By Matthew McKenzie, Facilitator, National Ethnic Mental Health Carer Forum
Introduction: A Forum that Connects and Challenges
As the facilitator of the National Ethnic Mental Health Carer Forum, I never take for granted how special these sessions are. Each month, carers, professionals, and researchers from all over the UK log in to share knowledge, raise awareness, and push for change in how mental health services understand and support ethnic minority communities.
Our October 2025 session was a powerful one. Falling on the last day of Black History Month, it brought together crucial themes on race equality, co-production, research, and carer visibility.
We heard from two key areas shaping mental health equity right now:
The OSMOSIS Project, led by Dr. Jacqueline Sin and Sharon Galliford, focusing on developing social care-based support for carers of people with psychosis.
The Patient and Carer Race Equality Framework (PCREF), presented by Aboobaker Bhana, Equality and Involvement Manager for South West Yorkshire Partnership NHS Foundation Trust.
Caring for someone with long-term mental illness is a profound act of love and responsibility, just as i cared for my mother, but it is also fraught with emotional complexities, especially within culturally tight-knit communities. The experience of unpaid carers, those who provide care without financial compensation, can be shaped by powerful cultural expectations, traditions, and social pressures. These factors often lead to hidden challenges such as guilt and shame, which can create barriers to seeking help and support.
This blog post which is a transcript of my video explores the intricate dynamics of care guilt and shame, drawing on my insights as facilitator of the National Ethnic Mental Health Care Forum.
While the focus often falls on ethnic minority carers, many of the themes discussed I feel are universal, affecting unpaid carers from all backgrounds. However By examining the cultural ideals, emotional burdens, and systemic challenges faced by carers, we can better understand how to support them and promote positive change in mental health care.
The Role of Culture in Shaping the Carer Experience
Family Duty and Community Honor
In many tight-knit communities, caring for a family member is seen as a moral duty and a source of honor. The expectation is clear: “We look after our own.” This deeply rooted tradition fosters strong family bonds and a sense of belonging. The carer’s role is often defined by values handed down through generations, reinforcing the idea that caring is not just a responsibility but an essential part of one’s identity.
However, these cultural ideals can also create significant challenges. The notion that the “perfect carer never complains or needs help” sets an unrealistic standard, making it difficult for carers to express their struggles or seek support. Weakness is discouraged, and the pressure to cope without showing strain is especially pronounced among men, who may feel compelled to “man up” and avoid displaying vulnerability.
Keeping Illness Within the Family
Another common theme is the tendency to keep issues of ill health, particularly mental illness, within the family or community. This approach is often seen as a way to protect the family’s reputation and maintain social cohesion. Religious and cultural beliefs may further reinforce the idea that problems should be addressed privately, sometimes through prayer or spiritual practices, rather than seeking external help.
While these traditions can provide comfort and a sense of solidarity, they can also lead to isolation and prevent carers from accessing the support they need. The fear of gossip, judgment, or being seen as failing in one’s duty can be overwhelming, especially when mental health is stigmatized or misunderstood within the community.
The Emotional Weight of Caring: Guilt and Shame
How Guilt Creeps In
Guilt is a pervasive emotion among carers, particularly when cultural norms dictate that they should be able to handle all challenges alone. The demands of caring often mean missing out on community events, family gatherings, or social obligations. Community leaders or members may notice these absences and interpret them as letting the community down, adding to the carer’s sense of guilt.
This guilt can manifest in several ways:
Resentment and Frustration: Carers may feel frustrated with themselves or the person they are caring for, leading to emotional strain and potential conflict.
Personal Guilt: The belief that needing a break or personal time is selfish can prevent carers from prioritizing their own well-being, even when burnout is imminent.
Fear of Judgment: In large families or communities, the expectation to manage alone can be overwhelming. Carers may worry about being judged or seen as failing in their role.
The Catch-22 of Self-Care
The need for personal time and self-care is undeniable, yet carers often feel trapped in a catch-22. Taking time for themselves is viewed as selfish, but neglecting their own needs can have detrimental effects on their mental and physical health. The pressure to uphold cultural ideals and avoid showing weakness makes it difficult to break this cycle.
In some communities, there may not even be a word for “carer”—it is simply assumed that family members will step in as needed. This lack of recognition further compounds the challenges, as carers struggle to articulate their needs or seek validation for their efforts.
The Impact of Shame and Stigma
Saving Face and Avoiding Help
Shame is closely linked to guilt, and both emotions can prevent carers from reaching out for help. The desire to “save face” is strong in many communities, where reputation and social standing are highly valued. Admitting to struggles or accepting support may be seen as a sign of weakness or failure, leading carers to reject offers of assistance from mental health services or outreach programs.
Internalized comments such as “this is your duty,” “you must put up a front,” or “we don’t put family in care” reinforce the belief that seeking help is unacceptable. The fear of gossip and misunderstanding is real, especially in communities where mental health is poorly understood or lacks a cultural vocabulary.
Religious and Cultural Barriers
Religious identity can also play a role in shaping attitudes toward mental health and caring. In some faith-based communities, there may be little space for open discussion about mental illness, and spiritual solutions may be favored over professional support. This can create additional barriers for carers, who may feel unsupported or misunderstood by both their community and the wider mental health system.
Systemic Challenges: Inequalities in Mental Health Care
The Patient Care Race Equality Framework (PCREF)
Recognizing the unique challenges faced by minority carers, NHS England has developed the Patient Care Race Equality Framework (PCREF). These set of policies aims to tackle inequalities in mental health care, particularly for ethnic minority groups. The framework emphasizes the importance of breaking down guilt and shame, promoting better outcomes for minority communities, and ensuring that carers’ voices are central to service design and decision-making.
However, systemic barriers persist. Minority carers may be reluctant to engage with mental health services due to fears of poor outcomes, discrimination, or further isolation. The double tragedy is that those who need support the most are often the least likely to receive it, as both community and systemic factors conspire to keep them from seeking help.
The Importance of Carers’ Voices
A key focus of the National Ethnic Mental Health Care Forum is to ensure that carers’ voices are heard and valued. Too often, the emphasis is placed solely on patients or those with lived experience, overlooking the vital role that families and carers play. Guilt and shame can stop carers from engaging with services, making it essential for mental health systems to recognize and address cultural barriers.
Breaking the Cycle: Towards Better Support and Outcomes
Engaging with Communities
To break the cycle of guilt and shame, it is crucial to engage directly with communities. This means attending religious and cultural gatherings, listening to minority carers and patients, and understanding the specific struggles they face. Education is key!! both for carers and for mental health professionals. Training staff to appreciate community values and avoid assumptions about disengaged carers can help foster trust and collaboration.
Creating Safe, Non-Judgmental Spaces
Safe spaces where carers feel invited and heard are essential. These settings should be non-judgmental and designed to encourage open dialogue. Just like my Ethnic carer forum. Co-production, where patients and carers are involved in designing and delivering services and can help ensure that support is tailored to the needs of diverse communities.
Promoting Positive Role Models
Just as I mentioned when I spoke at the North East London NHS PCREF event, I feel that Role models play a powerful role in challenging stigma and inspiring change. Mental health trusts and systems should promote positive examples of carers who have reached out for help and benefited from support. Sharing stories and experiences can help others see that seeking help is not a weakness, but a strength.
Self-Care as Strength
Promoting self-care as a strength, rather than a weakness, is vital. Carers need to recognize that it is okay to ask for help and take time for themselves. Engaging with community leaders and faith networks can help change attitudes and reduce stigma, using trusted voices to advocate for better understanding and support.
The Path Forward: Building Inclusive Mental Health Services
Co-Production and Service Design
Including carers in service design and decision-making is essential for building inclusive mental health services. By putting carers at the center of policy and practice, systems can better address the unique challenges they face and promote positive outcomes for all.
Education and Awareness
Ongoing education and awareness-raising are critical. Carers, communities, and professionals must work together to challenge stigma, promote understanding, and create environments where everyone feels supported.
The Power of Conversation
Ultimately, breaking the cycle of care guilt and shame requires open conversation and a willingness to learn from each other. By sharing experiences, listening to diverse voices, and fostering empathy, we can build stronger, more inclusive communities and mental health systems.
Conclusion
Care guilt and shame are complex, deeply rooted issues that affect unpaid carers across culturally tight-knit communities. The emotional weight of caring, compounded by cultural expectations and systemic barriers, can lead to isolation, burnout, and reluctance to seek help. Addressing these challenges requires a multifaceted approach engaging with communities, promoting positive role models, creating safe spaces, and ensuring carers’ voices are central to service design.
By working together to challenge stigma and promote understanding, we can support carers in their vital role and build mental health services that truly meet the needs of all. The journey is ongoing, but with awareness, education, and compassion, positive change is possible.
Caring for someone with mental illness? Check out our Ethnic carer forum. Dates shown below.
Been a while since I did a carer forum update, but felt I should do one otherwise I would be distracted by something else. Here is the brief update of my ethnic mental health carer forum for September 2022. The forum is aimed at those from an ethnic background caring for someone with mental illness.
The speakers for September are listed below
Madeleine Oakley on her Kings College London carers peer research group
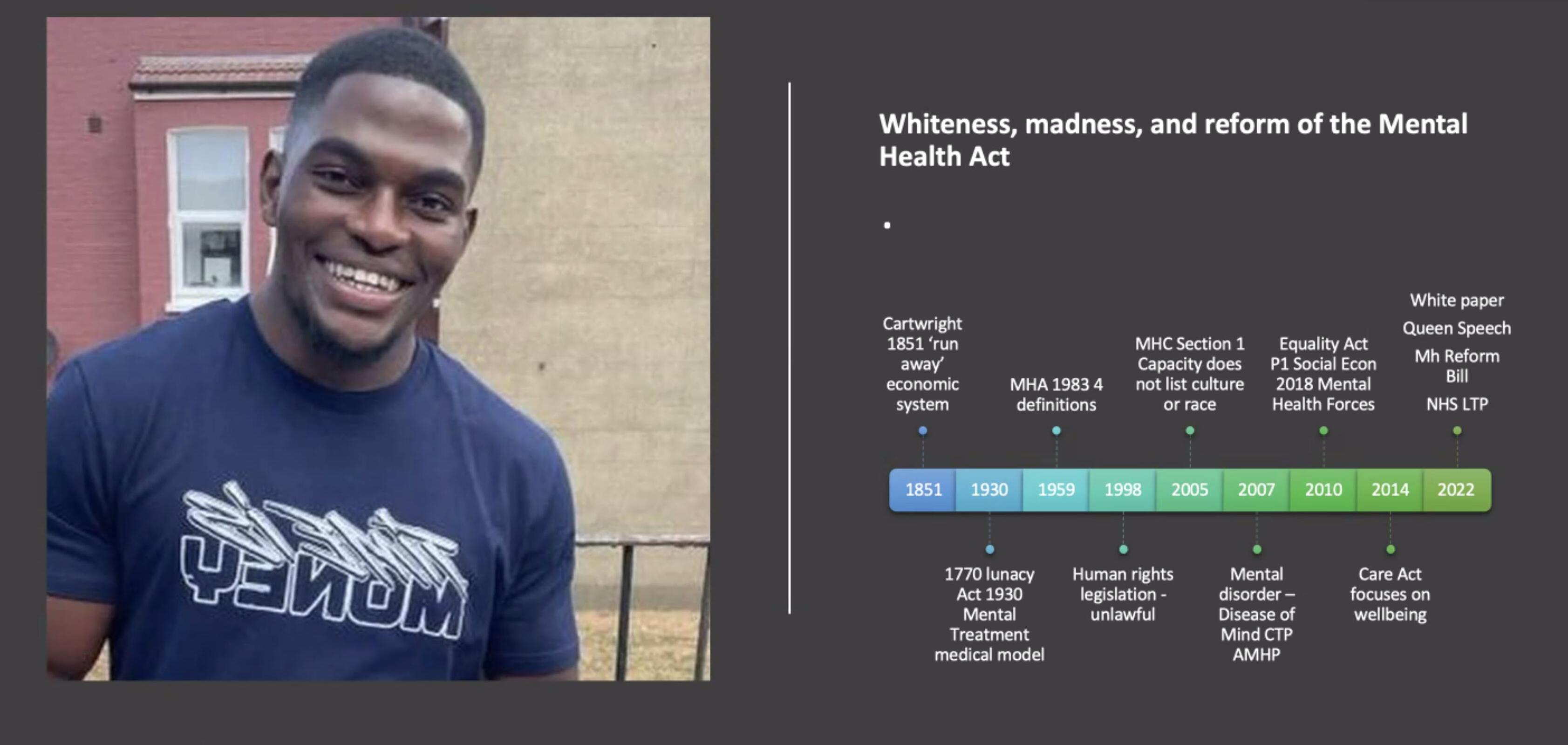
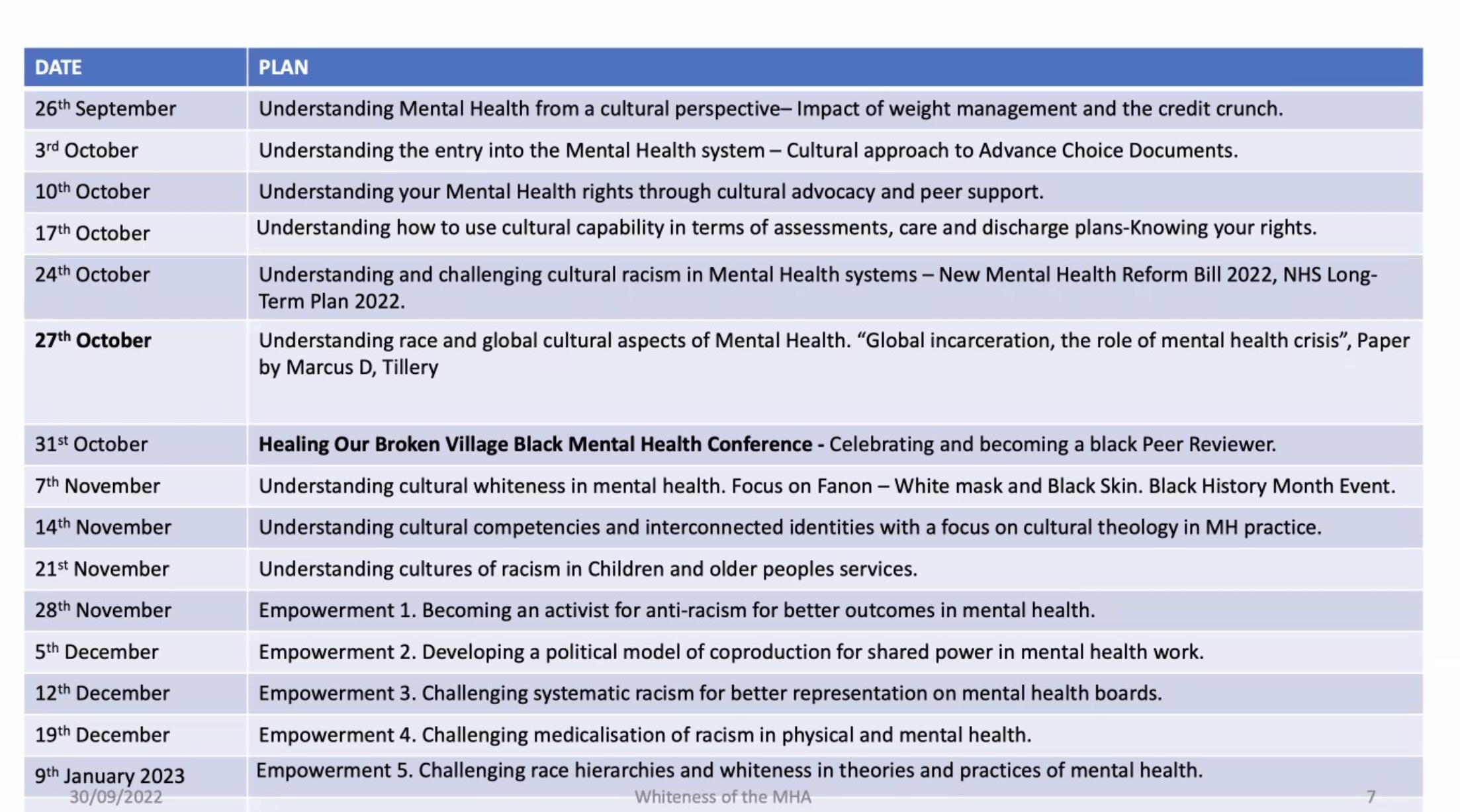
Colin King presenting on the Lancet report – Whiteness, madness, and reform of the Mental Health Act
Louise Goff on the Kings college London Health promotion Heal-D: a culturally-tailored diabetes self-management programme for adults of African & Caribbean heritage
Madeleine Oakley presents on her carers peer group
Madeleine from Kings College London has been using her skills as a psychotherapist to give people space to talk about their experiences, she has found that carers really appreciate connecting with each other. Madeleine also has the lived experience of caring for somebody with autism. Her groups have been for people who are caring for a family member who has got autism. So she started with autism and eating disorders, because there was a lot of research going on about that at the South London and Maudsley.
She is now doing an autism and psychosis carer group. Which is once every Friday morning, a month. Madeleine stated that unfortunately it does clash with my group one Friday morning, but basically, the next one is on the 23rd of October. The latest one has already started in September. Madeleine hopes members of my group can help spread the message.
Madeleine has also been interviewing family carers of people with autism and psychosis. So they’ve got both conditions that people are looking after. She is trying to explore the experiences of carers. How did they get the assessments? How did they get the treatments, how was being a carer affecting their lives?
Questions from carers
I started off asking “Is this group indefinite or is it just runs for a set period?”
Madeleine responded
The she wishes it was indefinitely. They are always looking for more funding, but it’s only until the end of March. So it’s a short thing as it is basically part of her PhD. But at the same time, she is applying for funding to sort of make the carers group permanent because the sad thing is all the work that she has done with carers since 2019, when she finishes her PhD, then where is the group going to?
Colin King presenting on Whiteness, madness, and reform of the Mental Health Act
Colin explained that he was sectioned schizophrenia within Maudsley many years ago, but what he was really concerned about was the whiteness within the theoretical and diagnostic framework was leading to historically the over representation of particular groups.
This led Colin to do an analysis looking at the start of something called cartwright 1851, which is the first diagnosis of race, which is when the black person ran away with slavery, they were diagnosed with, with depomania, and if you do the travel on the lunacy Act, at the mental health Act to the white paper Act to the White Paper review, Colin mentioned that we still got an over representation or of communities in the mental health system.
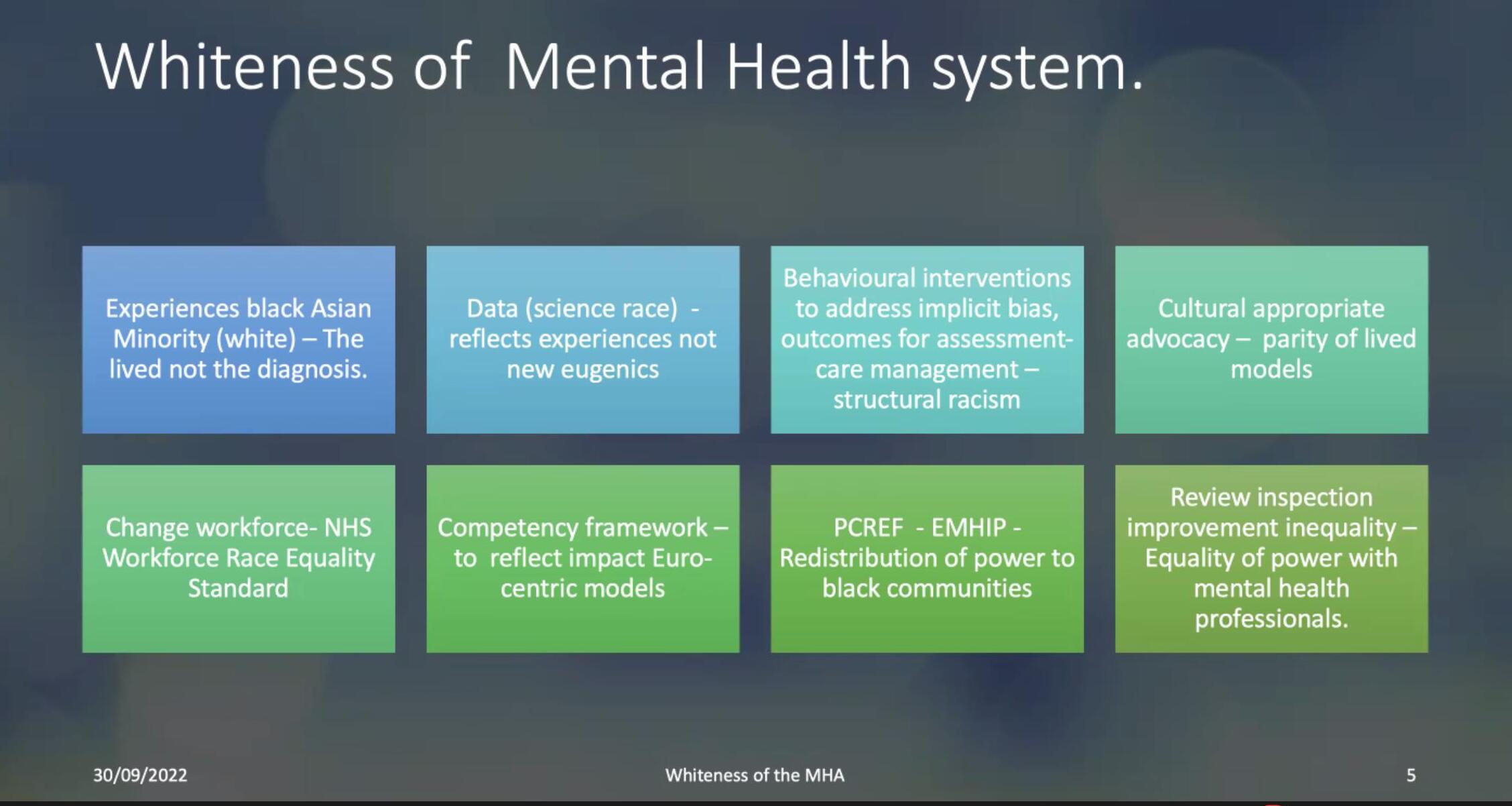
Colin wanted to understand what was whiteness, what why was whiteness, such a pervasive, intrusive and powerful intervention is in terms over representation.
Colin stated that some of it can be located in the history of theories of psychology and psychiatry that perpetuate eugenic theories about the black body and the black mind. And these theories emerged in the period of slavery, when there was a perpetuation of a division between what was whiteness as superior, and blackness as inferior. And these are some of the writers from Cartwright perpetuate his idea. Colin mentioned that even Henry Maudsley who ran the Maudsley had perpetual eugenic ideas about race.
Colin was really concerned about what the outcome this lead into in terms of particular types of whiteness, and the outcomes for diverse communities over the last 400 years, but particularly where we are with the activism for the PCREF (Patient Carer Race Equality Framework) and other campaigning groups.
So Colin began to analyze two diagnostic frameworks in terms of why they were leading to these race diverse outcomes, DSM-5, and also ICD-10. Colin mentions a book where whiteness contributes to the legalization of race as a diagnostic framework.
This leads to a problems with ideas that black people are much more naturally disordered, and what’s more psychotic. Colin felt that as activists, instead of trying to change the diagnostic framework, we should try to improve the system rather than dismantle it. THe main concern he was looking at, was community treatment orders.
And the data has continued to show that a particular groups are over represented are usually black Caribbean men, South Asian patients, women, but the biggest concern for him was why is it in 2007, when they introduced something called Community Treatment orders that 92% of them are used in relation to black men. And why is it with restraints show 75% of them have been used in relation to men. So Colin wrote a paper and it was really a plea for the abolition of community treatment order which he interpreted as a new type of slavery in mental health care and needed to be changed.
Colin spoke about the importance of being an activist, but also allowing lived experienced from the community to be involved in training and raising the importance mental health in the communities. Colin mentioned we all have something to contribute and if MH systems and beyond including schools, housing and communities services do not include minority lived experience then it hurts the community as a whole.
Louise Goff presents on a culturally-tailored diabetes self-management programme for adults of African & Caribbean heritage
Louise started training as a dietitian about 25 years ago, and then she went straight into a research career all focused around type-2 diabetes. This was on how nutrition and food affects diabetes, how it can prevent diabetes, how it can treat diabetes, She has been doing that for about 25 years now. However through her education, she was well aware that rates of diabetes were were significantly higher in people from African and Caribbean backgrounds, as well as in other minority ethnic backgrounds in the UK.
She then became really aware of contradictory messages from her professional colleagues compared to her own family and my social network. The messages that she had from her professional colleagues and network was that, people weren’t showing up for their diabetes appointments, and therefore, they didn’t care about their diabetes. This was particularly common in people of African or Caribbean heritage. And so there was this perception that diabetes wasn’t thought to be serious and wasn’t cared about. Speaking to her friends and family, particularly people who had diabetes, were so fearful of their diabetes, and so worried about their diabetes, and really wanted information about how to improve diabetes, how to avoid diabetes.
So that really led to her wanting to focus her research career more towards understanding that situation and understanding on what is going on in the health system. And what is going on in the communities. She has been using her research platform to try and unpick and work towards trying to improve that situation really. A while back she received some research funding to develop diabetes self management program specifically tailored to the needs of adults from African and Caribbean backgrounds
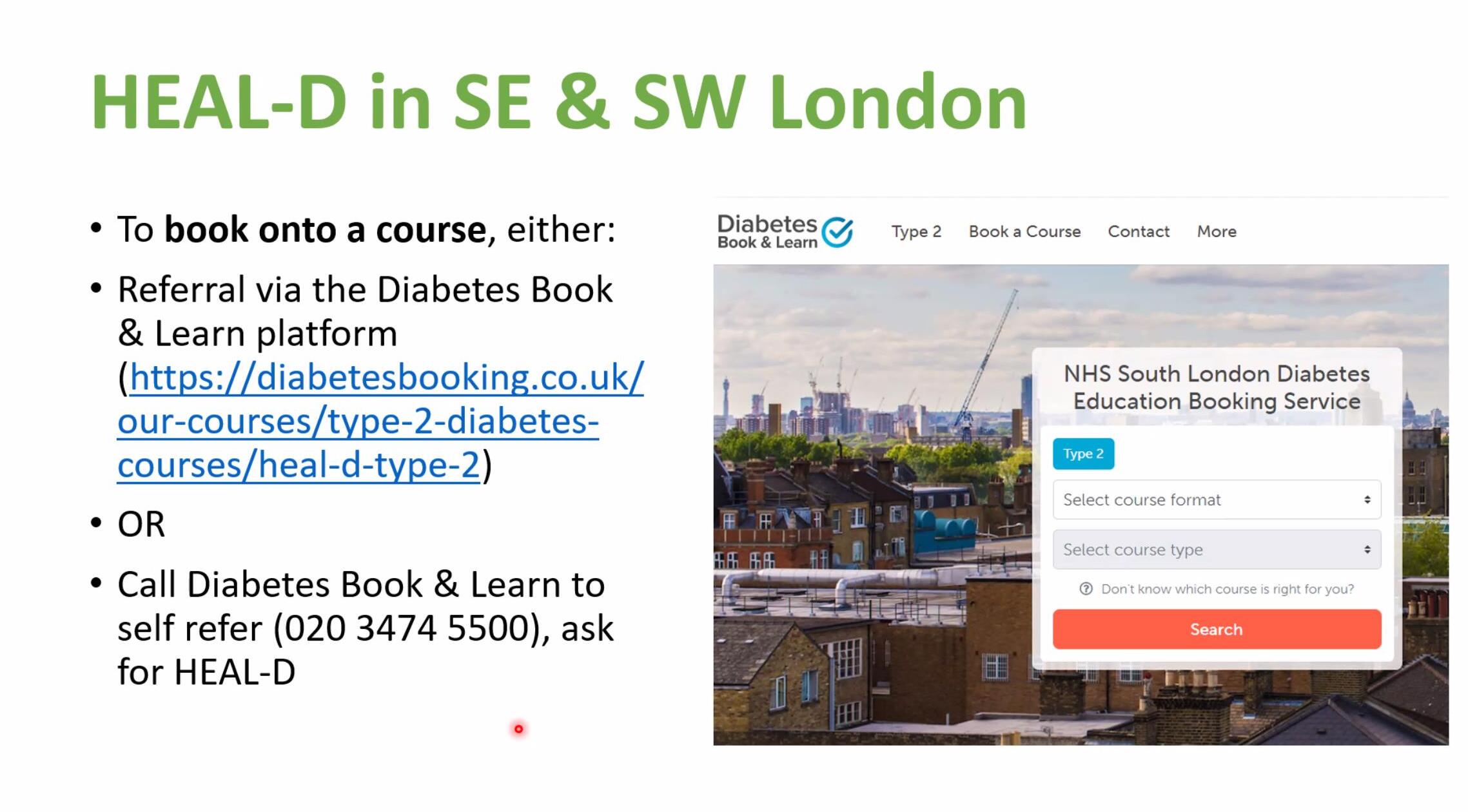
The project has the following skills
• Group-based • 7 sessions of 2 hours – 1-hr educational discussion & 1-hrexercise class • Delivered weekly • Delivered using video conferencing • Dietitian & community facilitators
The program is called healthy eating and active lifestyles for diabetes, or abbreviated down to heal D, but it’s a self management program that’s been developed to help people who are living with type-2 diabetes, to really understand what they need to do in their self management. In terms of diet and physical activity and other lifestyle components to improve the management of diabetes, all the while specifically tailored to African and Caribbean culture.
The program is called healthy eating and active lifestyles for diabetes, or abbreviated down to heal D, but it’s a self management program that’s been developed to help people who are living with type-2 diabetes, to really understand what they need to do in their self management. In terms of diet and physical activity and other lifestyle components to improve the management of diabetes, all the while specifically tailored to African and Caribbean culture.
Louise stated that this is about cultural health beliefs, cultural foods, cultural practices around food and physical activity and body weight. And all of the things that we know about medications and all of the things that we know that are related to diabetes management.
Louise continued she is actually following on from the really important messages that Colin was just sharing with us. when she went about developing this program, she knew that it was the people with the lived experience who were the experts through their lived experience that really needed to lead this project to understand what was needed in a program that would really support people.
So all of this work was done using a sort of community partnership approach, whereby they engaged with our communities, and this was conducted in southeast London.
Welcome to my March 2022 update of our SW London mental health carers forum. The group is a hybrid group of my other forums. Usually my carer forums focus on engagement and updates, but this one sometimes acts as a peer and network group for those caring for someone with mental illness.
Speakers for March 2022
Karen Persaud – SWLSTG – Carers, friends and family involvement coordinator
Gary Baker – Carers Support Worker – Richmond Mind
Antonia Buamah – Patient peer support – EMHIP– Ethnicity and Mental Health Improvement Project.
Karen from South West London & St George Presents
Karen who sometimes attends and engages with our group updated us on carer developments at the local SW London mental health trust. Karen spoke about the new carers peer support worker Zoe Hannah. The new role will be running for one year and should hopefully continue onwards.
The trust is actually really committed to pushing forward the lived experience workforce as part of their overall service delivery. This is where they have four services user peer support workers in posts. SWLSTG are also currently reviewing the trust’s carers strategy, which is quite outdated.
The new strategy will also be reflecting on the need for the trust to do more around supporting carers through their carers recovery journey, because carers go through a recovery alongside supporting loved ones through their own recovery journey. This means it is trying to balancing out wellbeing needs.
The next update for SWLSTG is there new recovery college course, which is being facilitated by Kingston adults education, college. The course has been adapted for wellbeing techniques for carers, families and friends. The course should be running for 10 weeks. Karen also updated briefly on the friends, families and carers group incase new members of our forum are interested in trust involvement.
Last updates from Karen was on the carer awareness training for staff, especially on induction for staff. This would involve carer communication skills plus carer involvement in the planning and discharge.
Gary Baker – Carers Support Worker – Richmond Mindpresents
Gary fed back on how Ricmond Mind works closely with Richmond carers regarding mental health carers. Carers can be self refered or be referred to by another professional. Once they received that referral, Richmond Mind will contact the carer. From there the carer will be given access to support and workshops.
Gary mentioned that quite a few people tend not to like the term carer and tend to prefer being called a client or the person’s relative.
Responses from carer members.
Are services at Richmond could be offered in Merton or Kingston? (quite a few members asked about the services) My question was on engagement from SWLSTG, I wondered if Richmond Mind staff have been invited to meetings. Gary talked at length regarding carer champion meetings. The next question I asked for engagement from community mental health teams. This is where Gary mentioned that there was not enough.
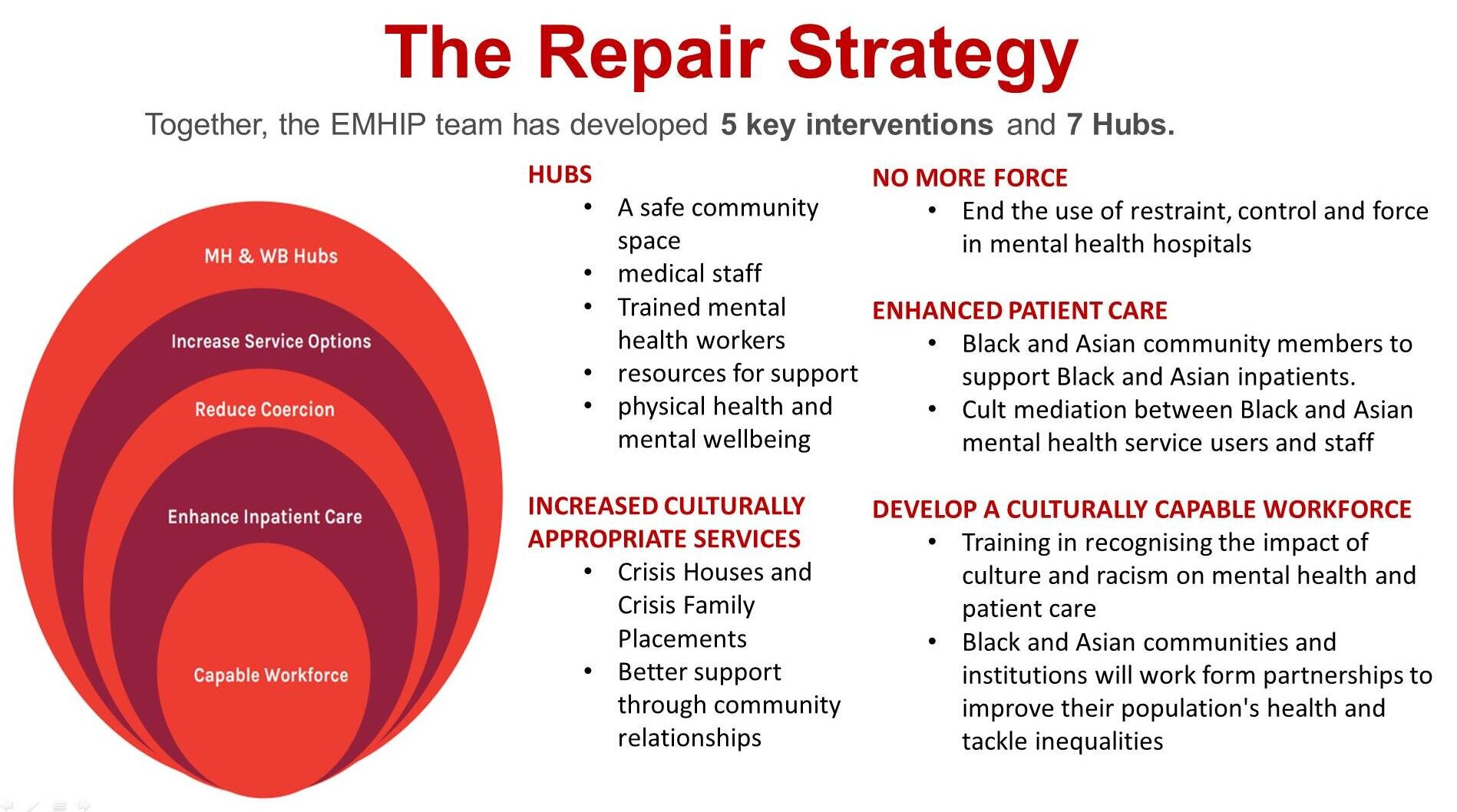
Antonia presents on the Ethnicity and Mental Health Improvement Project (EMHIP)
Antonia talked about how the Ethnicity and Mental Health Improvement Project (EMHIP) is an attempt to reduce inequalities in access, experience and outcome of mental health care in South West London (Wandsworth & Tooting, Battersea locality). It was developed through the leadership and activism of leaders within the African, African Caribbean, and Asian communities.
The EMHIP advocates for a practical, locally based service improvement programme, co-designed with service users and local Black and Asian communities, based on established evidence, building on existing community led, co-produced projects.
In the UK, people from the Black and Asian community are being denied equal and compassionate mental health care.
They more likely to be brought to and kept in without their consent.
They are more likely to access mental health services through the police and criminal justice systems. find themselves unwell and back again, once released, particularly men
be forcibly restrained and given more than the recommended amount of medication.
The fence of mental heath for the Black and Asian community has been broken for several generations and the many promises of repair (partial or full) has not materialised to date.
We have delved deep, hence, our toolkit EMHIP– Ethnicity and Mental Health Improvement Project.
Antonia pointed out that as a community we’ve recognised that our broken fence must be repaired once and for all and have forged collaborations and partnership with many friends
South West London CCG (CCGs are now replaced to Integrated Care Boards) South West London and St. George’s Mental Health NHS Trust Local context of Black and Asian – voluntary, faith and community groups
This can be organized via the non-profit Wandsworth Community Empowerment Network (WCEN)
The Hub offers our guests, visitors and other attendees a communal safe place to sit down, relax and have a conversation in a hospitable environment.
Service/Sessions provided:
¨ Physical Health and Wellbeing checks ¨ Citizen Advice Bureau/Housing First Aid ¨ Pastoral Systemic Therapy ¨ Mental Health and Wellbeing Out-patients type clinics ¨ Explore training or employment opportunities ¨ Promote on-going recovery ¨ Social life wellbeing ¨ Effective “active sign-posting” to the supportive local services or agencies
This was a brief update for my SW London mental health carers peer group. For the month of July SW London NHS will be engaging our group regarding SW London’s mental health strategy. I for one will hope it will include families and carers.
Did you know that I run a monthly online carers newsletter? Although most of my focus is on mental health carers, the newsletter focuses on all unpaid carers. The rest of the carer news focuses on Mental health updates, ethnic mental health news and items relating to NHS and national organisations responsible for health & social care.
mind word cloud gradient blue sky background only
For January update we have the following news items