By Matthew McKenzie – Chair, National Ethnic Mental Health Carers Forum
The July meeting welcomed unpaid carers, NHS organisations, universities, researchers and community groups from across England to discuss how mental health services can become more inclusive for carers from ethnic communities.
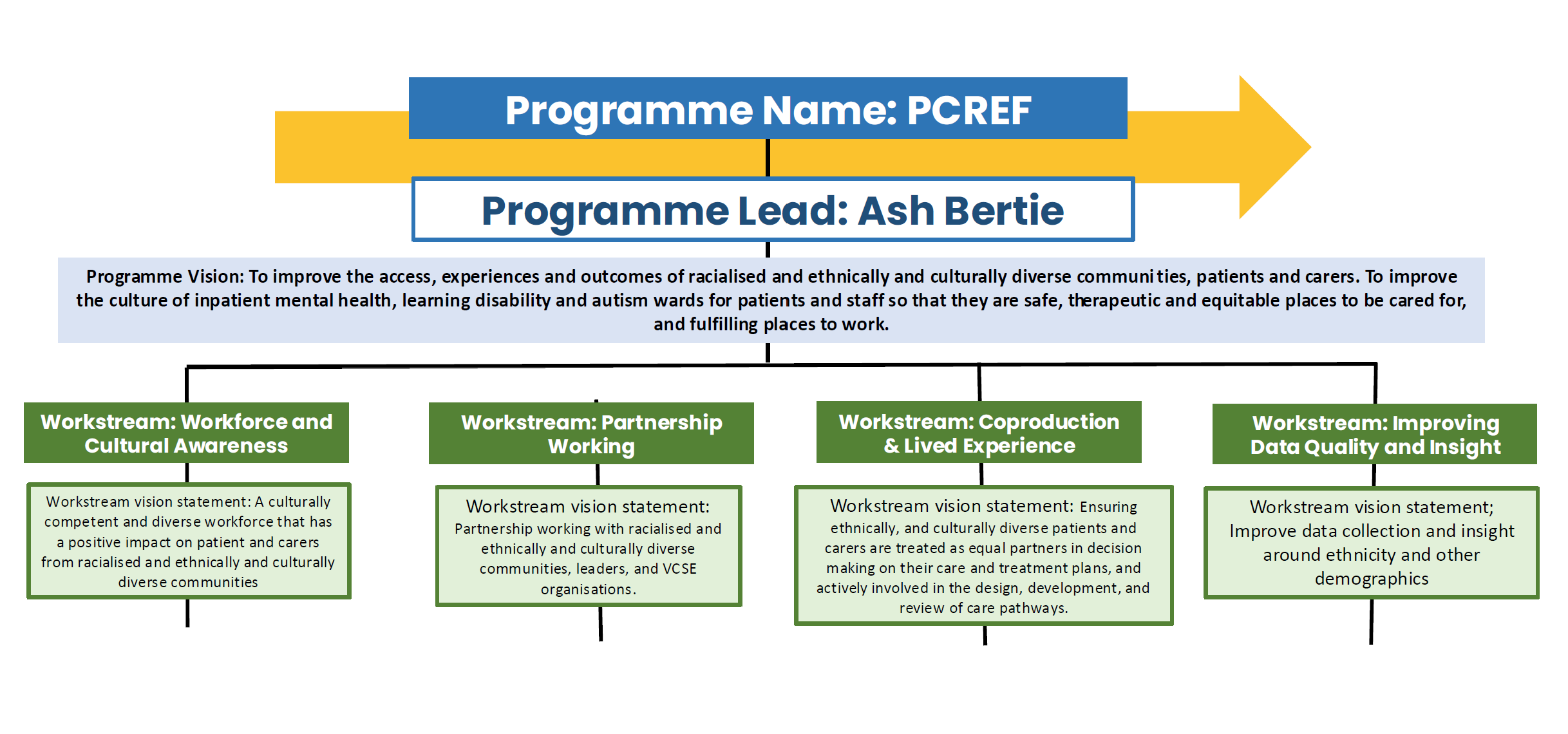
Matthew McKenzie opened the meeting by reflecting on over thirteen years of facilitating the forum and explained how its purpose has grown alongside national initiatives such as the Patient and Carer Race Equality Framework (PCREF) and the Triangle of Care. The forum continues to provide a national platform where carers can influence NHS services, hear about new research and share experiences with professionals and decision-makers.
Matthew introduced the day’s programme, which included research presentations, NHS England engagement, updates from mental health trusts and national organisations, and opportunities for carers to influence future policy
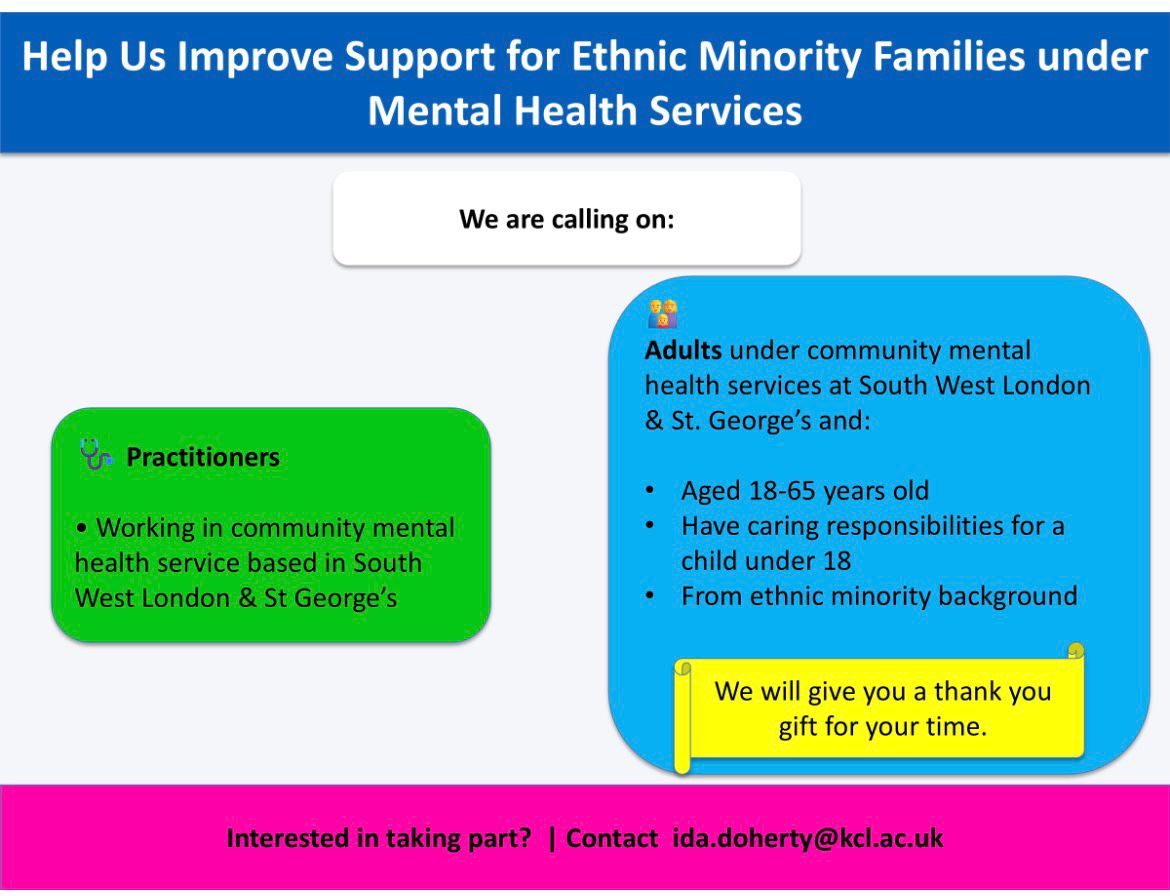
Dr Ida Doherty – King’s College London
Supporting Ethnic Carers in South West London
Dr Ida Doherty presented her doctoral research exploring how adult mental health services support ethnic minority families where a parent experiences mental illness.
She explained that despite national policy promoting a Think Family approach, implementation across England remains inconsistent. Many parents receiving mental health support are never asked about their children, meaning opportunities for preventative family support are often missed.
Discussion Highlights
This presentation generated one of the longest discussions of the meeting.
Carers highlighted:
- Adult and children’s services continue to work separately.
- Families often have to repeat their stories to multiple organisations.
- Parents fear seeking support because of concerns about children being removed.
- Structural racism continues to affect safeguarding and mental health services.
- Disabled parents and carers experience multiple layers of discrimination.
- Services often respond only during crisis rather than providing early intervention.
There was also an important discussion about safeguarding carers who participate in research. Participants stressed that research should include emotional support, culturally appropriate safeguarding and co-produced approaches to prevent re-traumatisation. Dr Doherty welcomed these suggestions and explained the safeguarding measures built into her study.
Dr Doherty encouraged forum members to promote the study across South West London to help ensure ethnic families are represented within the research.
Certainly. Here’s a more professional version that focuses on the discussion rather than identifying who asked each question.
Questions and Discussion
Q1. How can mental health services better implement the “Think Family” approach?
A question was raised about the continuing separation between children’s and adult mental health services, with concern that families are often required to navigate multiple systems that fail to communicate with one another. It was suggested that supporting one family member in isolation overlooks the wider impact of mental illness on the entire household.
Response
Dr Doherty agreed that this is a significant challenge and explained that her research is centred on improving whole-family support. She highlighted that current services often operate in silos, limiting opportunities for early intervention and joined-up care. The aim of her research is to identify practical ways of embedding the Think Family approach more effectively within adult mental health services.
Q2. How will the research address the inequalities experienced by ethnic minority families?
A discussion focused on the additional challenges faced by ethnic minority families, particularly where disability, poverty, language barriers and mental health intersect. Concerns were raised about institutional racism, unequal treatment and the fear some parents experience when engaging with services.
Response
Dr Doherty acknowledged that these intersecting inequalities can significantly affect families’ experiences. She recognised that services can often adopt a risk-focused rather than strengths-based approach and explained that her research seeks to identify earlier, more supportive interventions that better meet the needs of ethnic minority families.
Q3. How will carers participating in the research be protected from emotional harm?
The discussion explored the importance of safeguarding participants involved in research. It was suggested that sharing lived experiences can be emotionally challenging and that researchers should have appropriate support mechanisms in place before, during and after participation.
Response
Dr Doherty explained that safeguarding had been a key consideration throughout the development of the study. She described how support, supervision, training and ongoing review have been built into the project, alongside close collaboration with Experts by Experience from the earliest stages of the research.
Q4. Will participants receive ongoing emotional support after difficult discussions?
A further question explored whether structured debriefing and emotional support would be available for participants who may experience distress after discussing traumatic experiences.
Response
Dr Doherty confirmed that the study includes a comprehensive safeguarding framework, including debrief sessions and wellbeing support. She explained that the project had undergone rigorous NHS ethics approval and that participant welfare continues to be reviewed throughout the research process.
Q5. How is co-production embedded within the research?
The final discussion focused on ensuring that the research is genuinely co-produced with ethnic communities rather than being designed solely from a professional perspective. There was also support for developing safeguarding approaches jointly with carers.
Response
Dr Doherty explained that co-production is fundamental to the project. She has worked alongside Experts by Experience since the study was first developed and described the research as something being undertaken in partnership with people who have lived experience. She also welcomed suggestions for strengthening carer-led safeguarding approaches as the project progresses.
Dr Maeve (King’s College London)
Research Study: The Nearest Relative under the Mental Health Act
Dr Maeve introduced a new King’s College London research project examining experiences of the Nearest Relative provisions within the Mental Health Act. She explained that the study aims to understand how the current legislation works in practice and gather views ahead of the proposed reforms to mental health law. The researchers are interested in hearing directly from people who have lived experience of the system, recognising that the Nearest Relative can play a crucial role in supporting someone during assessment, detention and treatment.
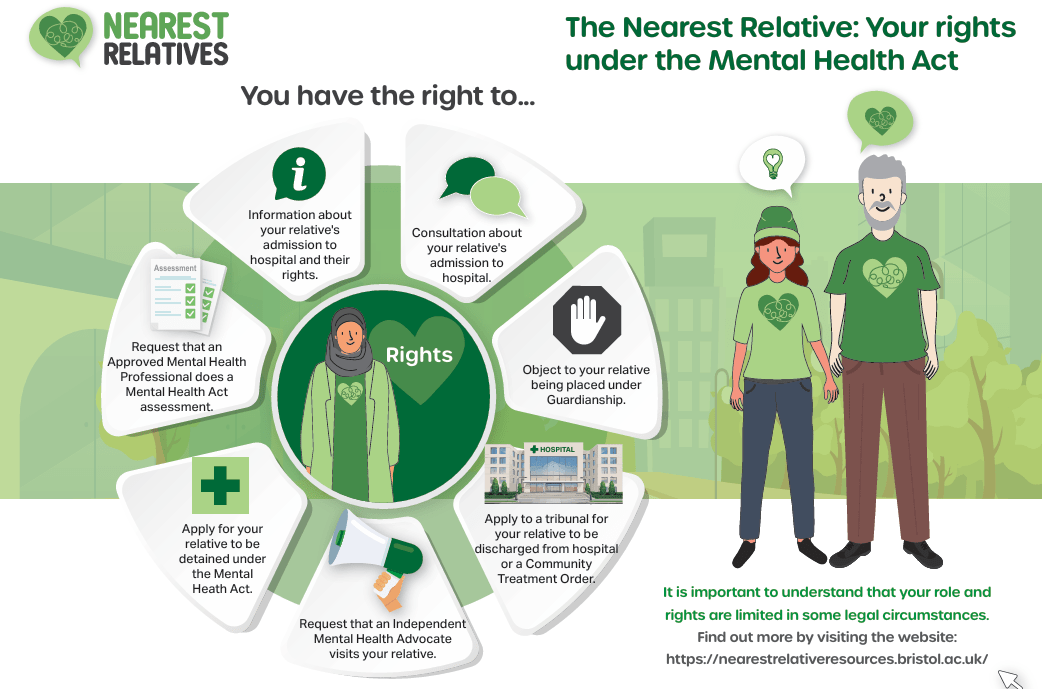
The study is seeking participants from a range of backgrounds, particularly unpaid carers who have supported someone detained or assessed under the Mental Health Act, as well as individuals who have themselves experienced detention or assessment. The research team is especially keen to hear from Black and other ethnic minority communities, along with younger people, to ensure that a wide range of perspectives help inform future policy and practice. Interviews are conducted online via Microsoft Teams at a convenient time for participants, last approximately one hour, and participants receive a £30 shopping voucher as a thank-you for contributing their experiences. Dr Maeve encouraged anyone interested to contact the research team or share the opportunity with others who may wish to participate.
Ruby Neish – University College London
Cancer Care and Black Women
Research Study: Supporting Carers of Women with Endometrial (Womb) Cancer
Ruby Neish, a Master’s researcher from University College London working in collaboration with the Centre for Early Detection, introduced a research project exploring the experiences of family members, friends and unpaid carers supporting women diagnosed with endometrial (womb) cancer. She explained that while much research focuses on the experiences of patients themselves, comparatively little is known about the challenges faced by those providing informal care throughout diagnosis, treatment and recovery. The study aims to build a more complete picture by understanding how carers experience the cancer pathway, the support they receive and the barriers they encounter. Ruby emphasised that carers often play a vital role in navigating appointments, providing emotional support, helping with treatment decisions and managing the practical realities of living with cancer, yet their experiences are frequently overlooked in research.

Following the presentation, forum members shared a wealth of lived experience highlighting why this research is particularly important for Black and minority ethnic communities. The discussion explored how delayed diagnosis, language barriers, cultural expectations, disability, poor communication and wider health inequalities can all contribute to poorer experiences for both patients and their families. Members also reflected on the importance of improving awareness of cancer symptoms within communities, encouraging uptake of screening programmes and ensuring services are culturally responsive. Several contributors stressed that carers often become advocates, interpreters and navigators of the healthcare system, particularly where individuals experience multiple forms of disadvantage. The discussion reinforced the importance of ensuring that future cancer services recognise and support carers as an essential part of the patient’s journey.
Questions and Discussion
Q1. Why is it particularly important to understand the experiences of Black and minority ethnic women living with cancer?
Forum members discussed how people from Black and minority ethnic communities can face additional barriers throughout the cancer pathway. These included language differences, lower awareness of symptoms, cultural beliefs about illness, disability, mental health needs and difficulties accessing appropriate support. It was suggested that these factors can contribute to delayed diagnosis and poorer outcomes if services fail to respond to people’s individual circumstances.
Response
Ruby welcomed these observations and explained that hearing directly from carers is essential to understanding these inequalities. She noted that while patients’ experiences are being explored separately, the research hopes to capture the perspectives of carers to identify barriers that may otherwise remain invisible. Together, these findings will help build a more complete understanding of how cancer services can better support families from diverse communities.
Q2. How can cancer services improve early diagnosis within ethnic communities?
The discussion highlighted the importance of encouraging earlier engagement with screening programmes and improving awareness of cancer symptoms within local communities. Examples were shared of women whose diagnoses were delayed after repeated visits to healthcare services, alongside reflections on the positive impact that culturally appropriate information and trusted community support can have in encouraging people to attend screening appointments. Participants emphasised that services need to communicate in ways that are accessible and sensitive to different cultural backgrounds.
Response
The discussion reinforced that improving awareness, reducing communication barriers and working more closely with communities could contribute to earlier diagnosis and improved outcomes. The research aims to identify where carers believe improvements can be made across the diagnostic and treatment journey, helping to inform future service development.
Q3. What role do unpaid carers play throughout the cancer journey?
A final discussion focused on the often unseen contribution of unpaid carers. Members described how carers frequently provide emotional reassurance, accompany relatives to appointments, help explain medical information, advocate for concerns to be taken seriously and support individuals throughout treatment and recovery. It was recognised that carers often become the link between patients, families and healthcare professionals, particularly where communication barriers or additional health conditions exist.
Response
Ruby explained that this is precisely why the study is focusing on carers’ perspectives. Understanding their experiences will provide valuable evidence about the practical and emotional challenges carers face and identify ways that cancer services can better recognise and support them alongside the person receiving treatment.
NHS England – Allied Health Professions Strategy
Steve Tolan (Deputy Chief Allied Health Professions Officer) & Barry O’Donovan (Senior Programme Manager)
Steve Tolan and Barry O’Donovan from NHS England joined the forum to begin an important conversation about developing a new national Allied Health Professions (AHP) Strategy. Rather than presenting a completed strategy for consultation, they explained that NHS England wanted to engage with carers, patients and communities before the strategy was written, ensuring that lived experience would help shape its priorities from the outset.
Steve introduced the Allied Health Professions as the third largest clinical workforce in the NHS, comprising fourteen professions including occupational therapists, physiotherapists, speech and language therapists, dietitians, radiographers and several others. He explained that these professionals work across virtually every part of health and care, from mental health and primary care to acute hospitals, rehabilitation and community services, making their contribution central to improving patient outcomes.
Barry explained that NHS England was seeking honest feedback on what Allied Health Professionals currently do well and, more importantly, where improvements were needed over the next five years. The discussion centred around several key questions, including how AHPs could help people stay healthier for longer, improve prevention, reduce health inequalities, remove barriers to accessing care, and work more effectively across different care settings. Forum members were also encouraged to complete a wider national survey, but NHS England emphasised that hearing directly from unpaid carers during the meeting would provide invaluable insight into the everyday realities experienced by families supporting loved ones with mental illness and other long-term conditions.
What followed was one of the richest discussions of the meeting, with carers sharing personal experiences of navigating health services and offering practical recommendations for change. Contributors acknowledged the important work undertaken by Allied Health Professionals but stressed that future success would depend upon moving beyond clinical interventions alone. Members called for greater emphasis on prevention rather than crisis management, stronger action to address racism and health inequalities, more personalised and culturally responsive care, improved communication with families and better recognition of unpaid carers as essential partners within the healthcare system. NHS England representatives listened carefully throughout the discussion, responding positively to the feedback and confirming that the experiences shared during the forum would help inform the development of the national strategy.
Feedback from Forum Members
There was a lot more feedback, but I have only included 4 feedback to the strategy
Feedback 1 – Prevention must become the priority, not simply responding to crisis
One of the strongest messages from the discussion was that health services often intervene too late. Contributors explained that many families recognise early warning signs long before services become involved, yet support is frequently unavailable until a situation has escalated into crisis. Members argued that Allied Health Professionals are well placed to identify emerging concerns earlier, particularly for people living with long-term mental health conditions, autism, learning disabilities and chronic physical illnesses. Earlier intervention, they suggested, would reduce avoidable hospital admissions while improving outcomes for both patients and carers.
NHS England acknowledged this feedback, explaining that one of the key ambitions of the new strategy is to support the wider NHS objective of shifting from reactive treatment towards prevention. Representatives welcomed examples from carers illustrating where earlier support could make the greatest difference.
Feedback 2 – Tackling racism and health inequalities requires more than training
Forum members spoke candidly about experiences of racism, discrimination and unequal treatment within health services. While acknowledging that cultural awareness training is becoming more common, contributors argued that training alone is insufficient unless accompanied by accountability and meaningful changes in practice. Some described inaccurate clinical records, assumptions based on ethnicity and situations where concerns raised by families were not properly reflected in care planning. There was a strong call for services to improve communication, record keeping and trauma-informed practice, ensuring that staff understand the impact of racism on health outcomes rather than viewing cultural competence as a one-off training exercise.
NHS England representatives recognised that tackling health inequalities and promoting anti-racist practice were already identified as “non-negotiable” priorities within the developing strategy. They explained that this was precisely why engagement with forums such as this was so valuable, helping ensure that policy reflects the real experiences of people using NHS services.
Feedback 3 – Unpaid carers must be recognised as equal partners in care
A recurring theme throughout the discussion was the role of unpaid carers within healthcare systems. Members explained that carers are often the people coordinating appointments, supporting communication, monitoring deterioration, providing emotional support and helping professionals understand an individual’s needs. Despite this, carers frequently remain unidentified by services or receive little information and support themselves. Contributors argued that Allied Health Professionals should routinely identify carers, involve them in care planning where appropriate and recognise them as equal partners whose knowledge can significantly improve patient outcomes.
NHS England welcomed these comments and recognised that carers play a fundamental role in delivering effective, preventative care. The examples shared demonstrated how stronger partnerships with carers could improve continuity of care while helping services better understand the needs of individuals and families.
Feedback 4 – Share and learn from examples of excellent practice
The discussion concluded with examples of positive experiences that illustrated what good care can look like. One contributor described receiving outstanding support from an Occupational Therapist who not only arranged practical adaptations within the home but also followed up afterwards to ensure everything was working well. Members suggested that NHS England should identify and promote examples of excellent practice across the Allied Health Professions so that high standards become the norm rather than the exception. Ideas included involving patients and carers more directly in evaluating services and using lived experience to help identify what compassionate, person-centred care looks like in practice.
West London Health Trust – PCREF Update
Linda Thomas – Co-producing an Independent PCREF Advisory Group
Linda Thomas, Co-production and Partnerships Development Manager at West London NHS Trust, opened the Trust’s presentation by describing how they have developed an independent PCREF Advisory Group designed to challenge, support and hold the Trust to account as a “critical friend.” Rather than creating a traditional advisory panel, West London NHS Trust commissioned three established community organisations GOS&D (Ealing), SHEWISE (Hounslow) and Managing Our Mental (Hammersmith & Fulham) to help design the model and understand how communities genuinely want to engage with mental health services. The approach seeks to increase diversity of voices, identify barriers preventing community involvement and rebuild trust between local communities and the Trust. Linda explained that members of the advisory group now sit alongside Trust leaders as equal partners on the Steering Group, while work is progressing to secure long-term funding to sustain the network and strengthen relationships with community organisations. The initiative demonstrates how co-production can move beyond consultation towards genuine shared decision-making between the NHS and the communities it serves.
Debbie Best – PCREF Carer Lead: Racial Trauma Workshops
Debbie Best, PCREF Carer Lead at West London NHS Trust, presented the development of the Trust’s Racial Trauma Workshops, which were co-designed alongside Natalie Mark (PCREF Lived Experience Lead), Dr Anne Aiyegbusi and Chief Nurse Gillian Kelly. Debbie explained that the workshops were created in response to the persistent racial inequalities experienced within mental health services, including disproportionate detention under the Mental Health Act, restrictive interventions, mistrust of services and the re-traumatisation experienced by many people from ethnic communities.
Rather than delivering traditional equality training, the workshops create reflective spaces where staff openly discuss difficult issues including trust, power, emotional labour, racialised assumptions and barriers to culturally safe care. Debbie emphasised that racial trauma affects not only patients but also carers and NHS staff, and that creating psychologically safe spaces for honest conversations is an essential step towards improving relationships, reducing inequalities and embedding the aims of the Patient and Carer Race Equality Framework (PCREF) across mental health services.
Christine – Triangle of Care, Carer Awareness Training and PCREF
Christine, speaking as a carer representative involved in co-production, highlighted how West London NHS Trust has successfully embedded carers within staff training through the Triangle of Care programme. She explained that the Trust achieved Stage 2 Triangle of Care accreditation in March 2026 and has developed Carer Awareness Training that is designed and delivered alongside carers themselves.
The training introduces staff to both the Triangle of Care and the Patient and Carer Race Equality Framework, helping colleagues understand the importance of recognising carers as equal partners while strengthening communication and collaboration with families. Christine also announced that West London NHS Trust has been selected as one of only thirteen national pilot sites testing the integration of Triangle of Care and PCREF guidance over the next twelve months. Ten clinical teams will take part in reviewing and implementing the updated guidance, ensuring that national best practice is informed by both professional expertise and lived experience.
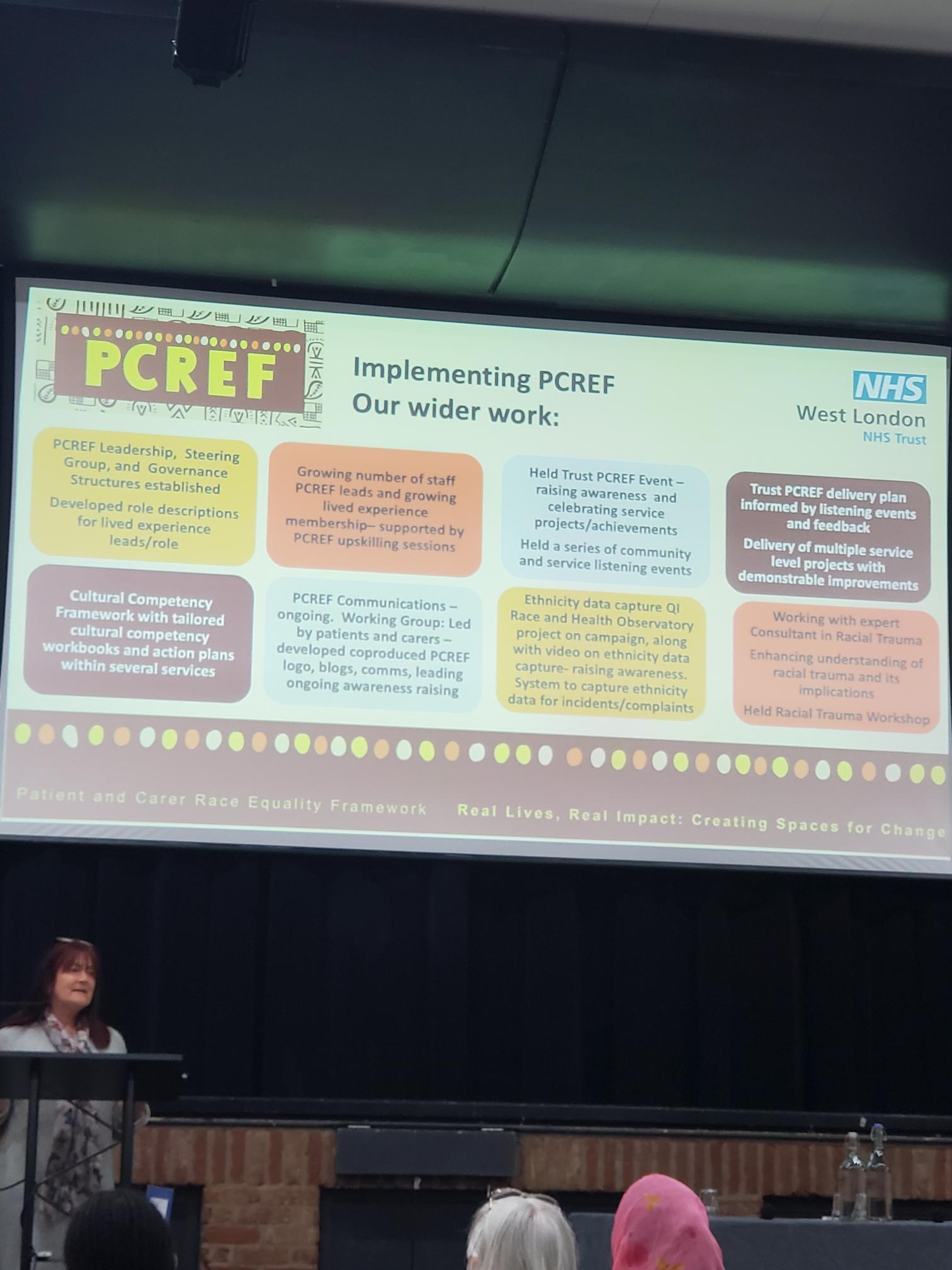
Debbie Best – Ethnicity Data Capture Project
Debbie concluded the presentation by introducing West London NHS Trust’s Ethnicity Data Capture Project, funded through a small grant from the NHS Race and Health Observatory. She explained that the project aims to improve understanding of why ethnicity information is not always accurately recorded and why some communities remain reluctant to share this information. Working alongside community organisations including SHEWISE, Our Voices and Managing Our Mental, the Trust has co-produced a range of resources including information leaflets, awareness films, social media campaigns, frequently asked questions and staff training materials. The campaign, titled “Seen, Heard, Counted,” aims to reassure communities that ethnicity data is collected to improve healthcare, tackle inequalities and ensure services better reflect the needs of local populations. Debbie explained that the next phase of the project will focus on wider public awareness and rolling out staff training across the Trust to improve confidence, transparency and trust around ethnicity data collection.
Bren McInerney
Race Equality Observatory
Bren McInerney provided an update on behalf of the NHS Race and Health Observatory, explaining that although he works closely with the organisation through its Stakeholder Engagement Group, he was speaking from his role supporting engagement rather than as an NHS employee. He began by outlining the Observatory’s purpose, which is to identify, understand and help reduce ethnic inequalities across health and social care through research, evidence and partnership working.

Bren highlighted that the Observatory has now produced a growing body of evidence to support NHS organisations in tackling inequalities and emphasised that this work must ultimately lead to practical improvements in services rather than simply producing reports. He also noted that the Observatory’s current funding arrangement is due for renewal in 2027, making it increasingly important to demonstrate the value and impact of its work across the NHS. The presentation encouraged attendees to remain engaged with the Observatory’s programmes and continue sharing lived experience to strengthen the evidence base for future policy and service improvement.
Bren also highlighted several recent initiatives designed to strengthen collaboration between the NHS and local communities. These included the publication of the Trauma-Informed Care and Racialised Communities Report, which explores how trauma-informed approaches can better respond to the experiences of people affected by racism and discrimination. He also described the Observatory’s Small Grants Programme, which has supported community-led projects across England, and introduced a new Community Participation and Co-production Resource developed in partnership with the Race Equality Foundation. This resource aims to help NHS organisations and Integrated Care Boards build stronger relationships with communities, improve meaningful involvement in decision-making and ensure that local knowledge helps shape healthcare services. Bren concluded by encouraging carers, voluntary organisations and community leaders to make use of these resources, share them widely and continue influencing the national conversation on race equality within health services.