By Matthew McKenzie – Carer & Chair of the National Ethnic MH carer Forum
The June 2026 National Ethnic Mental Health Carer Forum brought together carers, NHS Trusts, researchers, voluntary organisations and mental health professionals from across England to discuss one shared ambition improving mental health services through genuine co-production with ethnic minority carers.
Matthew reminded delegates that carers develop expertise through lived experience. Supporting a family member with severe mental illness means navigating NHS services, social care, benefits systems and advocacy. These experiences provide knowledge that cannot be learned through textbooks alone.
Opening Presentation
Matthew McKenzie
The Importance of Co-production
Forum Chair Matthew McKenzie opened the meeting by welcoming carers and professionals from across England and reflecting on more than a decade of leading the National Ethnic Mental Health Carer Forum.
He explained how the forum has evolved alongside the NHS Patient and Carer Race Equality Framework (PCREF), providing an increasingly important national platform for ethnic minority carers to influence mental health services.
A recurring theme throughout the presentation was the internationally recognised principle:
“Nothing About Us Without Us.”
He explained that this principle has guided disability rights and patient involvement movements for many years and remains just as relevant today for carers supporting loved ones with serious mental illness. Family carers often spend years navigating mental health services, social care systems and community support, developing valuable knowledge through lived experience that professionals alone cannot acquire. This expertise is especially important for carers from minority ethnic communities who may also encounter cultural misunderstandings, language barriers, discrimination or unequal access to services. Matthew argued that services cannot fully understand these challenges without involving the people who experience them every day. He encouraged carers to recognise that their experiences are not simply personal stories but a form of expertise that should be valued equally alongside professional knowledge when designing, reviewing and improving services.
The presentation concluded with a powerful call for organisations to move beyond consultation towards genuine partnership working. Matthew explained that when co-production is absent, services risk misunderstanding community needs, developing policies that fail to reflect lived experience and missing opportunities to reduce long-standing inequalities. Conversely, meaningful engagement enables carers to become active partners in service improvement, helping organisations build trust with communities, improve cultural responsiveness and design services that are accessible to everyone.

He also highlighted complementary approaches, including the Triangle of Care, Open Dialogue, cultural competence and shared decision-making, all of which reinforce the importance of collaboration between professionals, service users and carers. Matthew ended by encouraging every organisation represented at the forum to ensure that diverse voices are heard throughout the decision-making process, not simply those that are easiest to reach. His closing message resonated throughout the rest of the meeting: meaningful change begins by listening, respecting lived experience and ensuring that carers have a genuine seat at the table whenever mental health services are being designed or improved.
Q&A Highlights
Q: Why is co-production particularly important for ethnic minority carers?
Because carers from minority communities often experience additional barriers including discrimination, cultural misunderstandings and language challenges. Their lived experience helps services recognise issues that routine data alone cannot identify.
Q: What happens when services fail to co-produce?
Participants suggested services become “them and us” organisations where carers feel excluded, policies fail to meet community needs and trust declines.
Bradford District Care NHS Foundation Trust
Bronte Dines-Allen
Bronte Dines-Allen, Reducing Health Inequalities Lead at Bradford District Care NHS Foundation Trust, provided an inspiring overview of the Trust’s journey in implementing the Patient and Carer Race Equality Framework (PCREF). Introducing herself not only as a senior NHS leader but also as someone with lived experience as a family carer supporting her mother with mental ill health, Bronte spoke passionately about the importance of understanding services from both professional and personal perspectives.
She described Bradford as one of the most culturally diverse areas in England, with more than 150 languages spoken across the district and a population representing a wide range of ethnic communities. This rich diversity presents both opportunities and responsibilities for healthcare providers, requiring services to continually adapt, listen and ensure that care is culturally responsive and accessible to everyone. Bronte explained that Bradford’s approach to PCREF has been built around openness and transparency, with the Trust publishing annual progress reports and equality data to demonstrate both achievements and areas where further improvement is needed.
A major focus of Bronte’s presentation was the Trust’s recent “Amplifying Voices” event, which brought together NHS staff, voluntary and community organisations, chaplaincy services, neighbouring NHS Trusts and people with lived experience to discuss health inequalities and mental health care. Rather than concentrating solely on statistics, the event was designed to explore the stories behind the data, recognising that every figure represents a real person, family or community whose experiences deserve to be heard.

Participants shared personal accounts of navigating mental health services, building trust with professionals, overcoming barriers related to culture and language, and the importance of feeling genuinely listened to. Bronte stressed that collecting feedback is only meaningful if organisations demonstrate how that feedback influences future decision-making. One of the most encouraging outcomes of the event was the commitment from senior leaders that the experiences shared would directly inform the Trust’s refreshed organisational strategy, ensuring that health equity and reducing inequalities remain central to future service development.
Looking ahead, Bronte outlined several priorities that will continue to strengthen Bradford’s PCREF programme. These include expanding cultural competency training for staff, increasing awareness of PCREF throughout the organisation, developing educational resources that encourage conversations about race equality, and creating further opportunities for carers to contribute to service improvement.
She acknowledged that the Trust is still early in parts of its journey, particularly in strengthening engagement with carers and improving mechanisms for gathering feedback, but emphasised that genuine progress comes through honesty, collaboration and a willingness to learn from others. During the discussion that followed, delegates praised Bradford’s transparent approach and shared examples of similar work taking place across other NHS Trusts, reinforcing one of the key messages of the forum that improving mental health services is a shared national endeavour. Bronte concluded by reiterating that sustainable change depends upon building trusting relationships with communities, valuing lived experience as expertise and ensuring that carers remain active partners in shaping the future of mental health care.
Q&A Highlights
Q: What specific work is being undertaken with older adults?
Bronte acknowledged that Bradford is still developing this area and welcomed suggestions from carers and other Trusts, emphasising the importance of learning nationally.
Q: How is co-production influencing your work?
The event itself was co-designed with voluntary sector partners and accountability groups, ensuring community voices shaped both the programme and future priorities.
Q: How do you collect meaningful feedback?
Bradford continues improving its feedback systems following technical challenges and is exploring better ways of gathering and acting on carers’ experiences.
Research Presentation
Dr Meghana Kamble
Families of Children with Disabilities: Perspectives from South Asia
Dr M. Kamble from the University of East Anglia presented an insightful overview of an international research project exploring the experiences of South Asian families caring for children and adults with intellectual and developmental disabilities.
The study spans the United Kingdom, India, Sri Lanka and the United States, bringing together the voices of parents, siblings, carers, people with disabilities and professionals to better understand the challenges faced by families across different cultural settings. Dr Kamble explained that despite increasing awareness of health inequalities, the experiences of many ethnic minority families remain underrepresented in both research and service development. The project seeks to address this gap by examining not only access to services but also how cultural beliefs, family dynamics and lived experience influence the support that families receive. Underpinning the research is the principle of family-centred care, recognising that supporting one individual also means understanding and supporting the wider family network that cares for them.
Drawing on early findings from interviews, focus groups and surveys, Dr Kamble highlighted several recurring themes that resonated strongly with delegates at the forum. Families consistently reported difficulties accessing culturally appropriate services, navigating complex health and social care systems, and finding professionals who understood the realities of their lived experience. Stigma, social isolation and language barriers were frequently identified as obstacles that prevented families from seeking support at an early stage.
One particularly interesting finding challenged common assumptions about South Asian communities. While it is often believed that extended family networks naturally provide substantial support, many participants described relying far more heavily on peer support groups, community organisations and voluntary sector services than on relatives. Dr Kamble also observed that outside Europe many people do not identify themselves as “carers” in the formal sense; instead, they simply see themselves as sons, daughters, brothers or sisters fulfilling their family responsibilities. This distinction has important implications for how services identify and engage people who may be eligible for support but never recognise themselves under the label of “carer.”
The discussion following the presentation explored how research findings can influence future policy and practice. Delegates highlighted the need for clearer information about carers’ rights, improved communication with communities and greater transparency from statutory services about the support that is available. Several participants emphasised that trust can only be built when organisations consistently involve communities in decision-making and demonstrate that lived experience genuinely shapes service improvements. Dr Kamble agreed that while systems and policies are important, individual professionals often make the greatest difference by taking the time to guide families through complex services and helping them understand their rights. Looking ahead, the research team plans to share its findings through publications, webinars, community engagement events and partnerships with organisations across the UK and internationally. The presentation served as a powerful reminder that reducing inequalities requires not only better research but also culturally responsive services that recognise and value the diverse experiences of families from every community.
Q&A Highlights
Q: How will the research findings be shared?
The project plans to publish papers, webinars, newsletters and community engagement events, with researchers keen to work alongside carers in disseminating findings.
Q: How can services better reach ethnic minority carers?
Participants emphasised:
- clearer information about rights
- better community engagement
- trusted local organisations
- simpler access to support
- transparent communication.
Q: Should organisations rethink the word “carer”?
Yes.
Several delegates suggested that many people never identify with the label “carer,” meaning they may never seek available support. Researchers agreed this requires further exploration.
Nottinghamshire Healthcare NHS Foundation Trust
Ashley Bertie
Accelerating PCREF Implementation
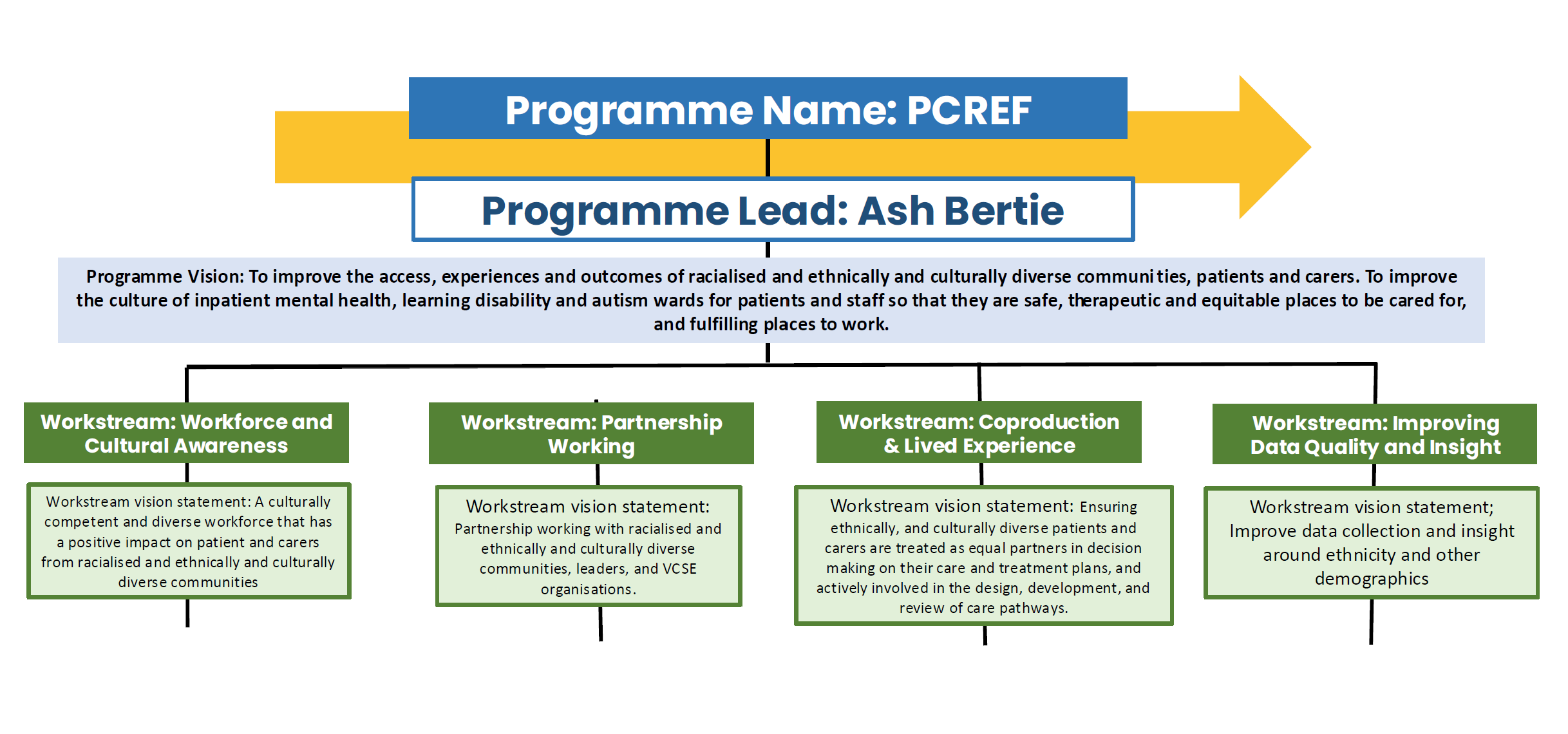
Ashley Bertie, Associate Director for Participation, Co-production and Patient Care Experience at Nottinghamshire Healthcare NHS Foundation Trust, provided an informative update on the Trust’s progress in implementing the Patient and Carer Race Equality Framework (PCREF). Ashley explained that although the Trust recognises there is still much work to do, PCREF has become a strategic priority across the organisation and is helping to drive meaningful cultural change.
Since taking up his role, one of his key objectives has been to accelerate implementation by embedding race equality, co-production and lived experience into the Trust’s everyday work. He described how the organisation has established a comprehensive governance structure, including a PCREF Steering Group chaired by the Chief Nurse, supported by specialist groups focusing on health inequalities, workforce development and lived experience. Importantly, carers, patients, Equality, Diversity and Inclusion (EDI) ambassadors and voluntary sector representatives are all involved in shaping the Trust’s work, demonstrating a commitment to partnership rather than top-down decision making.
Ashley emphasised that improving mental health services cannot be achieved by the NHS working in isolation. A significant part of Nottinghamshire Healthcare’s strategy involves developing strong partnerships with voluntary and community organisations, local authorities, Integrated Care Boards and other NHS Trusts.
He explained that many people from ethnic minority communities have longstanding relationships with trusted community organisations but may be reluctant to engage directly with statutory services due to previous negative experiences or cultural barriers. As a result, the Trust is increasingly taking its engagement activities into local communities, holding events in community centres, places of worship and neighbourhood venues where people already feel comfortable and supported. Alongside this community-based approach, the Trust is investing in cultural capability training for staff, improving transparency through publicly available equality dashboards and developing a new Lived Experience Advisory Group to ensure that carers and service users play a central role in monitoring progress and influencing future service improvements.
Looking ahead, Ashley outlined an ambitious programme of work designed to embed PCREF throughout the organisation over the coming years. Funding secured through NHS England will support a wide range of initiatives, including cultural awareness workshops, staff development programmes, community capacity-building projects and expanded opportunities for people with lived experience to influence recruitment, service design and quality improvement.
One of the Trust’s key ambitions is to ensure that at least 80 per cent of its workforce receives training on the principles of PCREF, helping staff to better understand health inequalities and deliver more culturally responsive care. Throughout his presentation, Ashley reinforced the importance of meeting communities where they are, listening carefully to lived experience and building relationships based on trust rather than assumptions. His presentation reflected the wider theme of the forum: that lasting improvements in mental health services depend upon genuine collaboration between professionals, carers, service users and the communities they serve.
Q&A Highlights
Q: Why are community partnerships so important?
Ashley explained that local organisations often have trusted relationships with communities that NHS services may not yet possess.
Q: How will Nottinghamshire involve carers?
Through a new Lived Experience Advisory Group, strengthened co-production arrangements and wider involvement in service design, recruitment and evaluation.
King’s College London
Ida Doherty
Supporting Ethnic Carers in South West London
Although this presentation formed part of the meeting agenda, discussion focused on ongoing work supporting ethnic carers across South West London through research and partnership working. The emphasis was on better understanding carers’ experiences and ensuring that future services are informed directly by those experiences.

More on her talk will be for the next forum due to time.
Looking Ahead
The National Ethnic Mental Health Carer Forum continues to provide a valuable national platform where carers, researchers, NHS Trusts and community organisations can learn from one another.
The discussions demonstrated that progress is being made through PCREF, research and community partnerships, but also recognised that significant challenges remain.
Moving forward, success will depend on maintaining the principles that underpinned every presentation:
- listening before acting
- valuing lived experience
- strengthening trust
- improving cultural responsiveness
- ensuring carers remain genuine partners in shaping mental health services.
The forum closed with networking and an invitation for organisations across England to continue sharing good practice, supporting one another and working collectively to reduce inequalities in mental health care.
Date of Next forum – 31st of July 10:30 am