If you weren’t able to join us for this month’s online forum, you missed a deeply insightful session packed with research updates and honest conversations. As a carer myself, I know how hard it is to find time for these meetings, so I’ve put together this expanded summary to keep you in the loop on the vital work being done for our community.
Meeting Agenda
- Welcome and Intro: The role of the Patient Care Race Equality Framework (PCREF).
- Speaker 1: Brenda Hayaka (King’s College London): Findings on ethnic inequalities in healthcare and the new “Interception” study.
- Q&A Session: Addressing dementia stigma, medication, and language barriers.
- Spirituality & Faith: Insights from Tuulia Castledine (Chaplain at SWLSTG) on recovery and holistic care.
- Speaker 2: Becky Forster (University of Southampton): Supporting carers facing harmful or upsetting behaviors.
- Local Advocacy: Healthwatch Croydon’s role in gathering carer feedback.
- Closing: “Rooted and Growing” (A PCREF poem).
Key Speaker: Brenda Hayaka – The Interception Project
Brenda shared findings from her previous work on ethnic inequalities and introduced her new study on Multiple Long-Term Conditions (MLTCs).
Brenda Hayaka opened her keynote by sharing the heart behind her work on ethnic inequalities in healthcare. Drawing on her previous research, she described how minoritised ethnic patients and their carers often face significant challenges navigating multiple long-term conditions (MLTCs) with little support or recognition. She emphasized that while global interventions exist for conditions like diabetes and depression, there is a notable gap in UK-based research specifically addressing MLTCs in minoritised communities. This “major evidence gap” became the driving force behind her current study, The Interception Project.
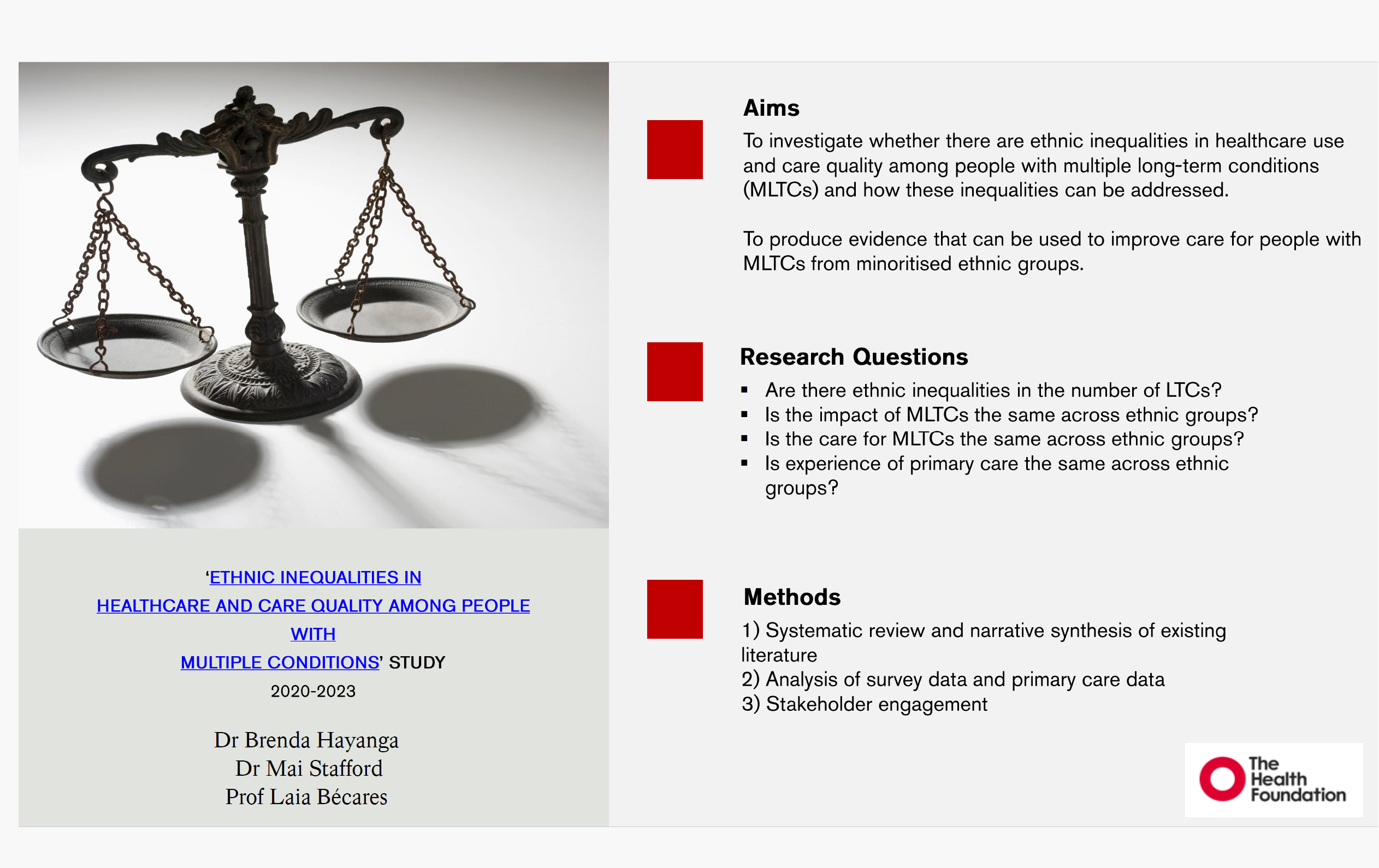
What the Research Shows:
- Systemic Disadvantage: Minoritized ethnic groups are disadvantaged from the development to the management of multiple conditions.
- Poor Continuity of Care: Many experience poor therapeutic relationships with practitioners.
- The UK Evidence Gap: While interventions for depression and diabetes exist globally, Brenda found zero studies specifically targeting MLTCs for minoritized groups within the UK healthcare system.
The “Interception” Study:
The Interception Project uses a creative and collaborative method called journey mapping to trace the lived experiences of patients and unpaid carers. Brenda explained that this approach goes beyond merely collecting data: it seeks to identify the pathways people take when seeking help, the barriers they encounter, and the moments where the healthcare system fails them. By listening deeply and reflecting these experiences back to communities, the research provides actionable insights into improving care quality and equity. The study is expanding beyond London to include Coventry and Manchester, recognizing that every community has unique strengths, challenges, and solutions.
Brenda highlighted that a central aim of the project is to co-create actionable recommendations with communities. These recommendations are intended for NHS leaders, commissioners, and policymakers, ensuring that the voices of carers and patients directly inform service design and delivery. She also spoke about the role of trusted community leaders in building access and overcoming barriers such as language differences, mistrust of institutions, and cultural stigma around certain health conditions. Faith communities, she noted, can play a crucial role not only as support networks for participants but also as partners in research, data collection, and advocacy for change.
Throughout her presentation, Brenda emphasized that understanding the journey of carers and patients requires attention to both systemic and relational factors. Minoritised ethnic groups often experience disadvantages in developing and managing multiple conditions, and poor continuity of care can weaken therapeutic relationships with practitioners. By documenting these experiences in detail, the Interception Project aims to fill the evidence gap and provide a roadmap for more equitable, culturally sensitive care. Brenda closed her keynote by reminding attendees that meaningful equity in healthcare begins when previously invisible experiences are recognized and acted upon—a call to transform insight into change.
Spirituality in Care: Forum Introduction by Matthew McKenze
I had the honor of opening the spirituality segment of the forum, emphasizing the vital role that faith and cultural practices play in supporting carers and patients from minoritised ethnic communities. I framed the discussion around the idea that mental health care cannot be fully effective unless it recognizes the whole person, including their spiritual and cultural identity. I highlighted that carers often draw strength, resilience, and meaning from their faith, and that this dimension is frequently overlooked in traditional mental health services.
I encouraged participants to consider spirituality not as an abstract concept, but as a tangible resource that can inform recovery, foster belonging, and enhance coping strategies. By acknowledging spiritual needs, mental health providers can build trust with communities that have historically experienced marginalization or misunderstanding within healthcare systems. I also set the tone for an open and reflective conversation, inviting attendees to share experiences, insights, and challenges related to integrating faith and mental health support.
By positioning spirituality as both a personal and systemic consideration, the forum aimed to explore how services can better engage with faith perspectives in a respectful, inclusive, and practical way. This introduction laid the groundwork for Tuulia Castledine’s keynote, which delved deeper into the spiritual tools and frameworks that support carers and patients in their mental health journeys.
Spirituality in Care: Insights from Tuulia Castledine (SWLSTG)
We were joined by Tula, a Chaplain from South West London and St George’s (SWLSTG), who led a vital discussion on the spiritual dimension of mental health.
Tuulia highlighted that for many carers and patients, faith is not just a personal practice but a framework through which they make sense of mental health crises. Spirituality often provides a lens for understanding why challenges occur and offers a source of hope, helping individuals navigate uncertainty with resilience.
Beyond offering meaning, Tuulia explained that spirituality can serve as a practical tool in recovery. It provides a “language for recovery” that allows carers and patients to express experiences and emotions that might otherwise be difficult to articulate. This sense of connection fosters belonging and strengthens the psychological resources people draw upon when coping with mental health challenges.
Tuulia also stressed the importance of services adopting what she called “spiritual curiosity.” Mental health professionals are encouraged to engage openly with faith perspectives rather than making assumptions or ignoring them. By integrating spirituality into holistic, person-centered care, services can better meet the needs of minoritised ethnic communities.
Finally, Tuulia highlighted a critical concern: when services fail to acknowledge faith, they risk deepening the mistrust that many minority communities feel toward mental health providers. Recognizing and valuing spiritual needs, she emphasized, is not just compassionate—it is a crucial component of equitable care, fostering trust, understanding, and more effective therapeutic relationships.
Summing up Tuulia’s talk
- Making Sense of Illness: For many, faith is how they make sense of why a crisis is happening and where they can find hope.
- A Tool for Recovery: Spirituality provides a “language for recovery” and can build resilience and a sense of belonging.
- Moving Beyond Assumptions: Tula emphasized that services need to show “spiritual curiosity” and include faith as part of holistic, person-centered care.
- The “Mistrust” Gap: When services ignore faith, it can deepen the mistrust minority communities feel toward mental health providers.
Carer Voice: Questions & Feedback
The Q&A session was one of the most powerful segments of the forum, offering an unfiltered view of the real-world barriers faced by carers and minoritised ethnic communities. Participants shared candid experiences, highlighting gaps in current mental health support and pressing for practical solutions.
A professional opened the discussion by addressing the critical issue of language and access. She pointed out that many research projects and healthcare initiatives fail because they do not allocate adequate resources for language interpretation or accessibility for disabled individuals. Without these provisions, vital services and studies inadvertently exclude those who may benefit most, leaving carers and patients marginalized.
A carer contributed a particularly thought-provoking critique regarding medication versus conversation. He challenged the system on why Black men are often prescribed stronger medication for longer periods rather than being offered meaningful dialogue and psychosocial support. This raised an important conversation about the need for culturally sensitive approaches to treatment that value listening, understanding, and relationship-building alongside pharmacological intervention.
The unpaid carer also highlighted the challenge of dementia stigma within older generations of minoritised communities. He described how deeply ingrained cultural perceptions can make it difficult for families to seek early support or even acknowledge the condition, creating additional stress for carers. The discussion emphasized that tackling stigma requires both education and culturally attuned engagement, alongside support networks that respect the values and experiences of carers and patients.
A mental health professional from another mental health NHS trust added a vital perspective on community engagement and trust-building. He emphasized that carers often encounter inconsistent communication from services and a lack of culturally informed support, which can leave families feeling isolated and unsupported. He urged healthcare providers to work more closely with community leaders, faith groups, and carers themselves to co-design services that truly respond to the specific needs of minoritised ethnic communities.
Overall, the feedback session underscored that systemic improvements must be informed by the lived experiences of carers. Their insights illuminated the gaps between policy, research, and practical care, reminding the forum that real change is rooted in listening to and amplifying these voices.
Support for Carers in Crisis
Becky Forster introduced a deeply important new study funded by Marie Curie, focusing on carers who find themselves in extremely challenging and sometimes frightening situations. The research aims to better understand the experiences of carers who have faced harmful, aggressive, or abusive behaviors from the person they care for, particularly at the end of life. Becky emphasized that these situations are often overlooked in traditional guidance, leaving carers without the support or strategies they need to cope safely and effectively.
The study seeks to gather real-life experiences from carers, acknowledging that their insights are invaluable in shaping practical and compassionate guidance for healthcare providers. Becky explained that the goal is not only to document these difficult experiences but also to translate them into actionable tools and recommendations for the NHS, ensuring that carers receive timely support, protection, and training when dealing with complex end-of-life care scenarios. By centering the voices of those who have lived through these crises, the project hopes to reduce isolation, increase safety, and enhance the wellbeing of carers facing some of the most emotionally and physically demanding circumstances.
Becky encouraged attendees to participate and share their stories, reassuring them that contributions would remain confidential and that their experiences could directly influence policy and practice. This initiative highlighted the critical need for systemic recognition of carers’ emotional and practical needs, ensuring that they are not left to navigate trauma and stress alone. The session reinforced that understanding, guidance, and compassionate support are essential for carers’ resilience and for providing safe, dignified care to those at the end of life.
Croydon Healthwatch
We concluded the forum with an important reminder from Anna of Healthwatch Croydon, who emphasized that anyone in England has the right to provide anonymous feedback on their care. Anna highlighted that this is more than a formal process, it is a powerful tool for carers, patients, and communities to have their voices heard. By sharing experiences of both excellent and inadequate care, individuals can directly influence how services are shaped, highlight gaps in provision, and push for improvements where they are most needed.

Anna also underscored that feedback plays a crucial role in holding policymakers and healthcare leaders accountable. When carers and patients report their experiences, patterns of inequality, or systemic barriers, it creates evidence that decision-makers cannot ignore. This feedback is particularly vital for minoritised ethnic communities, where historical mistrust and underrepresentation have often left issues unaddressed. She encouraged all attendees to see feedback not as a bureaucratic exercise, but as an instrument of empowerment, helping to drive change at both local and national levels.
I closed the session with my poem “Rooted and Growing,” celebrating that we don’t have to lose our identity to get the care we deserve.
Matthew McKenzie
Mental Health Carer & Forum Chair
