levels kick into gear regarding drug users.
If you affected by the descriptions in this review. Here is a link where you can get advice and support.
http://www.nhs.uk/Conditions/Suicide/Pages/Getting-help.aspx
