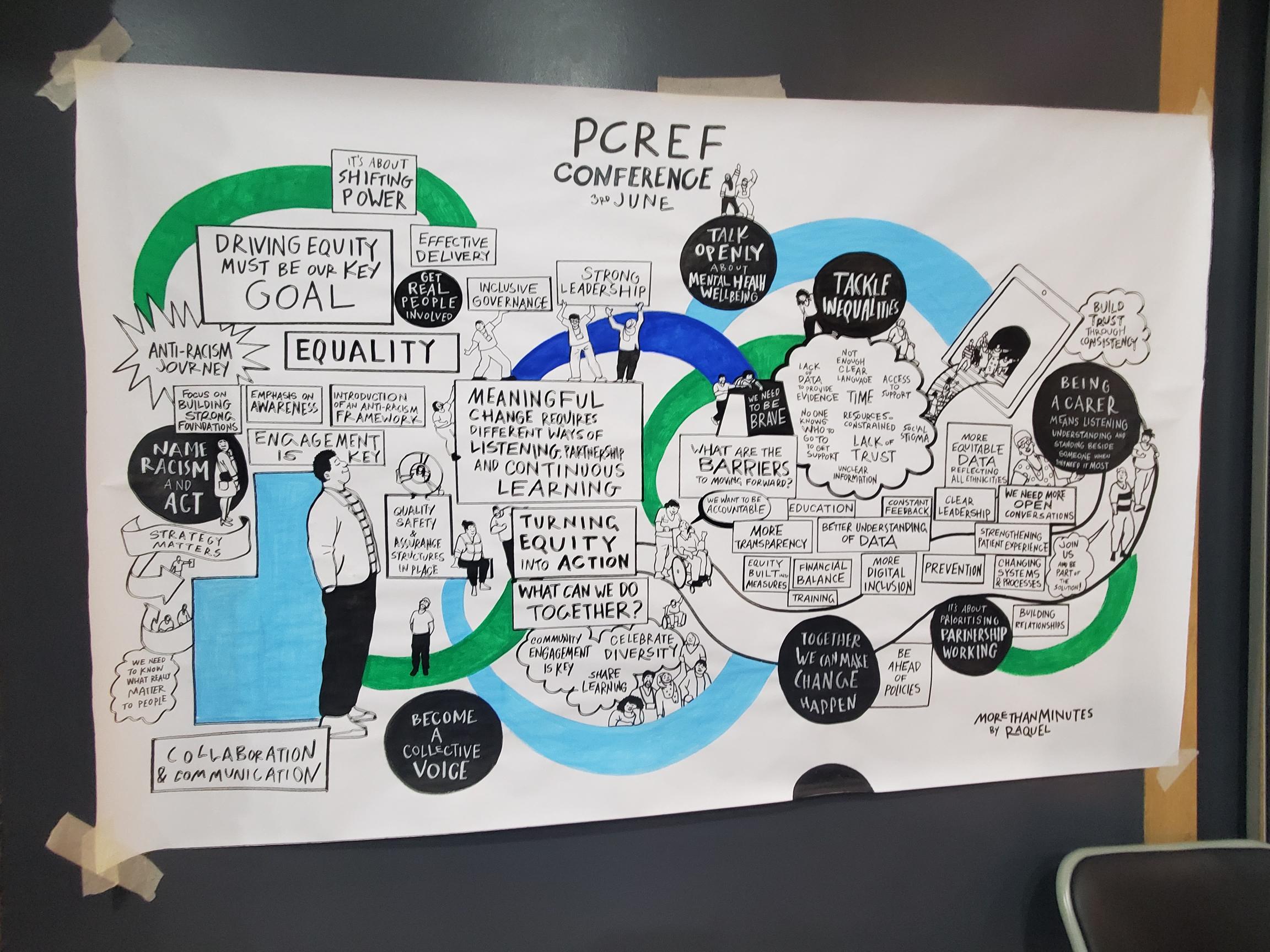
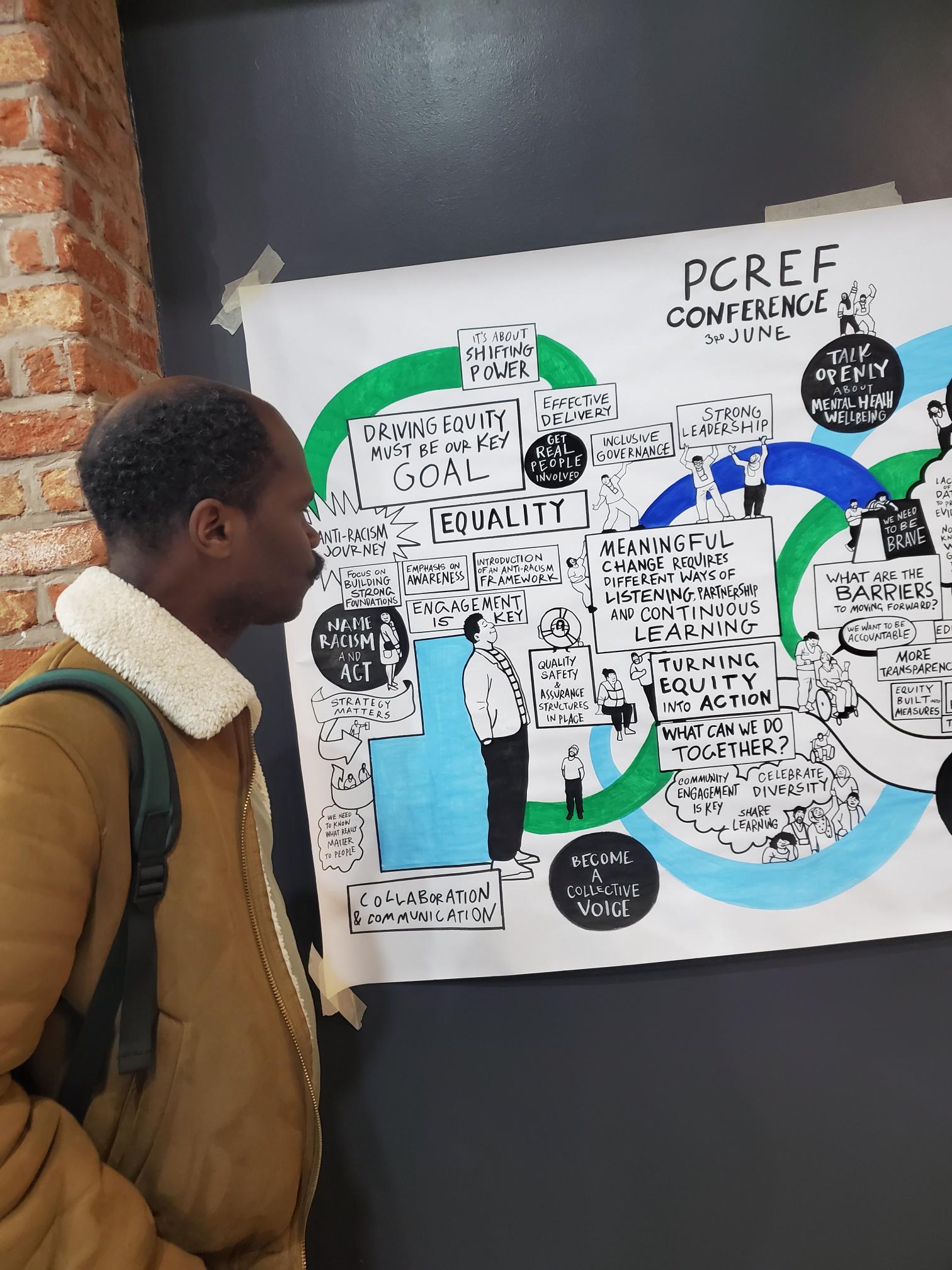
On Wednesday 3 June 2026, colleagues from all eight London Mental Health Trusts, alongside carers, service users, community organisations, researchers, regulators and system leaders, gathered at ISH Venues in central London for the Pan London Patient and Carer Race Equality Framework (PCREF) Conference.
Chaired by Erica deti from North East London NHS Foundation Trust (NELFT), the conference provided a unique opportunity to showcase progress, share learning and strengthen London’s collective commitment to race equity within mental health services.
The conference was built around the principle that advancing race equity requires both organisational commitment and meaningful partnership with people who use services, carers and communities. Throughout the day, speakers challenged delegates to move beyond discussion and towards action, recognising that the inequalities experienced by racialised communities within mental health services remain one of the most significant challenges facing the NHS.
South West London and St George’s Mental Health NHS Trust
The first trust presentation was delivered by Amdad Ibrahim, Associate Director of Health Inequalities, and Dr Mona Dhesi, Consultant Forensic Psychologist and Associate Medical Director at South West London and St George’s Mental Health NHS Trust. Their presentation provided one of the clearest examples of how PCREF can be fully integrated into organisational strategy. Beginning with an explicit acknowledgement that racism exists within healthcare organisations and wider society, they demonstrated how their trust had used this recognition as the foundation for meaningful action.
The speakers outlined a comprehensive anti-racism programme linking governance, workforce development, community engagement and service transformation. Race equity has been embedded into business planning, leadership accountability and quality improvement processes, supported by cultural capability programmes, anti-racism steering groups and health equity assessments.
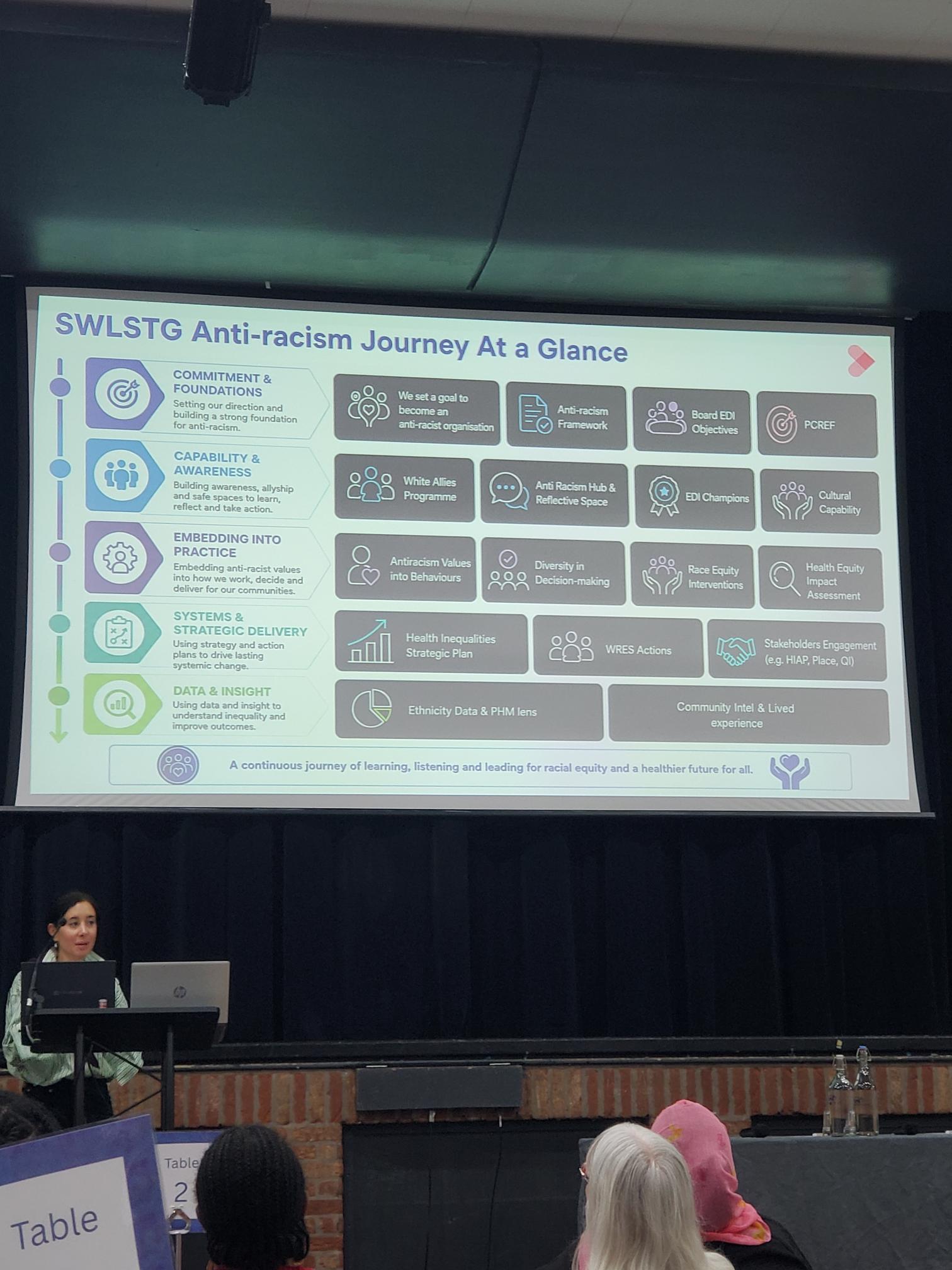
Their presentation demonstrated how PCREF can become part of the organisational DNA of a trust rather than a standalone initiative and provided a practical blueprint for others seeking sustainable implementation.
1. Commitment and Foundations
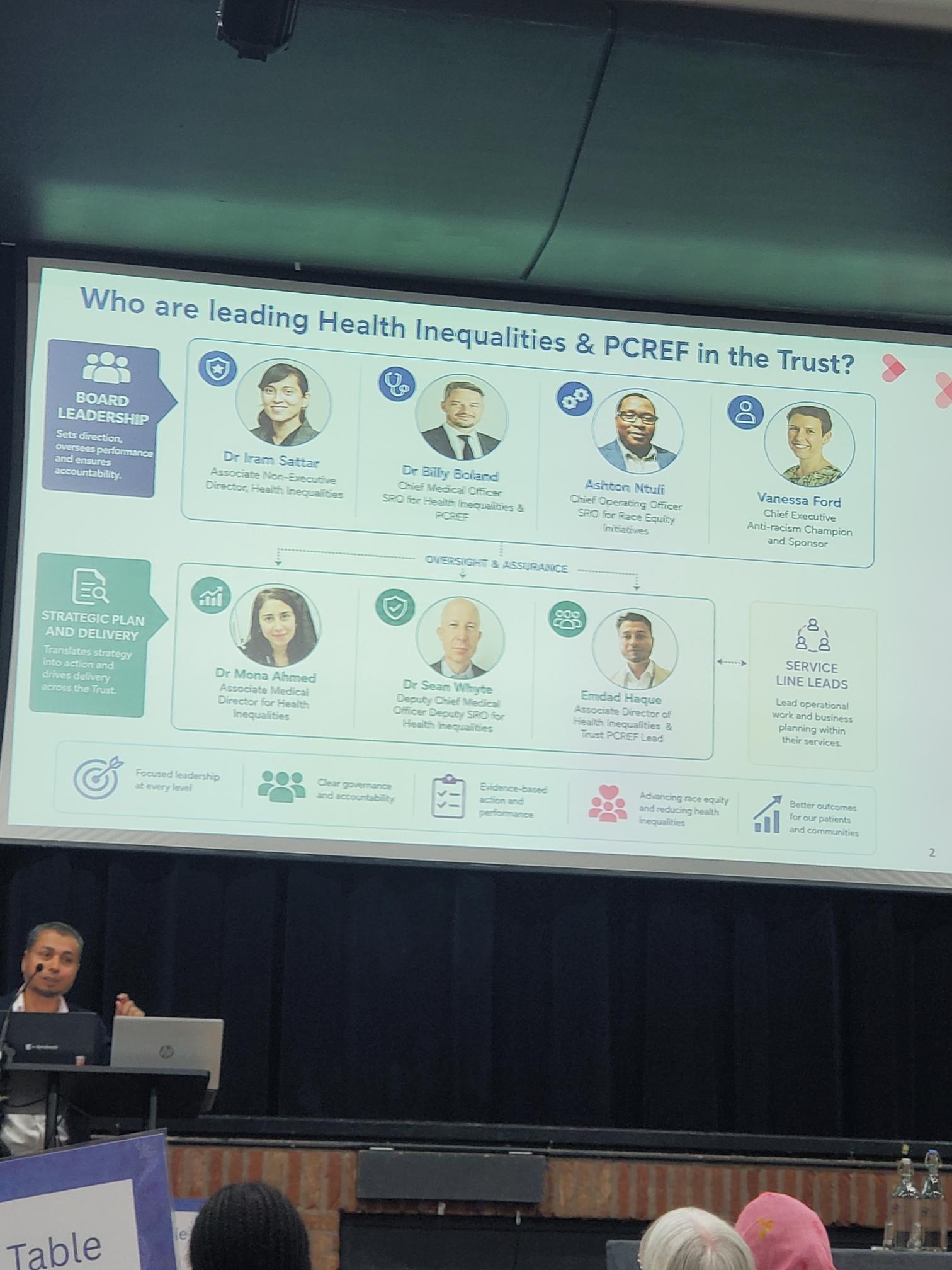
The Trust began by establishing a clear organisational commitment to becoming an anti-racist organisation. This commitment is supported through a range of strategic frameworks and governance structures, including the Trust’s Anti-Racism Framework, Board Equality, Diversity and Inclusion objectives, and the implementation of the Patient and Carer Race Equality Framework (PCREF).
Speakers emphasised that meaningful progress begins with leadership acknowledging that racism exists within healthcare systems and taking responsibility for addressing it. This commitment has been reinforced at Board level and incorporated into wider organisational priorities to ensure race equity remains visible and accountable.
2. Capability and Awareness
Recognising that sustainable change requires learning and reflection, the Trust has invested heavily in developing staff awareness and cultural capability. This includes initiatives such as:
- White Allies Programme
- Anti-Racism Hub and Reflective Spaces
- Equality, Diversity and Inclusion Champions
- Cultural Capability Training
These programmes create opportunities for staff to develop a deeper understanding of race, culture, privilege and inequality while providing safe spaces for reflection and discussion. The aim is to move beyond awareness and support staff to actively challenge inequity within their daily practice.
3. Embedding Anti-Racism into Practice
SWLSTG has focused on ensuring anti-racist values are embedded within decision-making processes and clinical practice rather than existing solely within training programmes.
Key areas of work include:
- Embedding anti-racist values into organisational behaviours
- Increasing diversity within leadership and decision-making structures
- Delivering targeted race equity interventions
- Using Health Equity Impact Assessments to inform service development
The Trust highlighted how race equity considerations are now being incorporated into service redesign programmes, policy development and clinical pathways, ensuring that decisions are assessed for their potential impact on different communities.
East London NHS Foundation Trust (ELFT)
Advancing Equity in All That We Do: ELFT Strategy 2026–2031
Presented by Carrie Sissons, Deputy Director of Integrated Care, East London NHS Foundation Trust shared how race equity and inclusion have been embedded at the heart of the Trust’s new 2026–2031 Strategy. Rather than developing a strategy behind closed doors, ELFT undertook an extensive engagement programme designed to ensure that the voices of service users, carers, staff and communities directly influenced the Trust’s future direction.
Carrie explained that the strategy was developed during a period of significant challenge for health and care services, but also a period of opportunity. The Trust recognised that if it was to improve outcomes for the diverse communities it serves across East London, Bedfordshire and Luton, equity could not be treated as a separate programme of work. Instead, it had to become a core principle underpinning every decision, every service and every improvement initiative undertaken by the organisation.
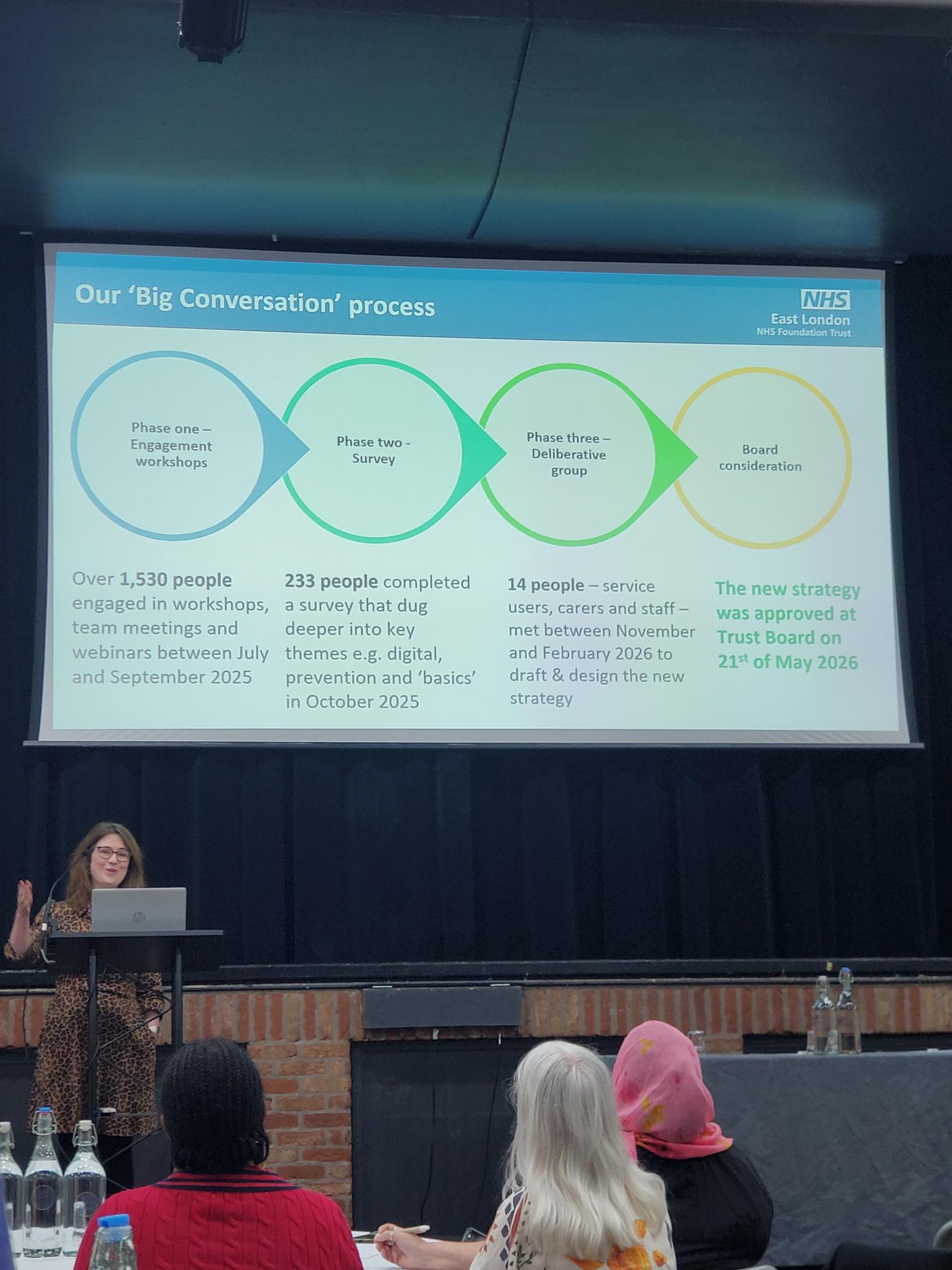
Building the Strategy Through the “Big Conversation”
A major feature of the strategy development process was the Trust’s extensive engagement exercise known as the “Big Conversation.” This programme was designed to ensure that the final strategy reflected the experiences, priorities and aspirations of the people who use and deliver services.
What People Told ELFT
One of the strongest messages emerging from the Big Conversation was the importance of equity. Participants consistently identified inequalities in access, experience and outcomes as issues that required sustained attention and action.
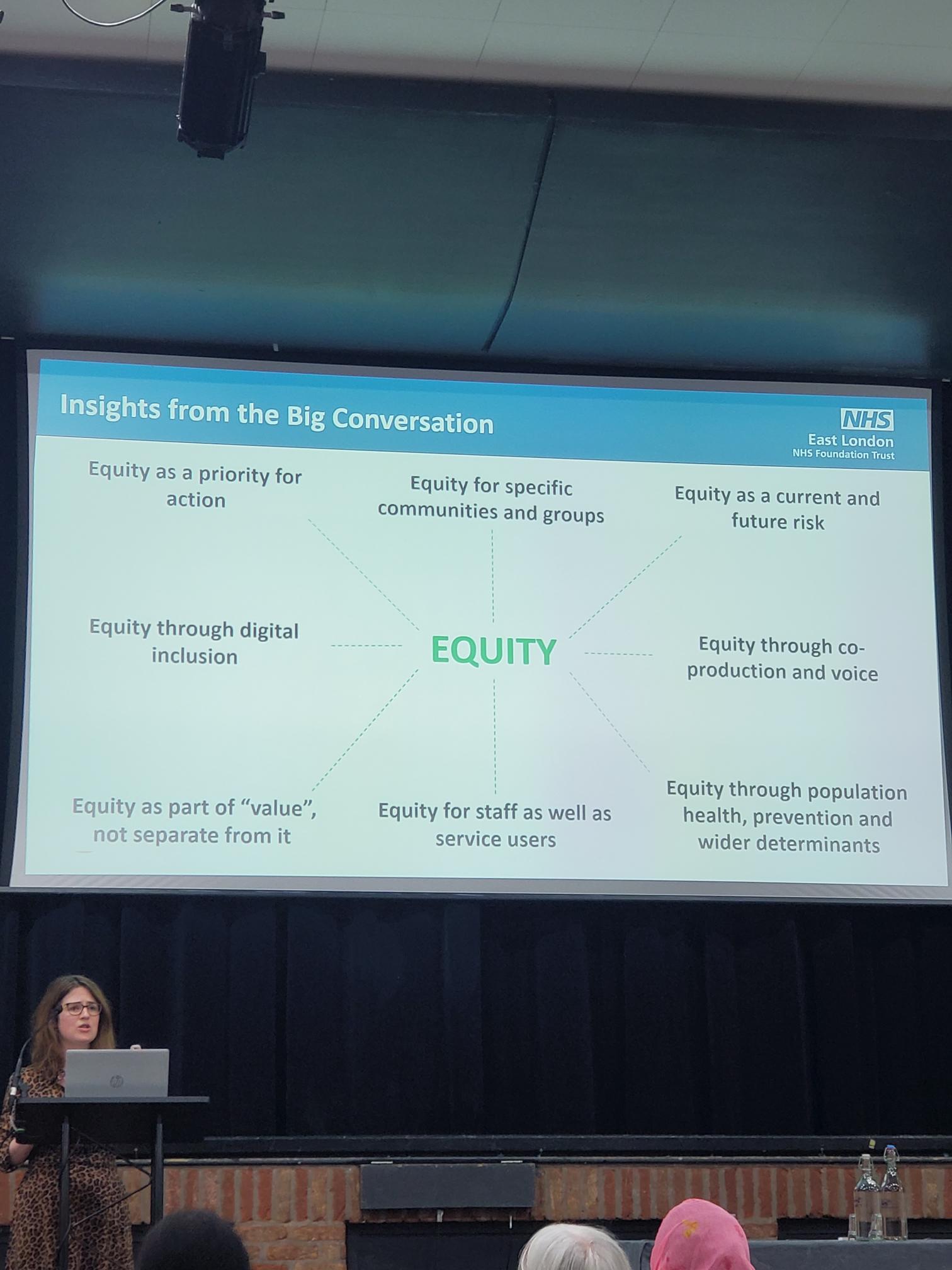
The engagement process highlighted several key themes:
- Equity as a priority for action.
- Equity for specific communities and groups.
- Equity as a current and future risk.
- Equity through co-production and lived experience.
- Equity through population health and prevention.
- Equity for staff as well as service users.
- Equity through digital inclusion.
- Equity as an essential part of value, not separate from it.
Carrie explained that these findings reinforced the need for equity to be visible throughout the Trust’s strategic objectives and operational plans. Participants wanted to see measurable action rather than broad commitments, with a focus on understanding and addressing disparities experienced by different communities.
The ELFT Strategy 2026–2031
The new strategy builds upon ELFT’s existing values and commitment to high-quality care. Serving approximately 1.8 million people across East London, Bedfordshire and Luton, the Trust recognised that reducing inequalities must remain central to its future ambitions.
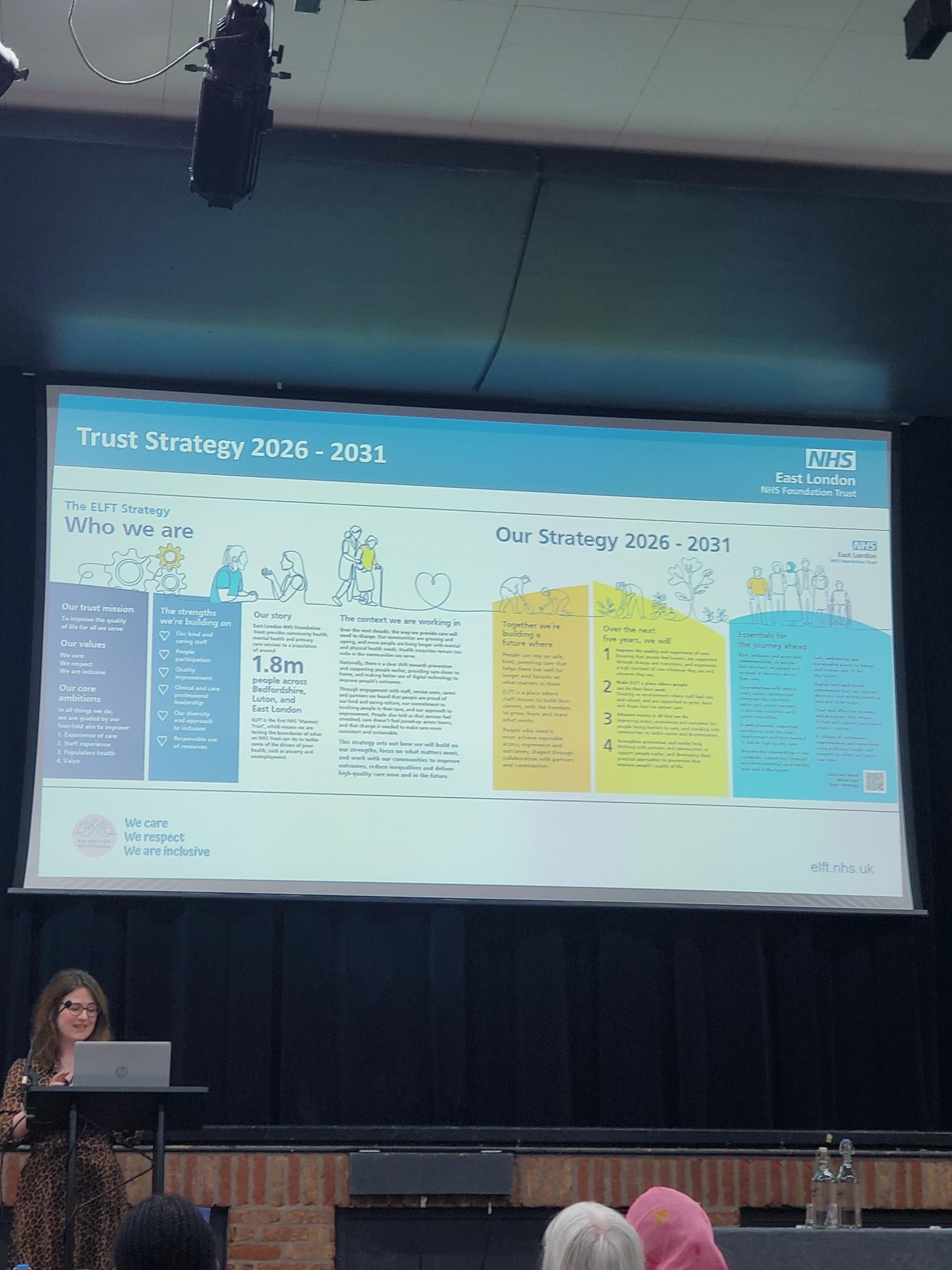
The strategy identifies four broad priorities for the next five years:
- Improve the quality and experience of care.
- Make ELFT a great place to work.
- Advance equity in all that we do.
- Work with partners and communities to improve lives.
Of these priorities, the commitment to advancing equity was particularly relevant to the themes of the PCREF conference.
Priority Three: Advance Equity in All We Do
Carrie described this priority as a commitment to ensuring that equity becomes embedded within everyday practice rather than being treated as a specialist programme.
By 2031, ELFT aims to ensure that:
- Teams routinely analyse access, experience and outcomes by population group.
- Services take action when disparities are identified.
- Progress continues against PCREF commitments.
- The Trust’s Anti-Racism Plan and Charter are actively implemented.
- Equity and inclusion are strengthened across the workforce.
- Inequalities experienced by racialised communities are reduced.
The strategy recognises that data alone is not enough. Equity must be considered throughout service design, quality improvement, workforce development and organisational decision-making.
West London NHS Trust
Presented by Debbie Best (PCREF Lead), Natalie Mark (Living Experience PCREF Lead) and Dr Anne Aiyegbusi, West London NHS Trust delivered one of the most powerful and thought-provoking presentations of the conference. Their session focused on racial trauma, exploring how racism affects patients, carers and staff, and how organisations can create safe spaces to acknowledge, understand and respond to those experiences.
The presentation was rooted in the recognition that racial inequalities remain deeply embedded within mental health services. The team explained that their work developed in response to persistent concerns around disproportionate referrals, detention rates and restrictive interventions experienced by racialised communities. They also highlighted how mistrust of services and experiences of re-traumatisation continue to affect people’s willingness to engage with mental health support. Importantly, they stressed that racial trauma is not only experienced by service users but also by carers and staff, many of whom continue to navigate systems that can reproduce inequity.
Why This Work Matters
West London NHS Trust identified several key issues that informed the development of their racial trauma programme:
- Disproportionate rates of referrals and detention among racialised communities.
- Higher levels of restrictive interventions within mental health pathways.
- Mistrust of services due to previous negative experiences.
- The risk of re-traumatisation through interactions with healthcare systems.
- The impact of racism on patients, carers and staff alike.
A particularly striking message from the presentation was that many racialised staff attending the workshops were not learning about racial trauma as a new concept. Instead, they were reflecting on experiences that formed part of their everyday reality. This observation reinforced the importance of creating environments where these experiences can be discussed openly and safely.
Co-produced Learning Spaces
The racial trauma workshops were developed through a co-production approach involving Debbie Best, Natalie Mark and Dr Anne Aiyegbusi, a forensic psychotherapist, group analyst and registered nurse who has published extensively on racial trauma. Together they designed reflective learning spaces where participants could explore difficult but essential conversations around race, identity and mental health.
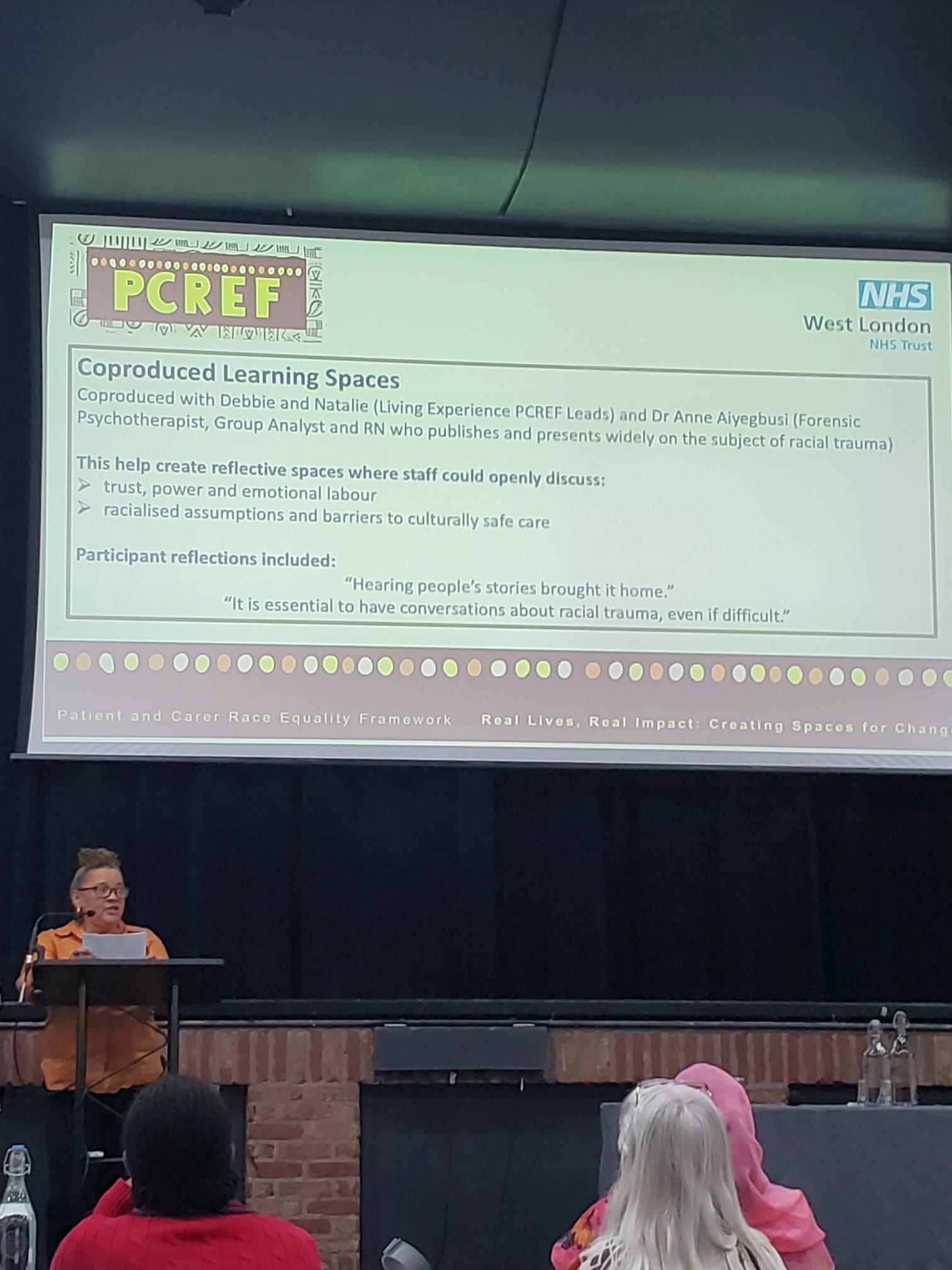
The workshops encouraged participants to discuss:
- Trust, power and emotional labour.
- Racialised assumptions within healthcare.
- Barriers to culturally safe care.
- Experiences of racism in professional and personal settings.
- Organisational responsibilities in responding to racial trauma.
Feedback from participants demonstrated the impact of these conversations. Attendees reported that hearing people’s lived experiences brought the issues to life in ways that data alone could not achieve. Many described the workshops as challenging but necessary, with one participant stating that conversations about racial trauma are essential even when they are uncomfortable.
Wider PCREF Implementation at West London NHS Trust
Alongside the racial trauma work, the presentation highlighted wider progress being made through PCREF implementation across the Trust.
Key achievements included:
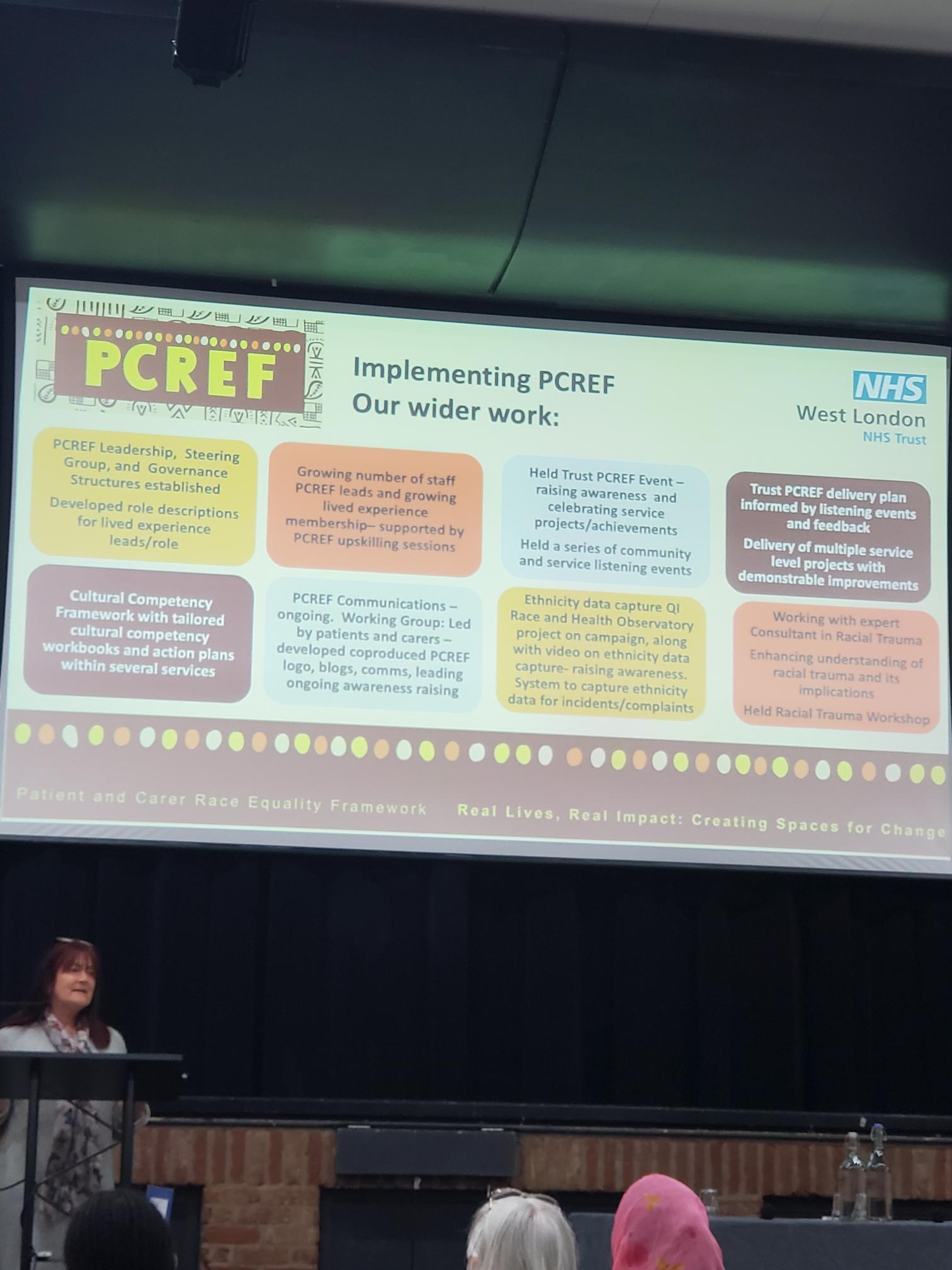
- Establishing PCREF leadership, steering groups and governance structures.
- Developing dedicated lived experience leadership roles.
- Increasing the number of PCREF leads and lived experience members.
- Delivering Trust-wide PCREF awareness events.
- Running community listening events and engagement activities.
- Developing a Cultural Competency Framework and tailored action plans.
- Creating co-produced communications led by patients and carers.
- Improving ethnicity data collection and reporting systems.
- Working with specialist racial trauma consultants to strengthen organisational understanding.
Particularly noteworthy was the emphasis on co-production. Patients and carers were not simply consulted but actively involved in shaping communications, governance structures, learning programmes and strategic priorities. This demonstrated a commitment to ensuring that those most affected by inequalities have a meaningful voice in driving change.
Key Learning from West London NHS Trust
The West London presentation demonstrated that addressing racial inequalities requires more than policy changes alone. It requires organisations to create spaces where difficult conversations can happen safely, where lived experience is valued as expertise and where learning leads directly to action.
Their work showed that racial trauma is not solely an individual experience but an organisational challenge that requires leadership, accountability and sustained commitment. By combining co-production, cultural competency, workforce development and organisational reflection, West London NHS Trust is helping to create the conditions for more equitable and culturally safe mental health services.
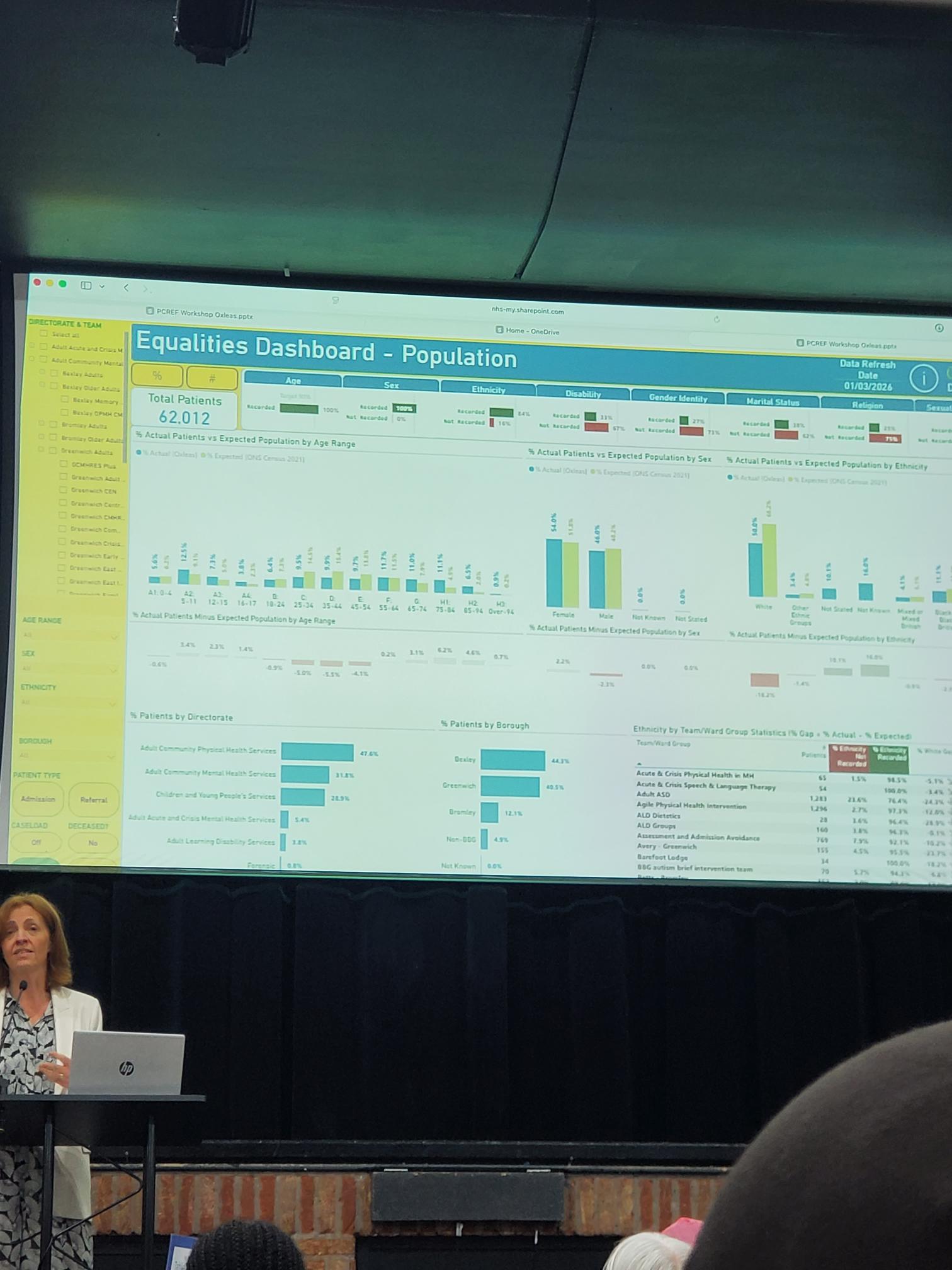
Oxleas NHS Foundation Trust
Reducing Inequalities in Restrictive Practice: From Data to Action
Presented by Oxleas NHS Foundation Trust, this session focused on reducing inequalities in restrictive practice through the lens of the Patient and Carer Race Equality Framework (PCREF). The presentation explored how data, lived experience, trauma-informed care and practical service improvements can work together to reduce the use of restraint, seclusion and restrictive interventions while addressing racial disparities.
The presenters explained that restrictive practices are not experienced equally across all communities. Evidence shows that people from some racialised groups are more likely to experience restrictive interventions, making this both a safety issue and a race equity issue. Oxleas therefore sought to identify practical actions that could improve care while simultaneously reducing inequalities.
Listening to Staff and Stakeholders
As part of their PCREF work, Oxleas engaged staff, service users and stakeholders to identify priorities for change. The feedback was grouped and ranked to establish the strongest starting points for improvement.
The consultation identified two immediate workstreams:
- Debrief and Escalation
- Trauma-Informed Care
The presentation emphasised that participants did not ask for abstract policy changes. Instead, they identified practical improvements that could be implemented directly within services.
Highest-Ranked Priorities
The most frequently identified priorities included:
A key message from the slide was that stakeholders wanted changes that would directly affect day-to-day care, staff behaviour and patient experience.
Workstream One: Debrief and Escalation
The first workstream focused on reducing escalation in the moment and improving learning after incidents occur.
The framework was organised into three stages:
Before Escalation
Staff are encouraged to:
- Pause before escalating situations.
- Ensure one lead staff member takes responsibility.
- Consider alternatives earlier.
- Use an equity prompt before moving to hands-on interventions.
The emphasis was on slowing decision-making enough to ensure staff are responding to the person’s needs rather than reacting automatically.
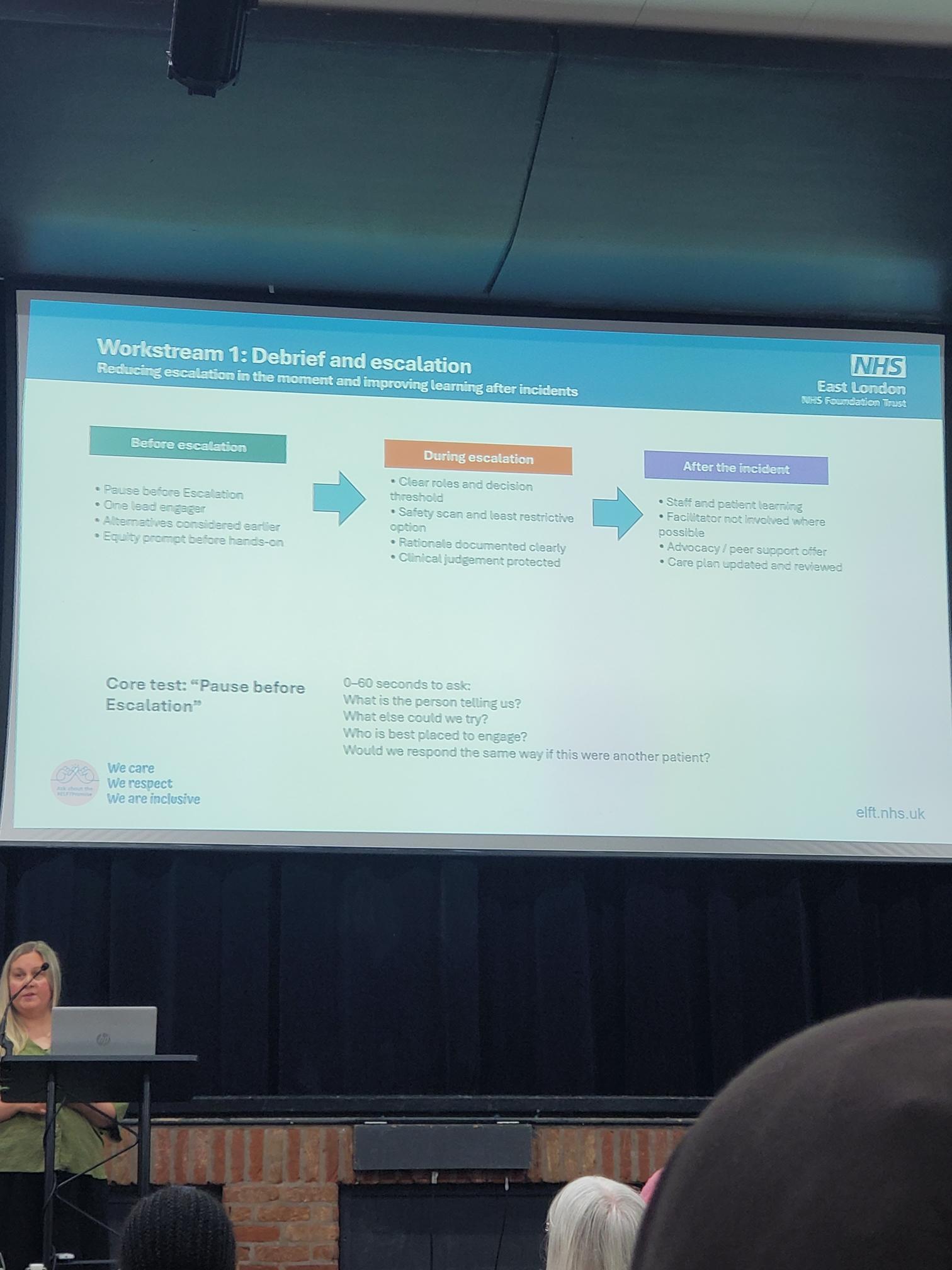
During Escalation
The presentation highlighted the importance of:
- Clear staff roles.
- Defined decision-making thresholds.
- Safety scanning.
- Choosing the least restrictive option available.
- Clear documentation of rationale.
- Protecting clinical judgement while maintaining accountability.
The objective is to ensure restrictive interventions are only used when absolutely necessary and are proportionate to the situation.
After the Incident
Learning after incidents was considered equally important.
Actions included:
- Joint staff and patient learning.
- Independent facilitation where possible.
- Advocacy and peer support.
- Reviewing and updating care plans.
The focus was not simply on recording incidents but on understanding what happened and preventing repetition.
Next Steps
The presentation concluded with a clear action plan for the coming period.
Planned Actions
- Agree a Trust-wide escalation and post-incident learning standard.
- Begin testing the “Pause Before Escalation” approach on selected wards.
- Finalise a Trust Trauma-Informed Care (TIC) protocol and minimum training standard.
- Strengthen dashboard reporting and improve protected-characteristics data quality.
- Embed lived experience into the design and review of changes.
These actions reflect the Trust’s commitment to moving from discussion to implementation.
Learning Across London
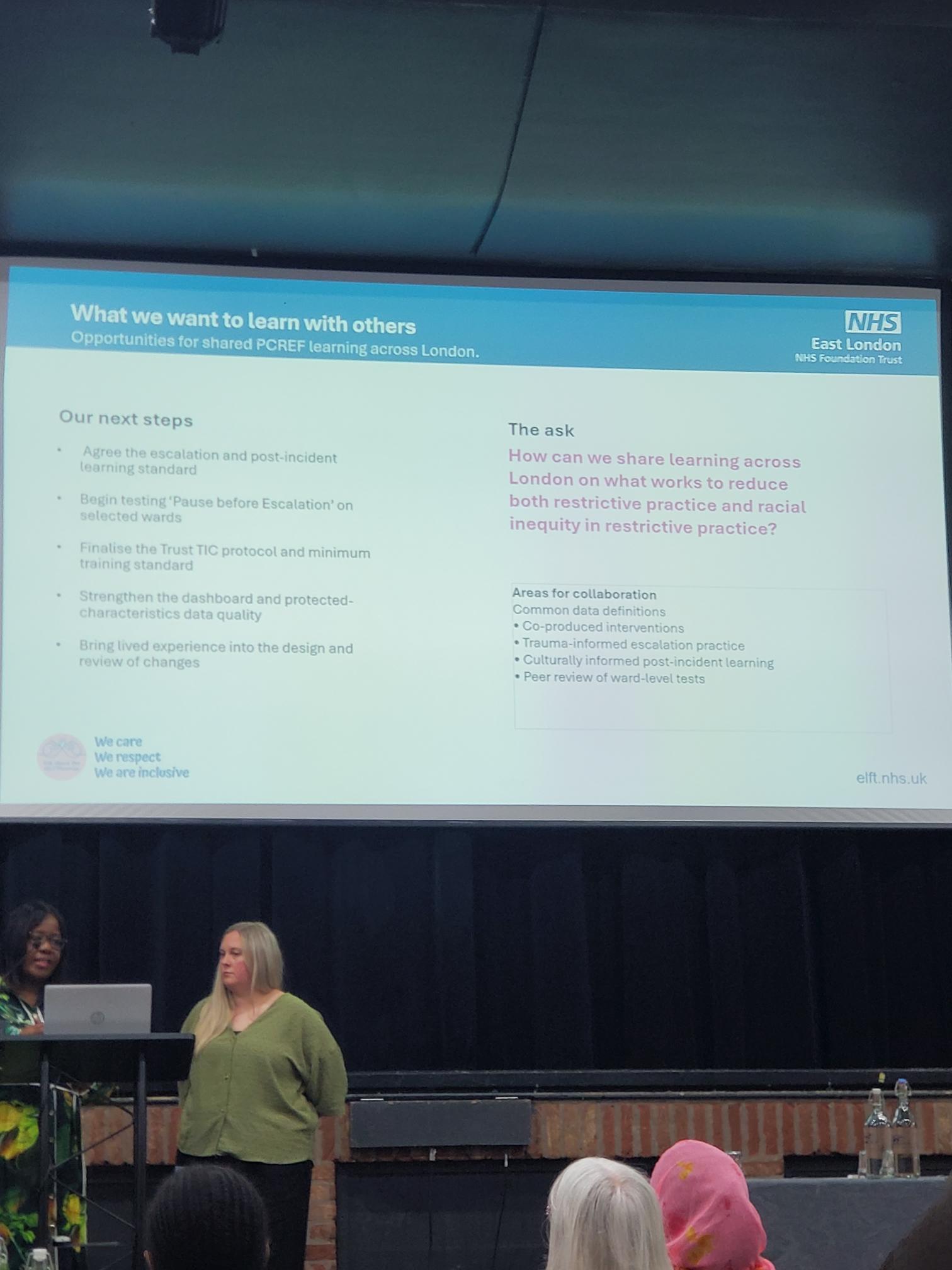
The presenters also highlighted the importance of collaboration across London’s mental health trusts.
Areas identified for collaboration included:
- Common data definitions.
- Co-produced interventions.
- Trauma-informed escalation practice.
- Culturally informed post-incident learning.
- Peer review of ward-level improvement projects.
This reflected one of the key themes running throughout the conference: that race equity work is strengthened when trusts learn from each other rather than working in isolation.
North East London NHS Foundation Trust (NELFT)
North East London NHS Foundation Trust (NELFT) presented its PCREF work through the lens of national competencies, demonstrating how race equity can be embedded into everyday clinical practice rather than being treated as a standalone initiative. The presentation, delivered by Erica Deti, Patient and Carer Race Equality Lead, highlighted the importance of developing a workforce that is confident, culturally competent and able to respond effectively to the needs of diverse communities. NELFT emphasised that meaningful change requires organisations to move beyond awareness and into practical action, ensuring that race equity is reflected in leadership, service design and frontline care.
A key focus of the presentation was the development and implementation of national PCREF competencies, designed to support staff at all levels in understanding racial inequalities and their impact on mental health outcomes. Erica explained how these competencies help staff build the knowledge, skills and confidence needed to challenge inequity, engage meaningfully with service users and carers, and contribute to culturally responsive services. The Trust also stressed the importance of involving people with lived experience throughout this process, ensuring that learning is informed by real experiences rather than theoretical concepts alone.
The presentation reinforced the message that achieving race equity is a continuous journey rather than a destination. NELFT shared examples of how the Trust is embedding co-production, reflective practice and accountability into its approach, while encouraging staff to consider how their decisions influence patient experiences and outcomes. By focusing on workforce development, lived experience leadership and organisational learning, NELFT demonstrated how PCREF can act as a catalyst for long-term cultural change, helping to create services that are safer, fairer and more responsive to the communities they serve.
A second NELFT presentation was delivered from local community organisations and Project Zero. This session focused on partnership working with local barbershops, voluntary organisations and community groups as a means of improving engagement with racialised communities. The speakers described how trusted community settings can help bridge gaps between services and populations that may feel excluded from traditional healthcare pathways.

Carer Spotlight
Matthew McKenzie and PCREF Carer Poetry
One of the most powerful moments of the afternoon came during the Carer Spotlight, where carers used poetry to share personal experiences of supporting loved ones through mental health services. The session moved beyond statistics, policies and organisational frameworks to remind attendees of the human stories that sit behind every discussion about race equity, access and care. The poetry was delivered by Matthew McKenzie and fellow carers, creating a reflective and emotional space that grounded the conference in lived experience. Through spoken word and personal reflection, the audience was invited to consider what it truly means to care, advocate and persevere within systems that do not always recognise the voices of carers.
A recurring theme across the poems was the often invisible role of carers. Several pieces explored the emotional labour involved in supporting a family member through periods of crisis, while also navigating complex services and systems.
Here is the poem from Matthew McKenzie taken from his collaborative book (in development) – Unpaid, Unseen and Yet Unbroken
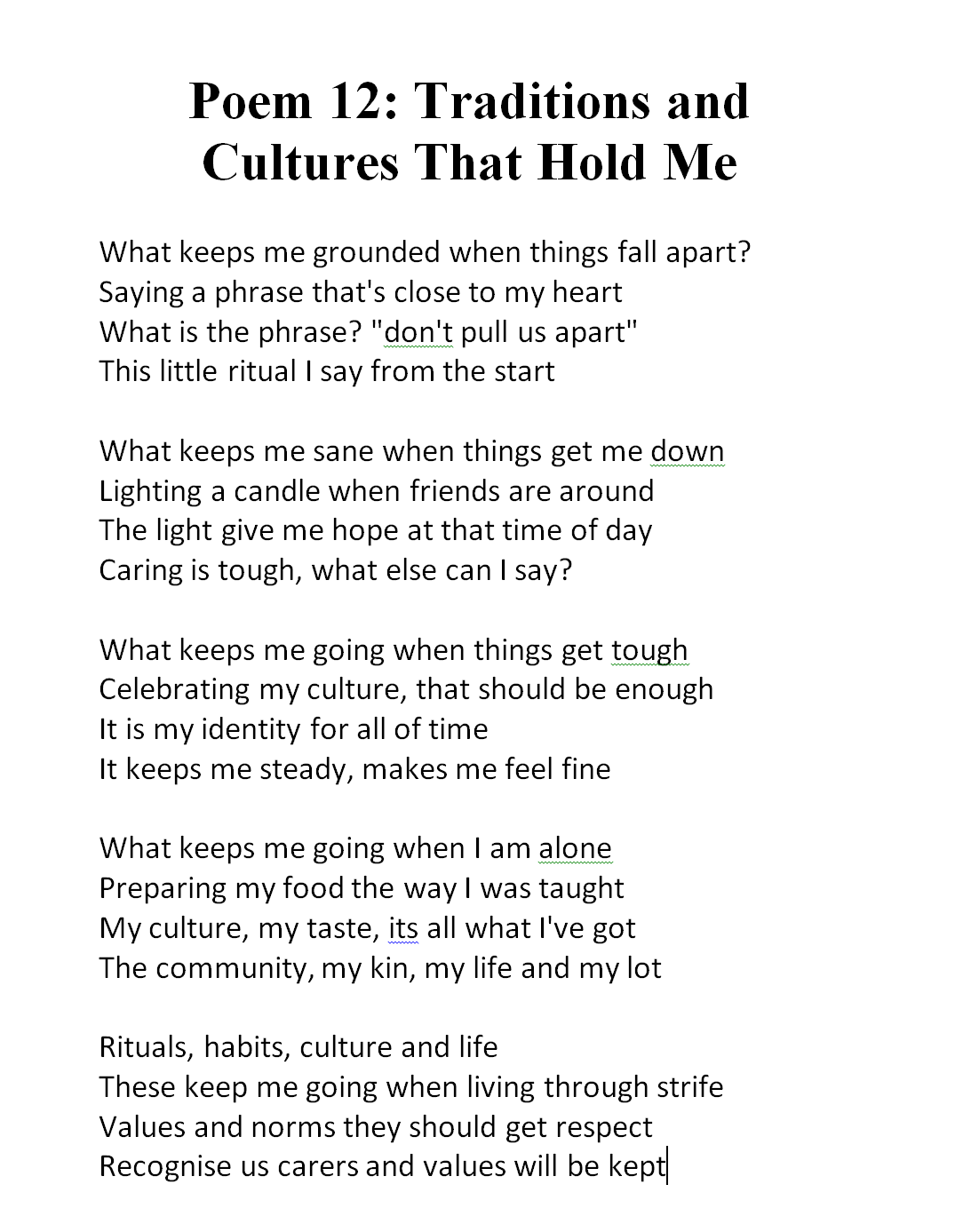
The poems highlighted feelings of exhaustion, responsibility and uncertainty, but also resilience and determination. Listeners heard about the challenges of balancing personal wellbeing with caring responsibilities, and the reality that carers frequently become experts in supporting their loved ones while receiving little recognition themselves. The poetry gave voice to experiences that are often hidden from formal reports and performance data, yet have a profound impact on individuals and families.

Another important theme was the need for genuine partnership between services, service users and carers. The poems reflected frustrations when carers felt excluded from conversations, ignored during decision-making or treated as outsiders despite their deep understanding of the person they support. At the same time, they celebrated examples of compassionate practice, where professionals listened, worked collaboratively and recognised carers as valuable partners in recovery. These reflections connected strongly with the wider messages of PCREF, reinforcing that co-production is most effective when carers are respected, included and treated as equal contributors rather than passive observers.
Central and North West London NHS Foundation Trust (CNWL)
Presented by J’nelle James, Acting Assistant Director of Culture and Equality, Diversity and Inclusion, Central and North West London NHS Foundation Trust (CNWL) showcased one of the conference’s most innovative examples of co-production through the Black Men’s Wellbeing Festival 2026. The presentation focused on how Milton Keynes Talking Therapies worked with Black men, community leaders and local organisations to improve engagement with NHS mental health services. Rather than expecting communities to come to services, CNWL demonstrated how services can go out into communities, build relationships and create spaces where conversations about mental health feel safe, relevant and culturally meaningful.
The presentation explained that the project began during Black History Month in October 2022, when Milton Keynes Talking Therapies hosted a free face-to-face wellbeing session for Black men at Stantonbury Health Centre. The event explored themes including racial trauma, stigma, family relationships, cultural influences and self-worth. What began as a single wellbeing session quickly revealed a significant unmet need within the community. Participants spoke openly about barriers to accessing support and the lack of culturally relevant mental health conversations, leading the team to recognise that a longer-term programme of engagement was needed.
CNWL emphasised that trust cannot be created through a single event or consultation exercise. Instead, trust is earned through visibility, consistency and genuine partnership. The Trust described a three-year journey of listening, learning and working alongside local communities, which ultimately led to the development of the Black Men’s Wellbeing Festival. The project became an example of how PCREF principles can be applied in practice by ensuring that communities are involved in shaping solutions rather than simply being consulted after decisions have already been made.
Building Trust Through Co-Production
A central message throughout the presentation was that “trust isn’t built overnight.” The festival emerged through a deliberate process of relationship-building and community engagement. CNWL outlined six stages that helped transform an initial wellbeing event into a large-scale community-led initiative.

The first stage focused on initial engagement, beginning with the October 2022 wellbeing session. Following this, the team moved into a listening and learning phase, hosting webinars, training sessions and community discussions to understand what Black men wanted from mental health services. Rather than assuming solutions, the Trust spent time listening to experiences and identifying priorities directly from community members.
The next stages involved meeting people in community spaces, strengthening relationships with local organisations and businesses, amplifying messages through trusted community networks and broadening engagement across Milton Keynes. The presentation highlighted that every stage was developed collaboratively with community partners, ensuring that ownership of the programme remained shared rather than NHS-led.
Key Stages of the Journey
- Initial engagement through Black History Month wellbeing events.
- Listening sessions and community conversations.
- Presence at local community gatherings and celebrations.
- Building partnerships with local organisations and businesses.
- Using trusted networks to amplify messages.
- Expanding engagement through media, events and outreach.
The Black Men’s Wellbeing Festival 2026
The culmination of this work was the launch of the Black Men’s Wellbeing Festival 2026, a community-led programme designed to improve access and engagement for Black men within mental health services. Running weekly between April and May 2026, the festival brought together clinicians, community leaders, lived experience speakers and local organisations to create open conversations about wellbeing, identity and mental health.
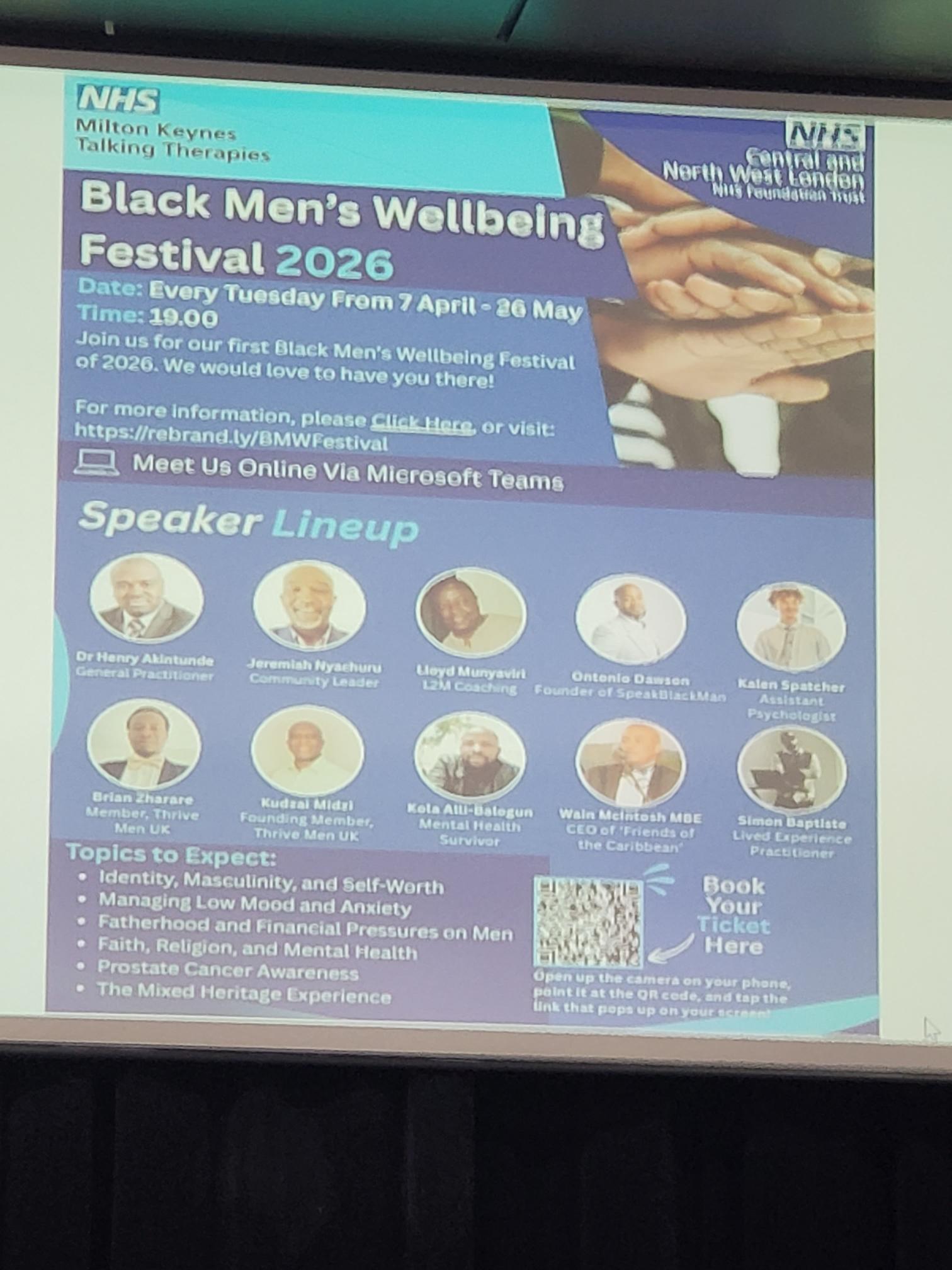
The programme tackled subjects that participants themselves had identified as important. Rather than focusing solely on clinical mental health conditions, the festival explored the wider social, cultural and personal experiences that influence wellbeing. This reflected a more holistic understanding of mental health and recognised that issues such as identity, masculinity, family expectations and discrimination all play an important role in people’s wellbeing.
The festival also demonstrated how NHS services can become more accessible when support is delivered in partnership with trusted community figures. By bringing together professionals and community leaders, CNWL created opportunities for conversations that may not otherwise take place within traditional healthcare settings.
North London NHS Foundation Trust
Equity and Health Inequalities Strategy 2026–2030: “Inclusion in Action”

North London NHS Foundation Trust presented its new Equity and Health Inequalities Strategy 2026–2030, centred on the theme of “Inclusion in Action.” The presentation highlighted the Trust’s ambition to embed equity into every aspect of organisational culture, leadership, workforce development and service delivery. Rather than treating equality and health inequalities as separate workstreams, the strategy positions inclusion as a fundamental principle underpinning better mental health outcomes, improved staff experiences and stronger communities. The Trust’s vision was summarised through the phrase: “Better Mental Health. Better Lives. Better Communities.”
A key theme throughout the presentation was the recognition that addressing inequalities requires action at both organisational and system levels. The strategy aligns with the Trust’s broader five-year organisational goals and is supported by the North London Way, Trust values, leadership framework and staff network structures. The presenters emphasised that lived experience, staff insight and community partnership have been central to shaping the strategy, ensuring that it reflects the realities of the diverse populations served across North Central London.
The presentation also highlighted the importance of shared accountability. Equity was presented not as the responsibility of specialist equality teams alone, but as a collective responsibility across leadership, clinical services, operational teams and partner organisations. Through this approach, the Trust aims to create sustainable cultural change while reducing inequalities experienced by both service users and staff.
Strategic Ambitions and Organisational Change
A major focus of the presentation was how the Trust intends to turn principles into practical action. The strategy builds upon existing organisational priorities while introducing a stronger and more explicit focus on equity and inclusion. The presenters described a framework that links the Trust’s strategic aims, leadership expectations, workforce culture and service improvement activity into a single coherent approach.

The strategy is closely connected to the work of the Staff Networks Alliance, which brings together a range of staff networks representing diverse communities and experiences. The Trust described these networks as essential partners in shaping policy, challenging inequalities and ensuring that organisational decisions are informed by lived experience. This collaborative model reflects a commitment to co-production and shared leadership rather than top-down decision making.
The presentation emphasised a set of organisational values that support inclusive practice, including visibility, accountability, compassion, collaboration and empowerment. These principles are intended to guide both staff behaviour and organisational decision-making. By embedding these values throughout the Trust, leaders hope to create a culture where inclusion becomes a routine part of everyday practice rather than a separate programme of work.
Building on Existing Foundations
The final section of the presentation focused on progress already achieved and the foundations that have been established to support future work. The Trust outlined a number of significant developments, including the creation of an Equality, Diversity and Inclusion (EDI) Programme Board, which provides governance and oversight for inclusion and health inequalities initiatives. This governance structure helps ensure that equity remains a strategic priority and is monitored at senior levels of the organisation.
The Trust has also introduced several initiatives aimed at strengthening accountability and supporting underrepresented groups. These include the launch of the Staff Networks Alliance, the development of anti-racism principles, positive action programmes, reciprocal mentoring opportunities and improvements in disability inclusion through the Reasonable Adjustments Passport scheme. The Trust reported achieving Disability Confident Level 2 status, reflecting progress in creating a more inclusive workplace environment.
Importantly, the presentation highlighted the implementation of the Patient and Carer Race Equality Framework (PCREF) as a key mechanism for advancing anti-racist practice and addressing inequalities within mental health pathways. Alongside embedding the North London Way as a shared organisational framework, the Trust views PCREF as a central component of its strategy for reducing inequities and improving outcomes. The overall message was that meaningful progress has already begun, but sustained effort, partnership and accountability will be required to achieve the ambitions set out in the Equity and Health Inequalities Strategy 2026–2030.
A recurring message from the closing discussion was that race equity remains everybody’s responsibility. While significant progress has been made, panellists acknowledged that much work remains. Delegates left with a renewed commitment to collaboration, stronger partnerships with carers and communities, and a shared determination to ensure that PCREF continues to drive meaningful and measurable change across London’s mental health services.