By Matthew McKenzie – Triangle of Care – Community group chair
Putting Carers at the Centre of Care
The latest Triangle of Care Community Group brought together carers, professionals and partner organisations from across England to share learning, celebrate progress and identify where further improvements are needed. The meeting highlighted the growing influence of the Triangle of Care across mental health and acute services, whilst reinforcing that there is still much work to do to ensure carers are consistently recognised, valued and supported.

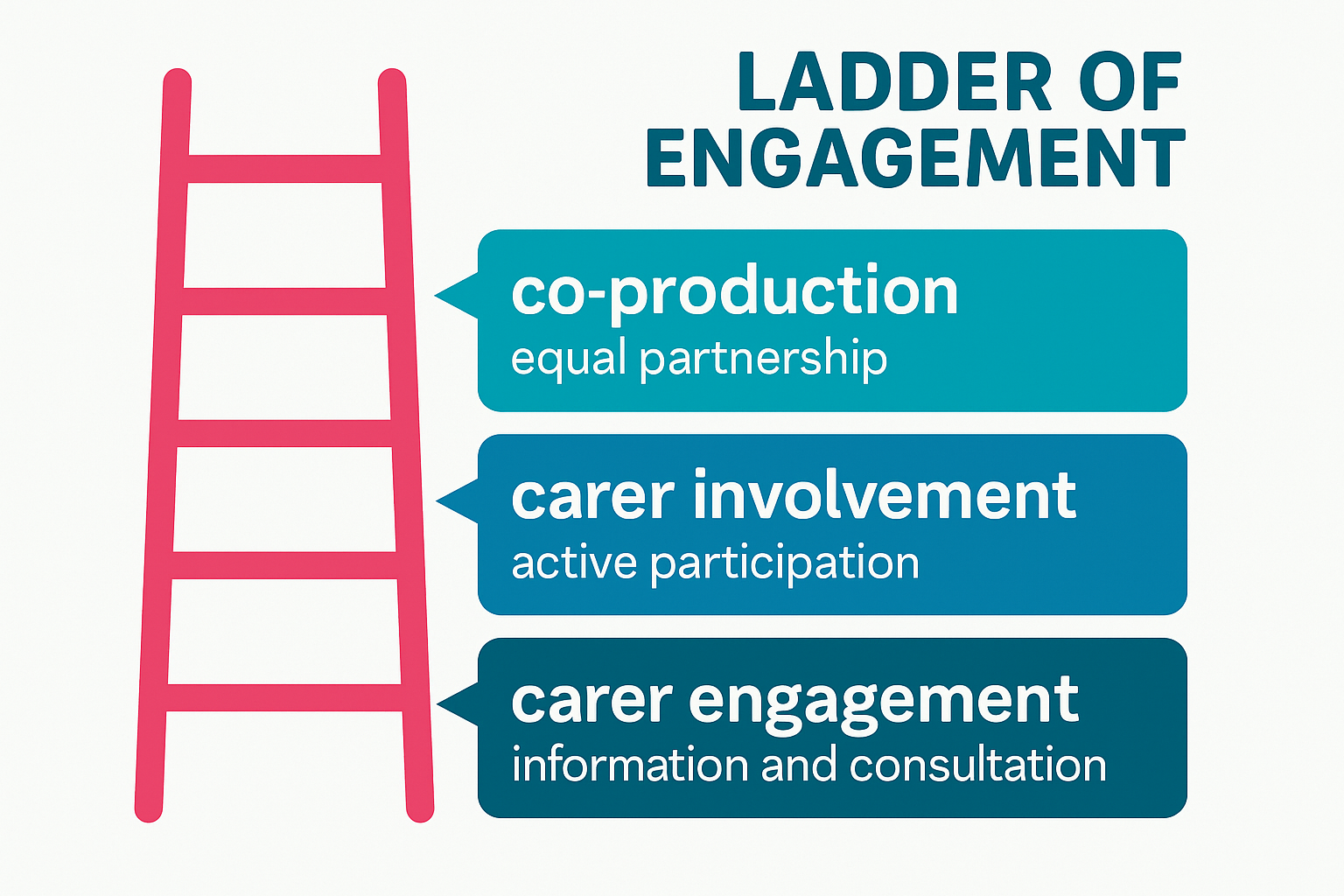
One of the most powerful aspects of the meeting was hearing directly from carers about their experiences. Whilst many spoke positively about the progress that has been made over recent years, there was a shared view that carer involvement remains inconsistent across services. Carers described feeling more included than ever before, with greater awareness of the Triangle of Care principles and more opportunities to participate in steering groups, service developments and community discussions. However, concerns remain around automatic carer identification, information sharing and ensuring that carers are genuinely recognised as partners in care.

Several carers reflected on the importance of having their voices heard early in a patient’s care journey. Examples were shared of services introducing carer contribution templates that ensure family members are involved within 72 hours of admission, whilst others highlighted improvements to confidentiality processes that allow patients to determine what information can be shared with carers at different stages of their recovery. These practical changes demonstrate how relatively small adjustments can have a significant impact on relationships between carers, patients and professionals.
Progress Across the Triangle of Care Programme
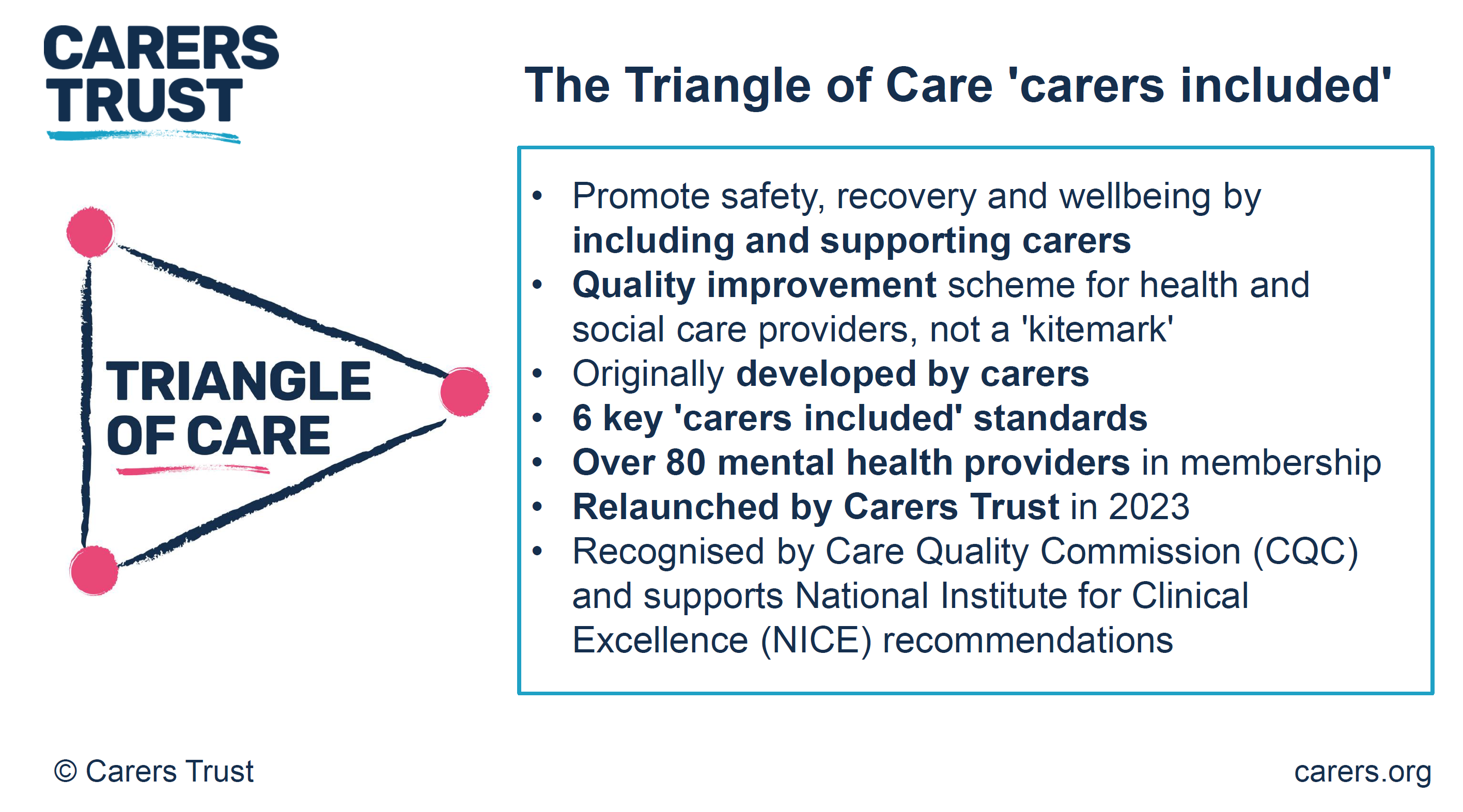
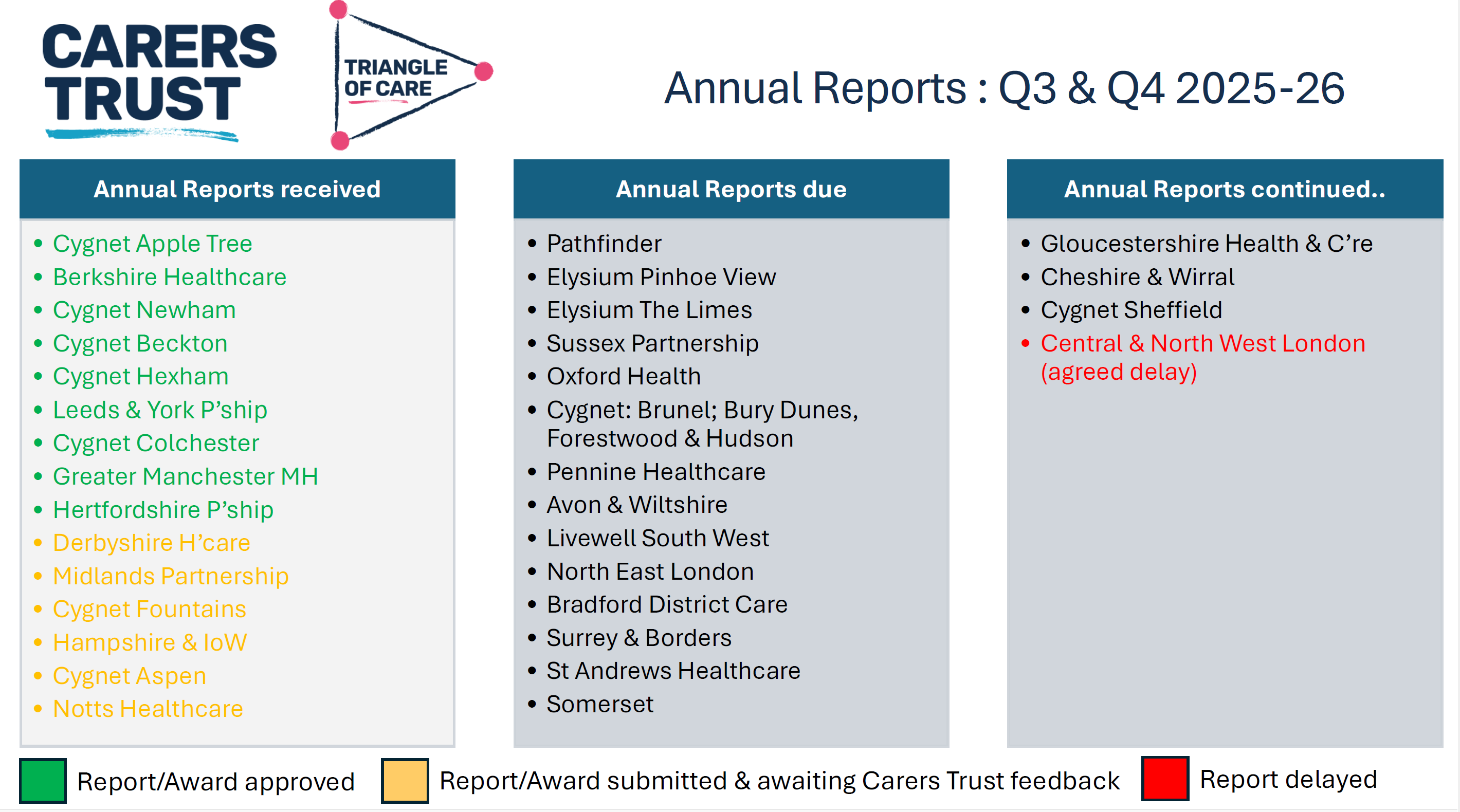
Mary Patel, Triangle of Care Programme Lead at Carers Trust, provided an update on developments across the national programme. The Triangle of Care continues to grow, with a number of organisations progressing through the STAR accreditation process and demonstrating their commitment to embedding carer-inclusive practice across services.
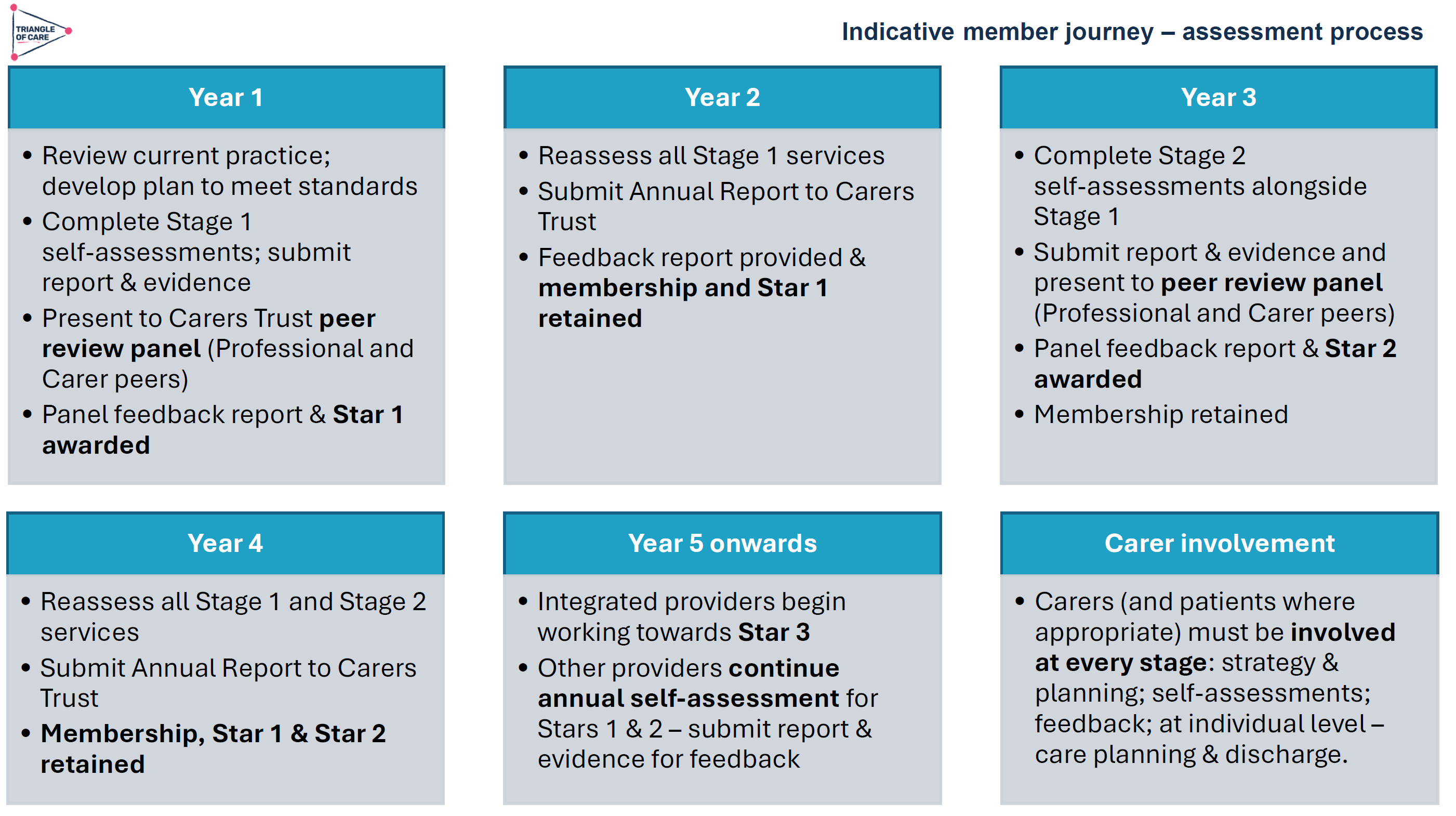
Importantly, members were reminded that the STAR awards are not designed to rank organisations, but instead reflect the breadth of implementation across different service areas. STAR I focuses primarily on inpatient and crisis services, STAR II expands into community services, whilst STAR III recognises organisations delivering integrated services across multiple clinical areas.
Several trusts have recently achieved STAR awards, whilst others are progressing through the assessment process over the coming months. The programme’s peer review approach continues to ensure that carers remain central to the assessment process, with carers actively involved in reviewing evidence, identifying good practice and making recommendations for future development.
The Triangle of Care Member Hub continues to provide valuable opportunities for peer learning, resource sharing and collaborative working. Upcoming webinars will include sessions exploring Open Dialogue approaches developed by Devon Partnership NHS Trust, providing members with further opportunities to learn about therapeutic models that place families and carers at the heart of care planning.
Advancing Equality Through the Patient and Carer Race Equality Framework
A significant development announced during the meeting was the launch of Phase Two of the Triangle of Care and Patient and Carer Race Equality Framework (PCREF) project.

PCREF represents the first mandatory anti-racism framework within mental health services in England. Recognising that carers from racially marginalised communities often experience poorer outcomes and face additional barriers when accessing support, the Triangle of Care programme has been working collaboratively with carers and mental health providers to strengthen the way services assess and respond to carers’ needs.
The revised self-assessment framework encourages services to move beyond assumptions and adopt a more professionally curious approach to understanding carers’ individual experiences. Rather than viewing carers as a homogenous group, the framework recognises that caring experiences are shaped by culture, identity, language, personal circumstances and wider health inequalities.
Pilot sites from across England are now testing the revised guidance, with learning being shared nationally throughout the project. Importantly, organisations do not need to be participating in the pilot to begin implementing the principles and learning that emerge from this work.
Alongside PCREF, Carers Trust continues to contribute to national policy developments, including the Modern Service Framework for Severe Mental Illness and the forthcoming Mental Health Strategy for England. Throughout these discussions, there has been a consistent message that carers must be recognised as partners in care and have access to appropriate support in their own right.
Confidentiality, Information Sharing and Carer Inclusion
Confidentiality remained one of the most prominent themes throughout the meeting. Whilst participants acknowledged the importance of protecting patients’ rights and preferences, carers highlighted that confidentiality can sometimes become a barrier to meaningful engagement.
Several contributors reflected that confidentiality should never prevent professionals from listening to carers’ concerns or receiving valuable information that may support a patient’s care. Others spoke about the importance of revisiting conversations around consent over time, recognising that patients’ preferences may change as their circumstances and wellbeing improve.

Practical examples of good practice included breaking confidentiality discussions down into specific areas, allowing patients to decide what information can be shared about medication, activities, wellbeing and treatment plans, rather than relying on simple ‘yes or no’ decisions. There was also discussion around the importance of staff training to improve confidence when navigating complex conversations around confidentiality and information sharing.
Participants agreed that carers should never be expected to provide significant levels of support without receiving the information necessary to do so safely and effectively. Achieving the right balance between confidentiality and partnership working remains an important priority for the Triangle of Care community.
Triangle of Care Principles Within Acute Services
The meeting concluded with an inspiring presentation from Wendy Doyle, Head of Patient Experience at St George’s University Hospitals NHS Foundation Trust and Epsom and St Helier Hospitals, exploring how Triangle of Care principles can be successfully implemented within acute hospital settings.

Whilst the Triangle of Care originated within mental health services, Wendy demonstrated that its principles are equally applicable across acute care environments. Her organisation supports approximately 19,000 members of staff across multiple hospital sites and has developed a comprehensive approach to identifying, recording and supporting unpaid carers.
Staff are encouraged to identify carers at the earliest possible opportunity, with this information recorded within patient records to ensure continuity throughout the patient’s hospital journey. Comprehensive carer awareness training is delivered through virtual sessions, ward-based education and e-learning resources, helping staff understand both the practical and emotional importance of recognising carers.
Importantly, identifying carers is only the beginning of the process. Every carer recorded within the hospital system receives a follow-up wellbeing check from the Patient Experience Team to discuss their own support needs, identify any challenges and facilitate referrals to local carers’ organisations where appropriate.
Partnership working sits at the heart of this approach, with close collaboration between acute services and local carers’ centres ensuring carers can access a broad range of practical and emotional support. Adult and Young Carers’ Charters have also been co-produced with carers themselves, helping to shape organisational commitments around kindness, inclusion and meaningful engagement.
Perhaps most importantly, Wendy highlighted that supporting carers improves outcomes for everyone. Better communication strengthens discharge planning, reduces avoidable hospital admissions and readmissions, improves patient safety and helps prevent carer burnout. Acute hospital stays can provide valuable opportunities to identify carers who may previously have remained invisible and connect them with longer-term support.
Looking Ahead
The discussions throughout the meeting demonstrated both the progress that has been made and the challenges that remain. There is increasing recognition that carers are essential partners in delivering high-quality care across both mental health and acute services. However, meaningful involvement cannot rely upon individual goodwill alone; it requires consistent systems, robust policies and a genuine commitment to partnership working.
Looking ahead, the Triangle of Care programme will continue to expand opportunities for peer learning, influence national policy developments and support organisations to embed carer-inclusive practices across services. The ongoing work around PCREF and wider mental health policy developments provide important opportunities to ensure that carers’ voices remain central to future service transformation.

Above all, the meeting reinforced a simple but powerful message: carers must not be viewed as an afterthought or an optional addition to care planning. They are experts through experience, invaluable partners in care and individuals with support needs of their own. When carers are identified early, listened to meaningfully and supported appropriately, outcomes improve not only for carers themselves, but for patients, families and services alike.
The Triangle of Care Community Group continues to provide an important space where carers and professionals can learn from one another, challenge existing practices and work collectively towards more compassionate, inclusive and effective care.