Welcome to a brief update for my Greenwich mental health carer forum. One of the carer groups I run with the support of Greenwich carers. As usual the forum focuses on unpaid carers who care for someone with serious mental ill health. The forum runs very 2 months since I mostly focus on my other group for greenwich, which is a carer peer support group.
The greenwich MH carer forum also focuses on engagement with unpaid carers rather than a peer supportive environment. Speakers for the Greenwich MH carer forum were as follow.
Victor Aigbe-Anderson – Social Care Assessor
We also had engagement from Greenwich CCG who have been active engaging in my carer groups.
Here is the brief update of my South West London carers forum for July. As mentioned, I have not been blogging much due to working on my 2nd book on unpaid mental health carer experiences. I still run my carer groups including helping out West London NHS health trust on their Black Asian minority carer peer group.
However back to South west London.
The following speakers for July were
Phoebe Averill – PHd Student at Kings College Carol Ellis – Carer speaking about her son’s new book Ros Spinks – NHS England Commitment to Carers programme Myself on Why unpaid carers must hold to account
PHOEBE AVERILL PRESENTS ON HER PHD PROJECT
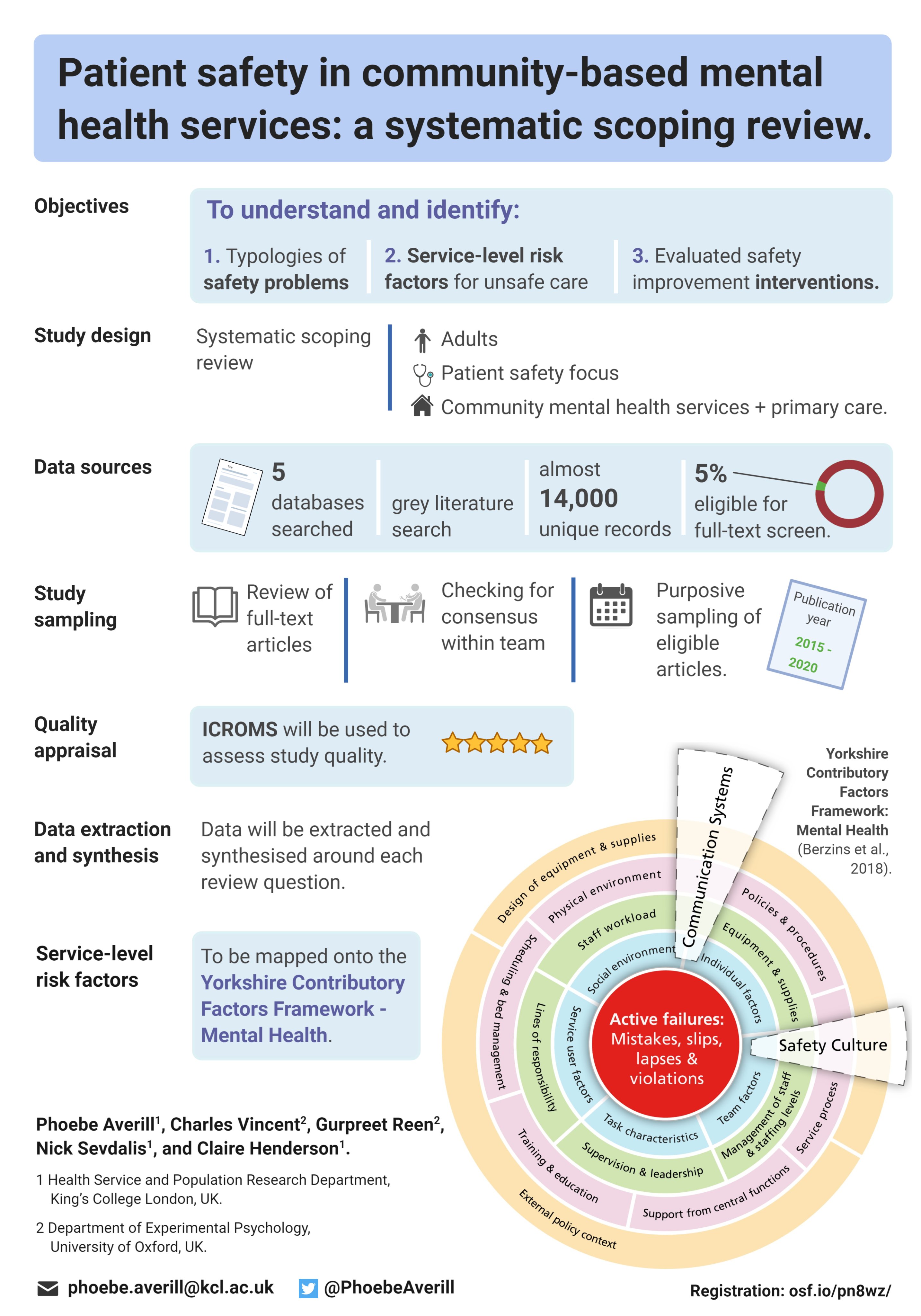
Phoebe from Kings college University spoke about focusing on safety and quality of care in community mental health Services. So as part of the research, she wanted to invite carers to share their views. Phoebe wanted to give us just a little bit more info about the research as the problem of patient safety hasn’t really been a given as much research which is limited, although there is a growing amount of research from those interested in this area. Still, it’s mainly focused on inpatient mental health services. In actual fact, most mental health care experiences are actually in community settings.
So that’s really important that patient safety in community mental health settings are researched as well. So that’s what she is trying to do with the research. Phoebe is speaking with families and carers of adults with mental health problems in the community services. What she is trying to find out is what kind of “safe and unsafe” care means to the carers in this context, because it’s not very well Understood. She would like to know what types of safety issues you worry about as carers and any ideas about what can make community mental health care safer and would could improve the services. There really is no right or wrong answers, it is about hearing carers experiences and opinions.
Phoebe also has spoken to services as well as to healthcare professionals, but it’s really what the carers views are? So what does the actual study involve? It will be a discussion with other carers since that will be what kind of format unpaid carers prefer.
For more information about the project I have included a screenshot below.
There were quite informative questions from carer members of the forum, but I have a lot to catch up with. So will move on to the next presentation.
Carol Ellis and her son talks about his new book
Carol’s son Shaun Ellis started off talking how he ended up with depression due to the death of his father. His book “A Gentle Breeze: Living with depression” focuses on how he managed to survive attempted suicide and his journey battling depression.
Shaun wanted to highlight such experiences through his words and actions. This is why he chose to write a book about his experiences. In this book Shaun describes all the techniques he used to battle his depression. As well as sharing his story, he wants to reach out to fellow suffers and encouraging them to seek the help they need.
Shaun then read a couple of passages from his new book, which led to questions coming from the carer members of the forum.
I have placed a link for those interested in the book below.
Ros Spinks from NHS England & Improvement presents on the Commitment to Carers programme
Ros from NHS England kindly engages with some of my carer groups I run online for half of London. She spoke about her role as one of the regional carer leads, however she covers London, while the rest covers England. Ros spoke about how the ‘commitment to carers programme’ is linked to NHS Englands long term plan, which is actually 2 years old. Ros talked about one of the big areas which are the quality markers in primary care. These are a set of standards that carer’s should expect from any GP practice across the country. However it is not mandatory, which is a bit of a challenge, because it can be difficult to get GP practices to do things in different ways, not because they’re bad practices, but due to such challenges.
Another quality marker is on identifying carer’s because there are still issues regarding the identification of carers in health and social care. It might be that some people do not identify themselves as carers, but that is not the point. It is up to the NHS and social services to help people understand and help educate them on what support they can get as an unpaid carer.
There was a Q & A session from members of the South West London carer forum.
One question was on why are the quality markers not mandatory.
Ros mentioned there has been discussion to make those mandatory, but raised the option that some GP practices work differently and would learn better from other GP practices in a network. Sometimes it is better to try different options ranging from training to rewards if GPs do well in identifying carers. Ros mentioned there is some leverage with the CQC as they use the NHS England quality markers to see if GPs are actually listening to their patients and carers.
Another question focused on what would Ros like to see in place to bring equality to unpaid carers to the level their patients have.
Ros felt she would like to see fantasic carer support centre that actually has the resources to care for the unpaid carer. She would also like to see a carer’s champion just like what they have in the GP practices in the London bourough of Hilligdon. Those in the GP practice could act as the carer champion, which could be the receptionist or GP and surprisingly it does not cost anything, they can help being carer friendly, identify carers and help refer them.
Another question which was very important came from a carer wanting to know what secondary care was doing for carers and if they follow NHS England & Improvement quality markers.
Ros was delighted such a question was asked and she mentioned hospitals were working towards a carer’s card or passport, actually some hospitals already have this and it is a recognition that a patient has someone who cares and that carer does need support and to be kept informed, infact the best secondary support from hospitals is that the carer will be involved in all the care decisions made and not just told what will happen or the carer be seen as an afterthought.
There were many other questions raised from carer members, but below was the one raised by myself on the commitment standards as I was interested in how NHS England’s Commitment for Carers has been progressing since it’s release around 2014. Ros responded to all of them, where some of the responses I have added below since at the time of the document it mentioned a few tasks were ongoing.
NHS England to raise the profile of what a carer does and how they can be supported with health care staff.
NHS England signed up and supports and promotes annual Carers Week campaign.
Establish a NHS England board level ‘Carer Champion’ and support NHS England board level members to shadow a carer.
A senior NHS England Carers Group to take ownership of the ‘Commitment to Carers’ document and NHS England’s support for carers.
Ros mentioned it is Jenifer Kenward who is on the senior management team and she links to the departments health and social care as well.
Collaborate with carers’ organisations to establish how carers award schemes might be extended to commissioners to support improving the experience of carers across England.
Ros responded these would be your Carers UK and Carers Trust organisations.
NHS England in partnership with NHS IQ to hold a national NHS Young Carers event to support how young carers can be better supported and the wellbeing of young carers promoted by the NHS.
Ros responded that usually three times a year, every region has a certain amount of young carer champions that come together to help drive the young carer’s strategy.
NHS England to support a Carers Champions Network bringing together the healthcare and carers groups.
NHS England will continue to implement the Equality Delivery System for the NHS, involving staff, patients, carers and the community to ensure equality is embedded within all of its core business including workforce development.
Ros mentioned NHS England has to do this, its practically a legal duty, she went into more detail about this.
NHS England is committed to supporting innovation in the NHS and will ensure that innovative ways of engaging with and providing care for carers are considered through the national innovation fund schemes.
Priority 1 Raising the Profile of Carers
NHS England to support the relevant bodies, including Health Education England, to support the use of packages for health care staff that increase carers awareness, and support staff to identify, involve and recognise carers as experts, and as individuals with their own needs, choices and aspirations.
On this question, Ros stated that Health Education England do have a training package that actually includes all frontline staff to increase carer’s awareness. Ros still mentioned there still is a problem to make training mandatory and she would very much like to see that.
NHS England to support the relevant bodies in signposting carers to information and advice about support available. The reason I asked Ros this question was because I felt even though resources are out there for carers, it seems not many carers are using them. I am aware there are social perscribers, but they seem geared for older adults to combat loneliness or for patients.
NHS England to contribute to increasing the awareness within the NHS of the duties and functions of local authorities with regards to carers.
Ros spoke how NHS England has made big strides on this task specifically for Integrated Care Systems (more on that in my September carer forum for Lewisham where Ros spoke about ICS Changes). Ros mentioned there has been much improvement and better awareness from a strategic level to the local NHS level.
NHS England and NHS IQ to liaise with carers organisations and the Royal College of General Practitioners (RCGP) in order to support their work on identification, implementation and sharing of best practice models. (Again, I tend to bother the Royal College of GPs because I was interested in an update to the RCGP carer’s strategy when Judith Cameron was the RCGP Carer leads).
Ros responded this would be on the quality markers from NHS England, but there was also recently a series of events from the Royal college of medicine regarding the focus on unpaid carers.
Priority 2 Education, Training and Information
NHS England to investigate approaches to measure the skills, confidence and knowledge of carers and potential benefits on care and carers.
Data sharing: As part of the Patient Online programme, NHS England to scope the potential for carers to access the GP medical records of the patients they care for, where applicable, and the patient has given their consent.
Ros mentioned a huge amount of work has been done on this since 2014, although due to COVID-19 happening she admits work on this has slowed down. Ros states hospitals should have the access to pull patient GP data if a patient turns up to hospitals very unwell and unable to speak for themselves.
NHS England’s new ambitions for End of Life Care, to be published in June 2014, will include the intentions for support for carers and bereaved relatives.
Ros again talked about the personalisation agenda as there has been a lot of work done on this. We spoke about the lead for end of life care who is Sherone phillips, although Ros mentioned there is a regional lead and a national lead for End of Life care.
NHS England to support timely dementia diagnosis and the best available treatment for everyone who needs it, including support for their carers. For example, the revised Dementia Enhanced Service will include an offer of a health check for carers and signposting for information and support.
Develop a programme of work to support the health and wellbeing of carers through the community nursing strategy.
NHS England’s widening digital participation programme to reduce inequalities: ‘100,000 citizens trained in basic online skills to boost health literacy’ will apply to carers as well as patients.
Ros mentioned this is NHS digital and a lot of work has been done on this, but there is more to do.
Priority 3 Service Development
NHS England will promote and work towards parity of esteem for carers so that mental health and wellbeing is considered and supported alongside physical health needs.
Through work on developing the House of Care toolkit, NHS England will work to bring together all the relevant national guidance, published evidence, local case studies and information to support carers to be informed and engaged in care.
NHS England to include carers in work around developing standards and service components for personalised care planning to help ensure carers are integral to the care and support planning process and are consistent with the National Voices principles of care and support planning.
Ros stated this does happen and that it is important to involve the public, patients and carers into the planning of personalised care. A good example is the work done with people with learning disabilities and those that support them regarding annual health checks.
Patients who can benefit will have the option to hold their own personal health budget resulting in direct benefits to carers, including feeling more in control and perceived health improvements.
Ros mentioned this happens through the personalised care.
Priority 4 Person-centred, well-coordinated Care
Scope how NHS England can most effectively support the RCGP and other partners in the work they intend to develop around carers.
I queried if NHS England also work closely with RCGP, RCPSYCH, RCM and others. Where Ros mentioned they do work across different programmes.
NHS England will consider how carers can be supported through commissioning of primary care including through future developments to the GP contract and enhanced services.
Ros mentioned at some point NHS England pulled back from this, but now there are discussions in place.
NHS England to work with NICE and other partners to develop measurement and best practice guidance in order to increase identification of carers.
Ros mentioned this happened last October, so NICE have issued guidence on how carers should be treated and it complementary to NHS England’s quality markers, it should not replace them. (I have posted a link below that might relate to what Ros mentioned).
NHS England to undertake a series of regional evidence summits for carers to establish an independent assessment of the evidence in order to capture, disseminate and encourage good practice.
Ros talked about how the above has happened and has probably morphed into innovated care systems. So this is how NHS England know how Yorkshire, Devon, Surrey have all these brilliant carer strategies, of there are other places as well.
NHS England to maximise opportunities to capture feedback and incorporate into discussions and work to improve quality and inform best practice.
Ros feels this feedback are from monthly calls from carers.
NHS England to undertake a piece of work to understand the impact of current commissioning incentives and system drivers in supporting carers. For example, through the GP contract, revisions to enhanced services for unplanned admissions and dementia.
Ros was not sure, it would be before her time, but it sounds like a one off piece of work, but can follow up on this with us.
NHS England to review current national processes in place to gather bereaved carers’ views on the quality of care in the last three months of life in order to address gaps in evidence.
Where commissioners identify the need for support, co-produce practical tools and a support programme of implementation with NHS IQ.
Priority 6 Commissioning support
NHS England to coordinate effective ways of working by developing partnership links between health, social services and other organisations, including the voluntary sector to establish how carers can be supported as effectively as possible.
NHS England to continue to work with the Standing Commission on Carers.
NHS England to remain a member of the cross government carers strategy board and will encourage and support carers organisations to play an active role in the Collaboration for Coordinated Care.
Establish an annual meeting with key partners including carers organisations to monitor progress and review objectives.
Priority 7 Partnership links
NHS England to continue as a corporate member of Employers for Carers.
NHS England to continue to implement and support established policies on flexible working, leave and emp
There were more discussions raised about NHS England & Improvement commitment to carers, but for more information you can check out NHS England’s Bi Monthly Carers Programme Lunch and Learn Webinar. The link is below.
This was a brief update for my South west London carers forum for July 2021.
It has been a long time coming since I have been so busy on writing my 2nd book which is title “Experiencing mental health caregiving – unpaid carers”. I have decided to take a break on my book and do another blog update. As usual I host many carer support groups and carer empowerment forums. This blog post is an update of my Lewisham carer forum.
The speakers for August were Denis Muganga who is the Service Manager for Lewisham In-Patient MH Services and works at South London and Maudsley. Denis is also deputy head of nursing at the mental health wards in Lewisham.
Denis spoke about Reducing Prone Restraint on Lewisham Acute wards. Many families and those caring for loved ones are often worried about the risk of restraint on mental health wards. Once a patient is in the care of mental health inpatient services then it is out of unpaid carers hands and we have to take a step back.
Welcome to a brief update of my BAME carers forum for the boroughs of Bromley, Lewisham and Greenwich. The focus is one of the 6 carer forums that focuses on discussions, awareness and campaigns regarding unpaid carers from an ethnic background specifically caring for a ‘loved one’ suffering mental ill health. Forum members do not have to have someone using the services, it could be they are caring for someone who might not be using the services of South London & Maudsley NHS Foundation trust or Oxleas NHS trust.
The BAME mental health carer forum update for July had the following speakers to engage with carers, although not in order.
Lola Jaye (psychothearapist, author, speaker) – Why race matters when it comes to mental health
Emma Wakeman (St Andrew’s Healthcare)- on The Missing Voices: Carers’ Experiences of Section 17 Leave (Mental Health Act 1983)
Kuldip Kaur Kang (West midlands trust) – on Religious and cultural needs of BAME mental health inpatients request
Rachel Nethercott – Carers UK focus on diversity unpaid carers
Leonie Down (SLaM Lewisham Head of Occupational Therapy and Partnerships Lead ) – Update on Patient Carer Race Equality framework
Dominic Parsons – Bromley, Lewisham & Greenwich Mind on their diversity initiatives.
Professor Shirin Rai from Warwick University – On the Impact of covid-19 on bame carers
Judging by the speakers, you can see the BAME carers forum is held online and is also attended by mental health NHS trust staff working to understand the issues that affect ethnic unpaid carers and patients.
Welcome to the July update of my Joint Southwark & Lambeth Carers forum. The forum is focused on unpaid carers who care for someone suffering mental ill health.
Speakers for the July forum were
Carol Ellis: Promoting her son’s book regarding surviving suicide
MP Helen Hayes – Speaking about carer updates for the boroughs
Dr Natasha Tyler – An associate Researcher from University of Manchester
DR NATASHA PRESENTS ON HER RESEARCH.
Dr Natasha started off by saying that as a researcher from the University of Manchester at the patient safety Translational Research Center. She has been working with Matthew probably for about three or four years now. He’s been involved in quite a bit more research and she was just going to give a little bit of an overview about involving carers in quality and safety research. Dr Natasha wanted to speak a little bit about involving carers in quality and safety research.
The Black Thrive Lambeth Partnership is inviting Black individuals, organisations and allies that are striving for an equal society to join our CommUNITY Assembly on 18 September 2021 for honest discussions about how together we can achieve real change for Black communities in Lambeth.
Welcome to the July 2021 update of my Lewisham mental health carers forum. The forum focuses on engagement for families and unpaid carers who care for someone suffering mental ill health. The ‘cared for’ does not actually have to be using mental health services, but it is important there is a platform for unpaid carers to learn about mental health support, understanding mental health and what is available for carers themselves.
Speakers for my July carers forum were:
Phoebe Averill – PHd Student at Kings College Polly Pascoe – Lewisham CCG Carla Fourie – SL&M director of social care
Phoebe Averill presents on her latest study.
First to speak was Phoebe Averill who is a PhD student at King’s College. She is working with South London & Maudsley NHS Trust (SL&M) on a research study and she wants to hear carer member’s thoughts and also invite anyone that might be interested in taking part in the research study. She is looking at safety of care in the community mental health services. Phoebe gave my forum a bit of background information about what the problem is. Basically safety in general hasn’t really been given much attention in mental health services. Historically, when you compare it to kind of physical health care services, where we’ve now got quite a good idea about how we can make care safer, what types of interventions and strategies might be needed. Still, there is a small kind of body of research and interventions coming out more recently. These are mainly focused on inpatient mental health services and unfortunately community mental health services have been a little bit left behind, even though that’s where the majority of people who are actually receiving care.
In recent figures, people were using community mental health services rather than inpatient services. So it’s really important that safety is kind of better understood in the community context, so that strategies can be developed to make the services safer. And that’s what she is trying to get started with this research research. Pheobe is currently trying to speak to family members and carers of adults who are using community based mental health services, to find out a bit about what they think about what safe and unsafe care means in this context, because it’s not really well understood. This is due to the types of safety issues that the carer is worried about in relation to the person that they support.
The way the study works involves speaking to her in a either a one to one interview or group discussion with other carers if there was interest from several people in taking part. And there aren’t really any right or wrong answers. It’s really just about hearing carer’s point of view. Carers have so much knowledge about the person that they support and their experiences of care. And it’s just really important that their views are incorporated into any efforts to, to make services safer.
Questions from carer members.
One question was focused on the issues of patient’s age. The carer felt that a 75 year old patient does not have the same issues you’d have with a 25 year old and they were curious to know, what Pheobe would be doing for older adults when it comes to community work? Especially for the carer because there’s a lot of issues with older carries with physical issues. How will the research be monitoring those patients or those carers?
Pheobe responded that unfortunately for this study, we’re only looking at sort of general adult services. So we’re Other than older adult services, like you mentioned, it’s not because it’s any less important. It’s just that at the moment, there’s the most kind of research knowledge in adult in adult safety. so future studies would be needed to look at older adults, because there’s like you mentioned, there’s lots of really important safety problems there.
Statement from myself
After some debate I mentioned that one thing in regards to research is that whatever is found out could lead to recommendations, usually, most research initiatives tend to recommend some findings that will have this influence services. A lot of people feel research is done for either funding on does not solve service issues, but I pointed out researchers are not in charge of mental health services.
Polly Pascoe – Lewisham CCG Presents
Polly spoke about her work within Lewisham Borough Council and southeast London CCG. Her role is it was called integrated Commissioner for mental health pathways. In essence, one of her key roles is getting us to use future systems across mental health care, while it’s occurring across healthcare in general, her focus is on mental health especially within Lewisham. This is kind of where we’re hoping to head moving forwards. The previous system, that being health and social care worked separately regarding statutory and voluntary. Such as Provider sectors were working separately and sometimes even competitively where age groups were handled separately, and such services provided different levels of focus and funding. Conditions were often handled separately, and there was a strong focus on outputs as in numbers, rather than changes necessarily. So there used to be a strong focus on reaching particular targets, on how many people were seen and how many people were funded by CCG.
Now Lewisham CCG have made some definite headway in Lewisham to becoming much more integrated in the way we do things. Of course it’s a journey. So we’re certainly not there yet. Still, Polly was sure a lot of people will have experienced a number of different frustrations around how the system’s working. She feels we are becoming a more integrated health and social care system. Where we are working much more closely with our sector providers. It’s not just the big players e.g. (SL&M), Lewisham CCG is also connecting into our community organizations and age groups do remain relatively distinct. Often the way we do things will mirror that which isn’t always appropriate until the impacts of concurrent issues are understood. So we do have a clearer idea of how different conditions work with each other, but they are still seen often as separate conditions.
At Lewisham CCG they are certainly moving towards a focus on improving outcomes, but they do still have quite a heavy target focus. Those targets are becoming more appropriate as Lewisham CCG move forward. What they are heading towards is a future system where health and social care workers one, and Lewisham CCG are focused on the individual rather than on our kind of organizational boundaries, let’s say, Lewisham CCG want to move between statutory and voluntary services. So between the NHS Trust’s and then any services working in community to be visible, Lewisham CCG don’t necessarily want people to feel they’re being handed off to different places all the time. And they want people to have their personalised journey where movements between that journey feels very seamless. They also want to move to an all age approach where the CCG see the individual as experiencing certain things throughout their lifetime.
So this is also moving beyond comorbidity, not just recognizing people’s potential health issues, but understanding wellness, and looking at their life, and how the CCG can ensure that the way of living and that the way people around them, treat them and work with them ensures optimum wellness, rather than just the absence of ill health, which is one of Polly’s key findings on commissioning and delivery. So this is the way that the CCG design and make services happen. Lewisham CCG deliver those services to people where it is outcomes based and focused. So we want to move away from numbers of people, and move towards the difference we make to people. So that’s the kind of very much that future system Lewisham CCG is working towards. Polly admits she has one very small part to play in a really huge system. And, in essence, this is kind of where she sits in and amongst everything else. Her area is primarily adults and older adults. So she continues to do look at these two areas, predominantly for herself and her team.
Carla Fourie – SL&M director of social care presents
Carla started off talking a bit about herself and when she was appointed in February this 2021, although some people will say that they sure they saw her prior prior to this year and that’s true. She started on secondment with the trust last year literally just a few weeks before the initial lockdown. Eventually the role was made permanent, and she applied for it. She was then formally appointed in a full time role in February this year. Carla looked at putting the slides together and thinking about how she could describe what her role is at the trust, she decided, looking at kind of the role to group it into four key categories. As the most senior social worker in the trust, she works closely with NHS trust board and she works closely with SL&M senior managers, to bring a social work perspective, to the NHS trust. So when we look at our multi professionals within the trust, we’ve got our doctors or nurses and OTS, etc.
In the end Carla’s role is to bring the social worker perspective at a the senior level, she has also the responsibility to work across the trust with the different local authorities, and to ensure that SL&M avoids working in silos, so there is partnership working, and to ensure that the Social Work offer is provided to people with mental health needs, and to help people become in terms of prevention. Her other role is also that trust wide responsibility for safeguarding so the heads of adult and children’s safeguarding reports to her including the areas for domestic violence and abuse, prevention agenda. She also has a trust wide responsibility for the mental health laws that include areas such as mental health capacity, Human Rights Act, etc. In terms of just tying back to the social work, leadership role, apart from working closely with a board, she also has the responsibility to ensure that our social work workforce, social workers that’s directly employed by the trust, are also professionally well supported.
Carla spoke in terms of support to carers and families, where she thought, were important just to highlight again, on a slide where the work at that the trust is doing overall, in terms of manpower strategy, and that’s very much also founded on the triangle of care, where SL&M sees the carer very much as a partner in the care that SL&M provide. There’s a lot of information that SL&M has developed as a trust and under the leadership of Gabriel Richards, who leads strategically on the carer’s agenda. SL&M has got a carer’s charter that is highlighted. SL&M also provides information in their families and carers Handbook, and also information leaflets, posters shown in the blog regarding carers rights under the care rights, writing, carers assessment. SL&M also has information about confidentiality and sharing of information.
SL&M also provide information to nearest relative where we have useful nearest relative leaflets as well on what is provided to carers. One of SL&Ms duties is to try To ensure that ‘cared for’s relatives are informed and consulted with, particularly when there was a Mental Health Act assessment under Section two of the mental health act. The approved mental health professional has a duty to inform the nearest relative under Section three, where the relative has the power to object to someone being detained to a loved one being detained under the Mental Health Act. The nearest relative can also ask for an IMHA, which is an independent mental health advocate to see the patient and the nearest relative can request a mental health assessment, which she thinks sometimes nearest relatives not everyone is aware of that in certain circumstances where it’s been really difficult or challenging to access for whatever reason. So whilst the local authority is to consider the assessment under the Mental Health Act, or the rights and powers of a nearest relative. The nearest relative can write to the associate hospital managers to request for discharge. Sometimes that’s out here too, but in circumstances where they’re responsible clinician disagrees from a clinical point of view, they can roll that request up to the hospital managers who will review that decision as well.
An nearest relative can also appeal to mental health health tribunal, and they’ll set up some circumstances where nearest relative feel that they are not able to take on this role, because it does have a lot of power and responsibility with it. And sometimes some families feel that if someone that’s been identified as a narrows relative that may impact on relationships with their loved one.
This concludes our Lewisham MH carers update for July 2021
Welcome to my latest blog. As a reminder my blog posts focus on mental health carers, what I mean about that is highlighting the caring experiences of those caring for someone with mental ill health or mental health needs. This latest blog post is about community, because when all is said and done for health and social care, it is how the outcomes impact the community.
Some would say to test good quality wellbeing and a caring community, you can literally pick an area in town and stand there to observe. If you see run down apartments, no one talking to each other, anti-social behaviour, lots of noise and people seeming unwell, then this is a prime example of a community in trouble. When we notice such things, it does not take long to think to ourselves who is responsible for all of this?
I am not saying that all communities are like this, but it is worthwhile to experience what I am mentioning. Of course don’t do this at night especially if the community is known for trouble. Perhaps you might be thinking to yourself, why is Matthew raising this in his blogsite? What has all this got to do with caring?
Well as you can see by my blog title “A community that cares is a good one”. The thing I am trying to point out is because we focus on caring being a personal and private experience. We make the mistake that caring only exists in small confined spaces. We also tend to think that caring can only be applied to those who are unwell and once that person has recovered, then caring can stop. This again does not take into context the importance of caring.
Caring in itself can be applied to so many things, not just the person in themselves, but to caring about the environment, caring about ourselves as in our own wellbeing, caring for the importance of education and caring for community. Make no mistake I am not saying to care about everything, since we do not care for racism, isolation, blaming others or being a general nuisance to others. It is what we care for that counts.
I am fully aware that caring for others, especially those close to us is not a forgone conclusion, since there are many challenges that needs to be worked upon, especially with the new Health and Care Bill 2021 (see my online carers newsletter for more detail). I urge those who are caring, carer reps and the general public to take interest in such bills because it will affect us all.
Going back to the idea of caring in itself, we must take note that a caring community cherishes the importance of not only strengthening caring for others but in caring overall, where a society brings caring about those close to us towards caring for the good of all of us. This is not a simple tasks and almost seems like a utopia because we all have different aims and agendas and I expect those to clash as people do not often see eye to eye, but not all communities are alike, if we find a bad community, then it cannot be the case ALL communities are bad as some are better off, we cannot also think that it is just down to money and resources, because there are people out there working very hard to bring out the best in their own communities.
What is wrong in wanting to live in a community that will reduce isolation, improve health and wellbeing, easier access to social care, less noise, pollution and anti-social behaviour? All these wants and desires being out the best in ourselves and makes us happier in the long run, but we need to understand this cannot be done without the emphasis on care or our mental wellbeing is at risk.
Welcome to a brief update of my BAME carers forum for June. The BAME carers forum is an online forum aimed at those who care for someone suffering mental illness, except the forum covers ethnic experiences regarding caring along with discussions on how serious mental illness affects minorities and diverse communities.
Hello fellow unpaid carers. This blog site is geared towards those who support or look after someone suffering mental ill health. I run a number of carer-led expert by experience forums, which focus on unpaid carers regarding engagement from services. Most forums tend to have speakers to engage members regarding mental health system changes or discussing carer awareness.
For the South West London carers forum the following speakers were
NHS South West London CCG – Understanding health Commissioning for carers Dolly Sen – Mental Health Patient/Carer champion Matthew Mckenzie (myself) – The importance of carer peer support
As you might be aware, clinical commissioning groups are merging in their own region as part of NHS England’s long term plan, because my group covers a large area, it made sense for the comissioners to speak to carers from different boroughs in South West London.
South West London CCG presentation
First to speak was Caroline O’Neill who is the Lead Engagement Manager and covers Kingston & Richmond from NHS South West London CCG, we also had John Atherton in attendance who is the Director of Mental Health Transformation for SW London CCG.
John started off the conversation on what the plans are for the rest of the year and going forward. John explained how the 6 CCGs formed in five commissioning groups in South west London. They are responsible for planning, commissioning and buying most of the NHS services in the south west london area. That means hospital care, GP surgeries, rehabilitation clinics, mental health support, learning disabilities and many others.
The CCGs have a healthcare budgets of over £2.3 billion, although carers who attended the June’s meeting were interested in the CCGs mental health pathways and how they were going to include families and carers.
John explained the importance of health checks as those with mental ill health often struggle to get physical health checks and support. John mentioned what happened in the past is people were encouraged by their GP go get a physical health check each year. It is important the CCGs continue to push this forward because there are some service users who had not had a good experience in the past, or they don’t believe in health issues, so they are encouraging people to check at their practice.
A carer reminded the CCG representatives about how difficult it is for people have mental health difficulties to travel especially using public transport. They wondered how this will affect people accessing mental and physical health services for check ups.
I also asked a question to the CCGs regarding is there a simple view of the commissioning structure? Because we have got CCGs doing stuff in 6 boroughs, and then you’ve got merged CCG? So how do people sort of feed into each other on what is going on? The representatives spoke about their governing body and who is on it.
Another carer was concerned about those with learning difficulties with poor health accessing recovery colleges and wondered what the South West London commissioners were going to do about it.
The representatives were pleased to hear SW London and St Georges were promoting the carers forum, but the CCGs also wanted to include our group on developments of mental health services, as the group stressed the carers should be consulted and involved when it comes to service provision. All too often CCGs struggle to get a good number of carers interested in what they do. It could be an added benefit that carers poke their noses into what is being comissioned and why. This is because carers have a vested interest in the health of who they care for, plus carers do actually use some CCG services which could be Increasing Access to Psychological Therapies. A carer member of the group was concerned about the number of carers not being identified and referred to carer services and groups.
An interesting point of the discussion was finding out who were the mental health leads from each of the 6 boroughs, although there is a lot of work needed in developing primary care networks, because some members feel some GP surgeries could learn a lot from other GP practicies.
Dolly Sen presents
It was requested by carer members for Dolly Sen to talk with us at the forum. Dolly Sen is a service user survivor and a carer and has been fighting 20 years for human rights. Dolly mentioned that over the years while trying to keep mentally well, she has been using energies to focus on art, film, performance and even talking about her experiences at other events.
A large part of Dolly’s activism is around the treatment of mental health users, especially around the problems with benefit payments or DWP. She is quite busy working to improve the mental health system in another area where she has moved to. Dolly admitts there are times when nothing can be done on someone’s health and situation, she feels sometimes it is best to be a witness.
A number of questions from members at the forum were interested in how their mental health trust is working to involve more carers in their involvement register. They queried with Dolly about involvement and activism.