By Matthew McKenzie – Carers UK ambassador / Chair of National ethnic mental health carers forum
Are you a Black unpaid carer supporting a family member with a learning disability (sometimes referred to as an intellectual disability) who has experienced mental health difficulties?
Have you ever tried to access mental health support on their behalf? This could include contacting services such as Community Learning Disability Teams, CAMHS, Community Mental Health Teams, Talking Therapies or other mental health services.
If so, your experiences matter.
Lauren Heath, a second-year Trainee Clinical Psychologist at the University of Southampton, is conducting doctoral research exploring the experiences of Black carers who have accessed, or attempted to access, mental health support for a family member with a diagnosed learning disability.
We know that Black unpaid carers often face additional challenges when trying to navigate health and social care systems. Too often, their experiences are unheard or underrepresented in research. This study aims to better understand those experiences and help inform more culturally sensitive and inclusive services in the future.
You may be eligible to take part if you:
Identify as Black.
Have significant caring responsibilities for a family member with a diagnosed learning disability (or intellectual disability).
Have accessed, or attempted to access, mental health services on their behalf.
Taking part will involve:
A confidential interview lasting approximately 1.5 hours via Microsoft Teams.
Your responses will be anonymised once all interviews have been completed.
You will receive a voucher to thank you for your time and contribution.
Lauren previously worked within Community Learning Disability Teams across the UK and became interested in understanding why so few Black families appeared to be accessing these services. Her doctoral research hopes to amplify the voices of Black carers and contribute towards improving culturally sensitive support for families in the future.
If you think this research may apply to you, or someone you know, please consider taking part or sharing this opportunity within your networks.
To find out if you are eligible, you can complete the short questionnaire or contact Lauren directly at L.Heath@soton.ac.uk.
Your lived experience could help shape future services for Black families and carers.
By Matthew McKenzie – Triangle of Care – Community group chair
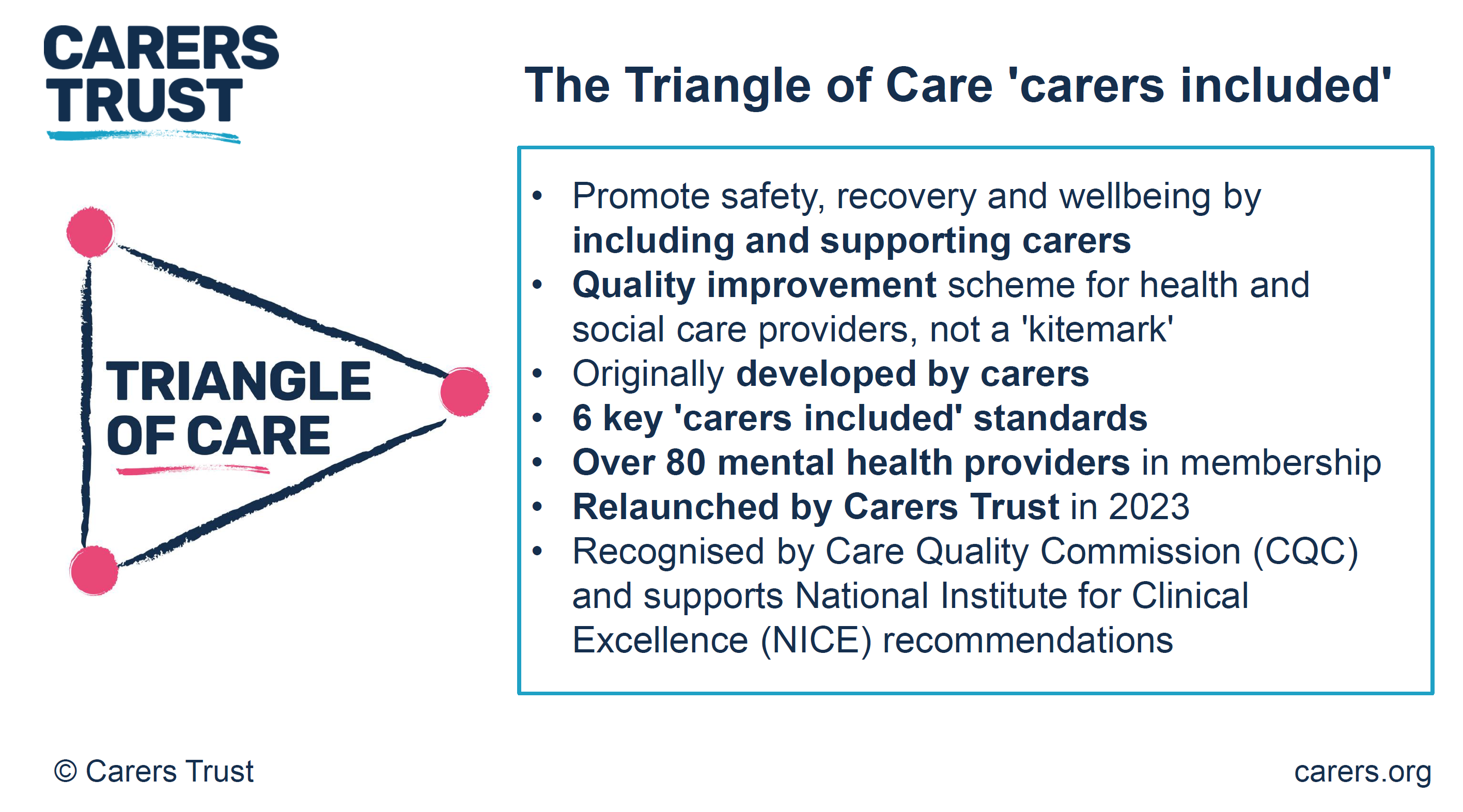
Putting Carers at the Centre of Care
The latest Triangle of Care Community Group brought together carers, professionals and partner organisations from across England to share learning, celebrate progress and identify where further improvements are needed. The meeting highlighted the growing influence of the Triangle of Care across mental health and acute services, whilst reinforcing that there is still much work to do to ensure carers are consistently recognised, valued and supported.
One of the most powerful aspects of the meeting was hearing directly from carers about their experiences. Whilst many spoke positively about the progress that has been made over recent years, there was a shared view that carer involvement remains inconsistent across services. Carers described feeling more included than ever before, with greater awareness of the Triangle of Care principles and more opportunities to participate in steering groups, service developments and community discussions. However, concerns remain around automatic carer identification, information sharing and ensuring that carers are genuinely recognised as partners in care.
Several carers reflected on the importance of having their voices heard early in a patient’s care journey. Examples were shared of services introducing carer contribution templates that ensure family members are involved within 72 hours of admission, whilst others highlighted improvements to confidentiality processes that allow patients to determine what information can be shared with carers at different stages of their recovery. These practical changes demonstrate how relatively small adjustments can have a significant impact on relationships between carers, patients and professionals.
Progress Across the Triangle of Care Programme
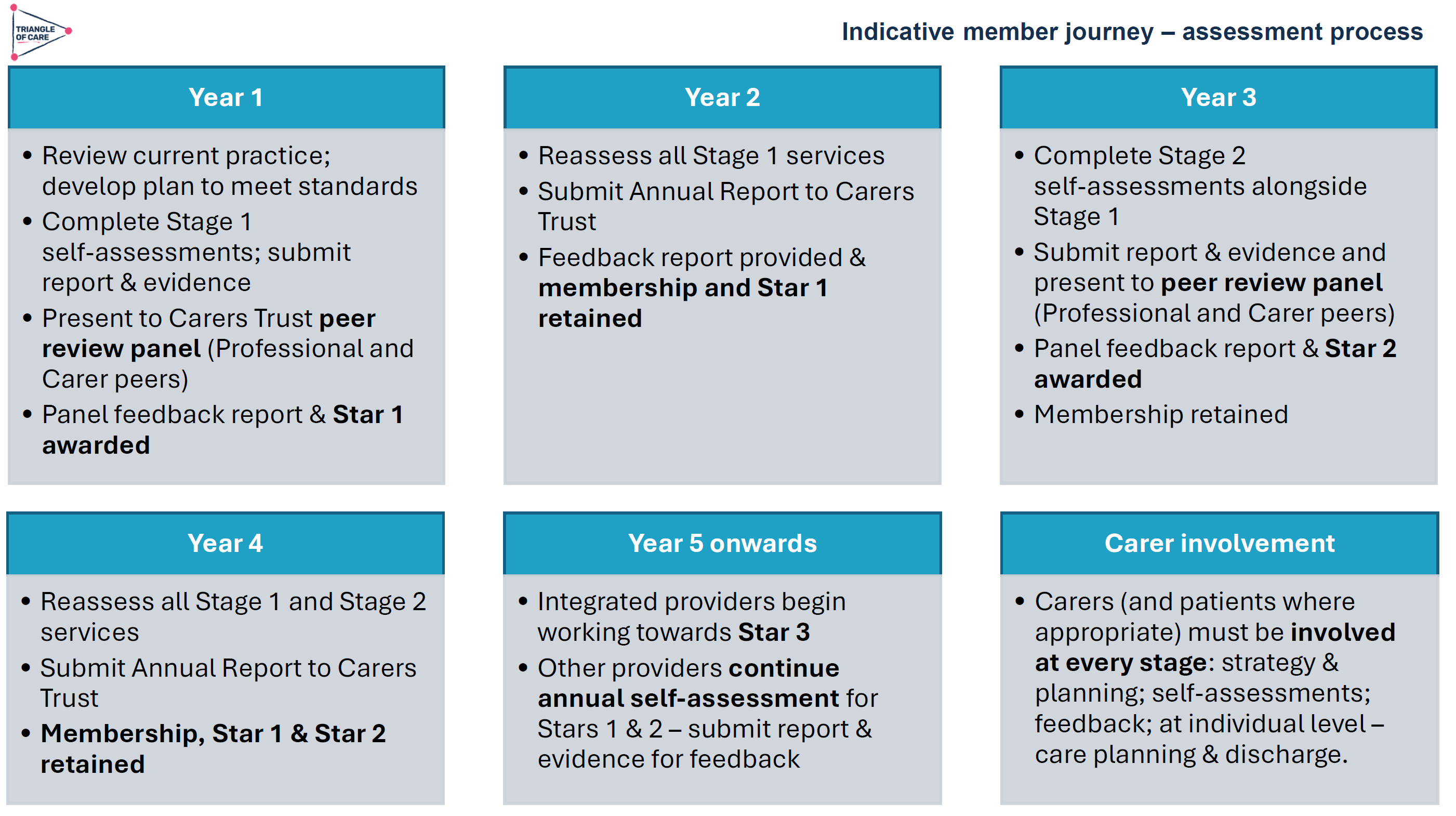
Mary Patel, Triangle of Care Programme Lead at Carers Trust, provided an update on developments across the national programme. The Triangle of Care continues to grow, with a number of organisations progressing through the STAR accreditation process and demonstrating their commitment to embedding carer-inclusive practice across services.
Importantly, members were reminded that the STAR awards are not designed to rank organisations, but instead reflect the breadth of implementation across different service areas. STAR I focuses primarily on inpatient and crisis services, STAR II expands into community services, whilst STAR III recognises organisations delivering integrated services across multiple clinical areas.
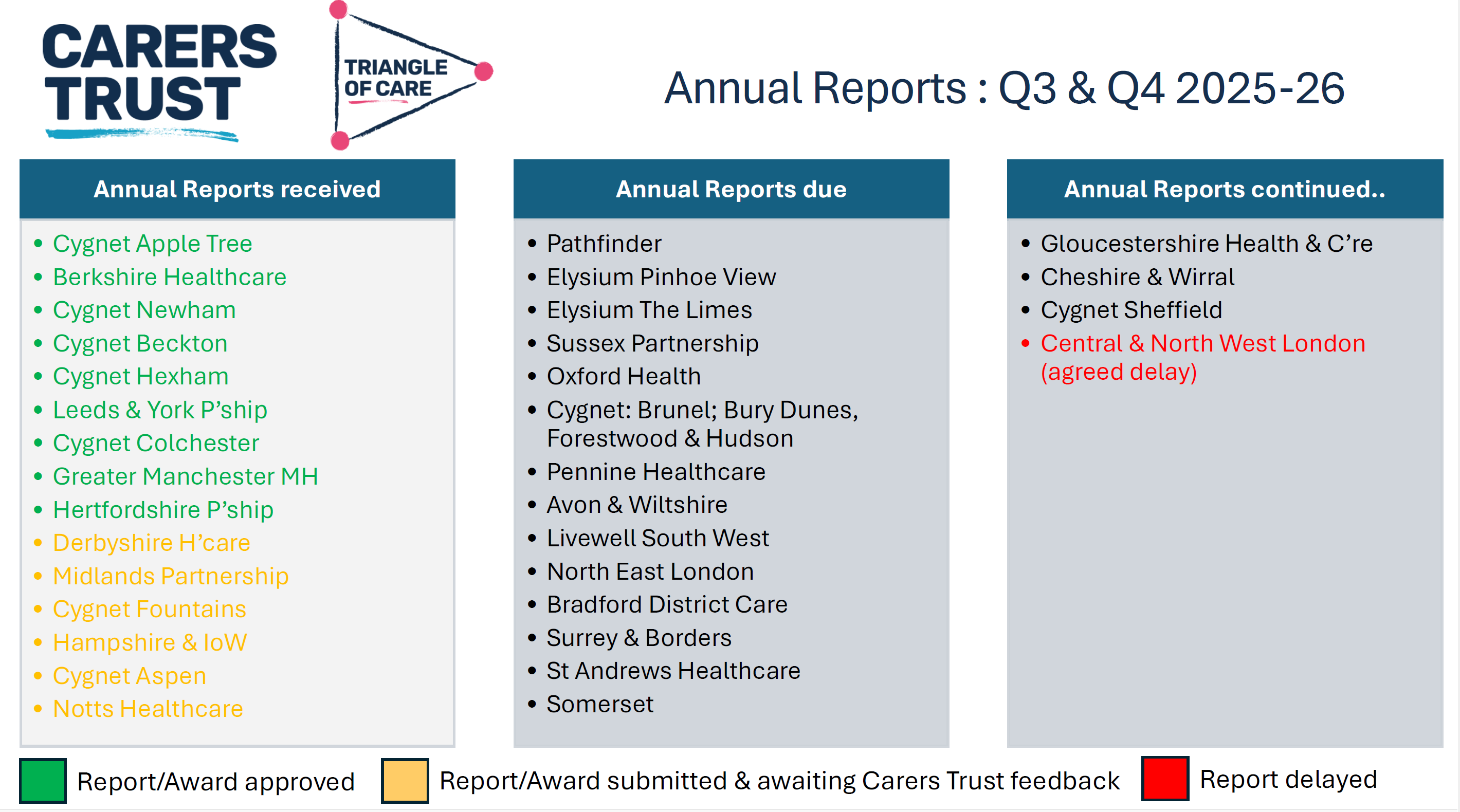
Several trusts have recently achieved STAR awards, whilst others are progressing through the assessment process over the coming months. The programme’s peer review approach continues to ensure that carers remain central to the assessment process, with carers actively involved in reviewing evidence, identifying good practice and making recommendations for future development.
The Triangle of Care Member Hub continues to provide valuable opportunities for peer learning, resource sharing and collaborative working. Upcoming webinars will include sessions exploring Open Dialogue approaches developed by Devon Partnership NHS Trust, providing members with further opportunities to learn about therapeutic models that place families and carers at the heart of care planning.
Advancing Equality Through the Patient and Carer Race Equality Framework
A significant development announced during the meeting was the launch of Phase Two of the Triangle of Care and Patient and Carer Race Equality Framework (PCREF) project.
PCREF represents the first mandatory anti-racism framework within mental health services in England. Recognising that carers from racially marginalised communities often experience poorer outcomes and face additional barriers when accessing support, the Triangle of Care programme has been working collaboratively with carers and mental health providers to strengthen the way services assess and respond to carers’ needs.
The revised self-assessment framework encourages services to move beyond assumptions and adopt a more professionally curious approach to understanding carers’ individual experiences. Rather than viewing carers as a homogenous group, the framework recognises that caring experiences are shaped by culture, identity, language, personal circumstances and wider health inequalities.
Pilot sites from across England are now testing the revised guidance, with learning being shared nationally throughout the project. Importantly, organisations do not need to be participating in the pilot to begin implementing the principles and learning that emerge from this work.
Alongside PCREF, Carers Trust continues to contribute to national policy developments, including the Modern Service Framework for Severe Mental Illness and the forthcoming Mental Health Strategy for England. Throughout these discussions, there has been a consistent message that carers must be recognised as partners in care and have access to appropriate support in their own right.
Confidentiality, Information Sharing and Carer Inclusion
Confidentiality remained one of the most prominent themes throughout the meeting. Whilst participants acknowledged the importance of protecting patients’ rights and preferences, carers highlighted that confidentiality can sometimes become a barrier to meaningful engagement.
Several contributors reflected that confidentiality should never prevent professionals from listening to carers’ concerns or receiving valuable information that may support a patient’s care. Others spoke about the importance of revisiting conversations around consent over time, recognising that patients’ preferences may change as their circumstances and wellbeing improve.
Practical examples of good practice included breaking confidentiality discussions down into specific areas, allowing patients to decide what information can be shared about medication, activities, wellbeing and treatment plans, rather than relying on simple ‘yes or no’ decisions. There was also discussion around the importance of staff training to improve confidence when navigating complex conversations around confidentiality and information sharing.
Participants agreed that carers should never be expected to provide significant levels of support without receiving the information necessary to do so safely and effectively. Achieving the right balance between confidentiality and partnership working remains an important priority for the Triangle of Care community.
Triangle of Care Principles Within Acute Services
The meeting concluded with an inspiring presentation from Wendy Doyle, Head of Patient Experience at St George’s University Hospitals NHS Foundation Trust and Epsom and St Helier Hospitals, exploring how Triangle of Care principles can be successfully implemented within acute hospital settings.
Whilst the Triangle of Care originated within mental health services, Wendy demonstrated that its principles are equally applicable across acute care environments. Her organisation supports approximately 19,000 members of staff across multiple hospital sites and has developed a comprehensive approach to identifying, recording and supporting unpaid carers.
Staff are encouraged to identify carers at the earliest possible opportunity, with this information recorded within patient records to ensure continuity throughout the patient’s hospital journey. Comprehensive carer awareness training is delivered through virtual sessions, ward-based education and e-learning resources, helping staff understand both the practical and emotional importance of recognising carers.
Importantly, identifying carers is only the beginning of the process. Every carer recorded within the hospital system receives a follow-up wellbeing check from the Patient Experience Team to discuss their own support needs, identify any challenges and facilitate referrals to local carers’ organisations where appropriate.
Partnership working sits at the heart of this approach, with close collaboration between acute services and local carers’ centres ensuring carers can access a broad range of practical and emotional support. Adult and Young Carers’ Charters have also been co-produced with carers themselves, helping to shape organisational commitments around kindness, inclusion and meaningful engagement.
Perhaps most importantly, Wendy highlighted that supporting carers improves outcomes for everyone. Better communication strengthens discharge planning, reduces avoidable hospital admissions and readmissions, improves patient safety and helps prevent carer burnout. Acute hospital stays can provide valuable opportunities to identify carers who may previously have remained invisible and connect them with longer-term support.
Looking Ahead
The discussions throughout the meeting demonstrated both the progress that has been made and the challenges that remain. There is increasing recognition that carers are essential partners in delivering high-quality care across both mental health and acute services. However, meaningful involvement cannot rely upon individual goodwill alone; it requires consistent systems, robust policies and a genuine commitment to partnership working.
Looking ahead, the Triangle of Care programme will continue to expand opportunities for peer learning, influence national policy developments and support organisations to embed carer-inclusive practices across services. The ongoing work around PCREF and wider mental health policy developments provide important opportunities to ensure that carers’ voices remain central to future service transformation.
Above all, the meeting reinforced a simple but powerful message: carers must not be viewed as an afterthought or an optional addition to care planning. They are experts through experience, invaluable partners in care and individuals with support needs of their own. When carers are identified early, listened to meaningfully and supported appropriately, outcomes improve not only for carers themselves, but for patients, families and services alike.
The Triangle of Care Community Group continues to provide an important space where carers and professionals can learn from one another, challenge existing practices and work collectively towards more compassionate, inclusive and effective care.
On Wednesday 3 June 2026, colleagues from all eight London Mental Health Trusts, alongside carers, service users, community organisations, researchers, regulators and system leaders, gathered at ISH Venues in central London for the Pan London Patient and Carer Race Equality Framework (PCREF) Conference.
Chaired by Erica deti from North East London NHS Foundation Trust (NELFT), the conference provided a unique opportunity to showcase progress, share learning and strengthen London’s collective commitment to race equity within mental health services.
The conference was built around the principle that advancing race equity requires both organisational commitment and meaningful partnership with people who use services, carers and communities. Throughout the day, speakers challenged delegates to move beyond discussion and towards action, recognising that the inequalities experienced by racialised communities within mental health services remain one of the most significant challenges facing the NHS.
South West London and St George’s Mental Health NHS Trust
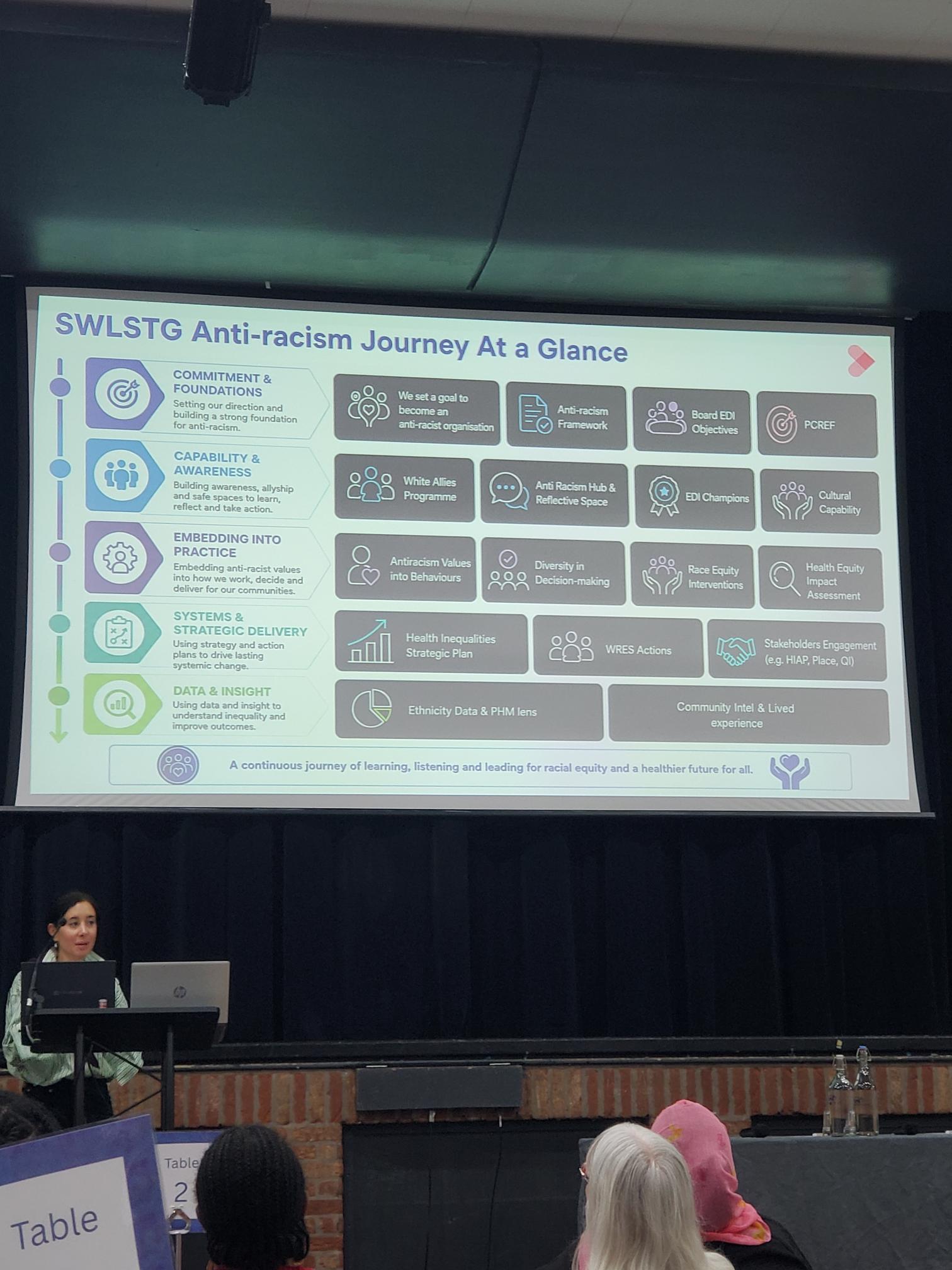
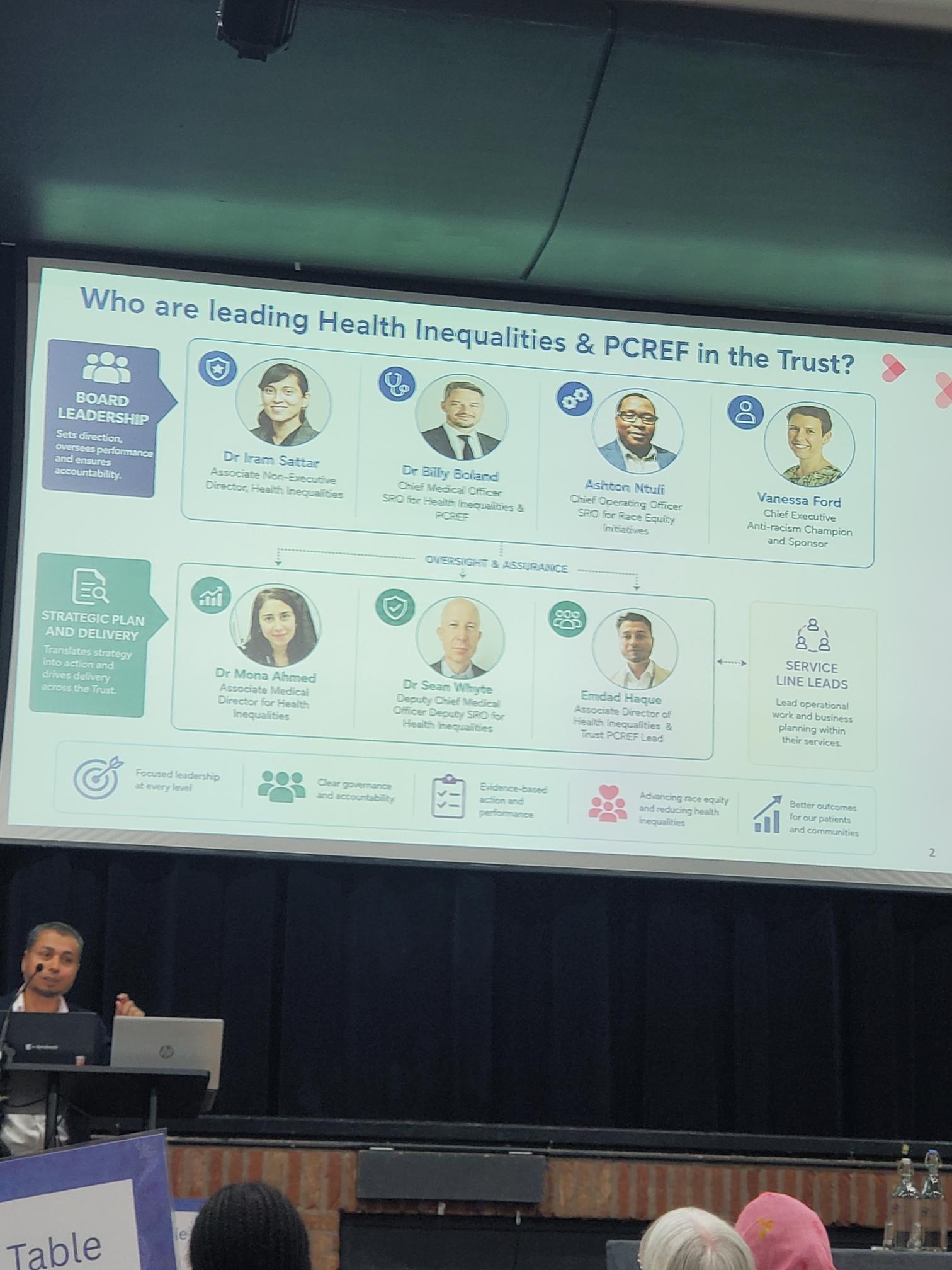
The first trust presentation was delivered by Amdad Ibrahim, Associate Director of Health Inequalities, and Dr Mona Dhesi, Consultant Forensic Psychologist and Associate Medical Director at South West London and St George’s Mental Health NHS Trust. Their presentation provided one of the clearest examples of how PCREF can be fully integrated into organisational strategy. Beginning with an explicit acknowledgement that racism exists within healthcare organisations and wider society, they demonstrated how their trust had used this recognition as the foundation for meaningful action.
The speakers outlined a comprehensive anti-racism programme linking governance, workforce development, community engagement and service transformation. Race equity has been embedded into business planning, leadership accountability and quality improvement processes, supported by cultural capability programmes, anti-racism steering groups and health equity assessments.
Their presentation demonstrated how PCREF can become part of the organisational DNA of a trust rather than a standalone initiative and provided a practical blueprint for others seeking sustainable implementation.
1. Commitment and Foundations
The Trust began by establishing a clear organisational commitment to becoming an anti-racist organisation. This commitment is supported through a range of strategic frameworks and governance structures, including the Trust’s Anti-Racism Framework, Board Equality, Diversity and Inclusion objectives, and the implementation of the Patient and Carer Race Equality Framework (PCREF).
Speakers emphasised that meaningful progress begins with leadership acknowledging that racism exists within healthcare systems and taking responsibility for addressing it. This commitment has been reinforced at Board level and incorporated into wider organisational priorities to ensure race equity remains visible and accountable.
2. Capability and Awareness
Recognising that sustainable change requires learning and reflection, the Trust has invested heavily in developing staff awareness and cultural capability. This includes initiatives such as:
White Allies Programme
Anti-Racism Hub and Reflective Spaces
Equality, Diversity and Inclusion Champions
Cultural Capability Training
These programmes create opportunities for staff to develop a deeper understanding of race, culture, privilege and inequality while providing safe spaces for reflection and discussion. The aim is to move beyond awareness and support staff to actively challenge inequity within their daily practice.
3. Embedding Anti-Racism into Practice
SWLSTG has focused on ensuring anti-racist values are embedded within decision-making processes and clinical practice rather than existing solely within training programmes.
Key areas of work include:
Embedding anti-racist values into organisational behaviours
Increasing diversity within leadership and decision-making structures
Delivering targeted race equity interventions
Using Health Equity Impact Assessments to inform service development
The Trust highlighted how race equity considerations are now being incorporated into service redesign programmes, policy development and clinical pathways, ensuring that decisions are assessed for their potential impact on different communities.
East London NHS Foundation Trust (ELFT)
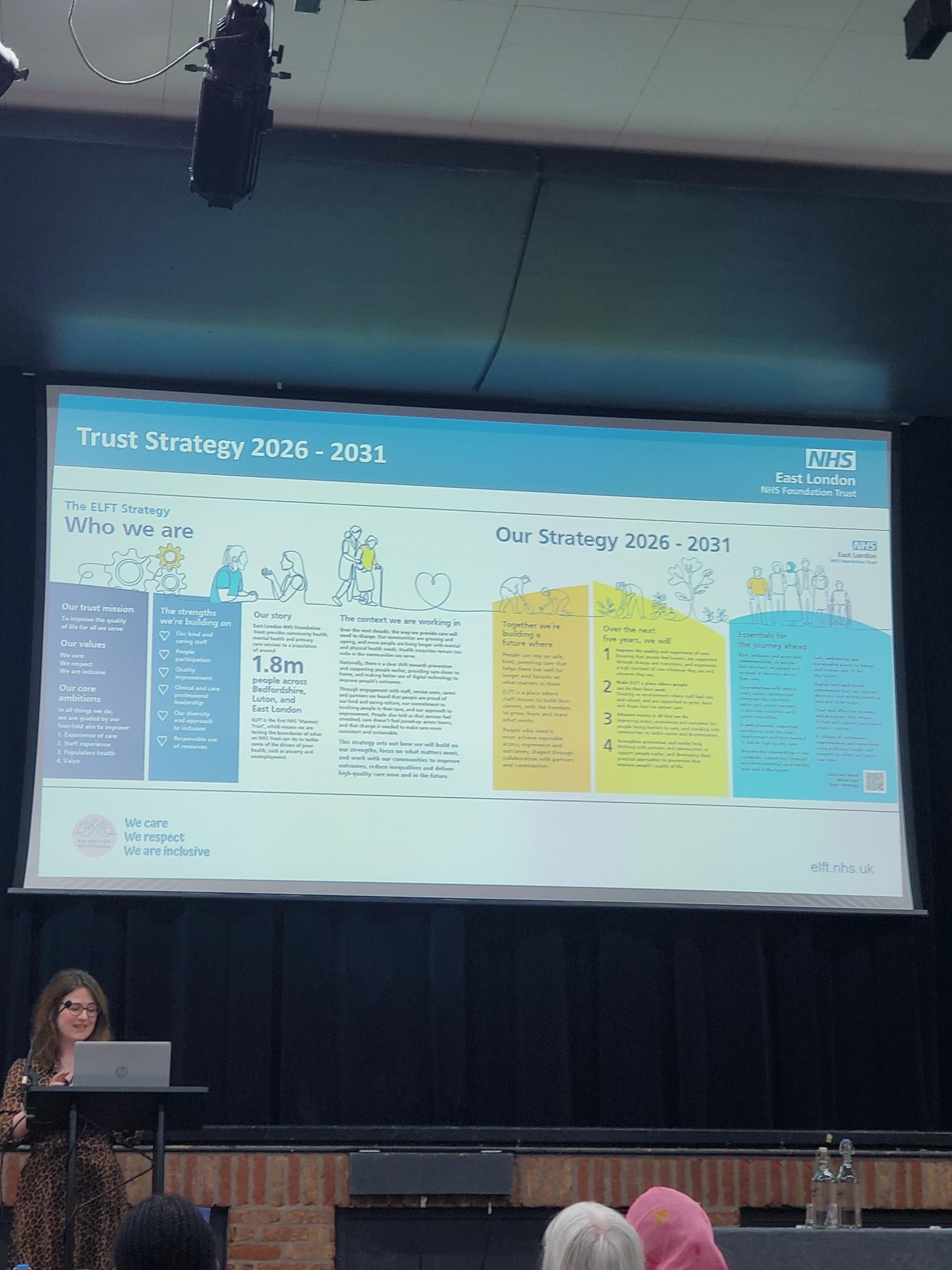
Advancing Equity in All That We Do: ELFT Strategy 2026–2031
Presented by Carrie Sissons, Deputy Director of Integrated Care, East London NHS Foundation Trust shared how race equity and inclusion have been embedded at the heart of the Trust’s new 2026–2031 Strategy. Rather than developing a strategy behind closed doors, ELFT undertook an extensive engagement programme designed to ensure that the voices of service users, carers, staff and communities directly influenced the Trust’s future direction.
Carrie explained that the strategy was developed during a period of significant challenge for health and care services, but also a period of opportunity. The Trust recognised that if it was to improve outcomes for the diverse communities it serves across East London, Bedfordshire and Luton, equity could not be treated as a separate programme of work. Instead, it had to become a core principle underpinning every decision, every service and every improvement initiative undertaken by the organisation.
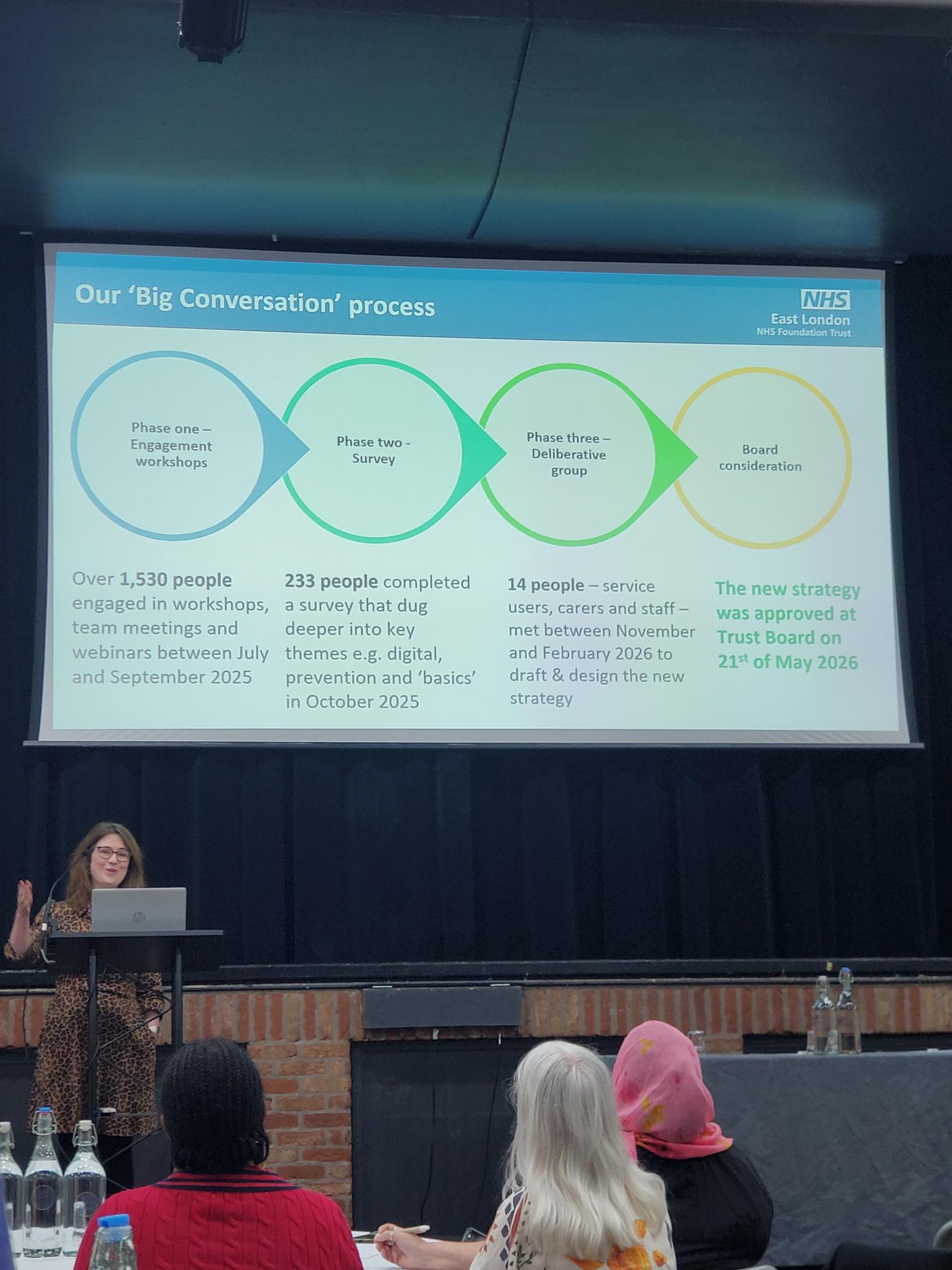
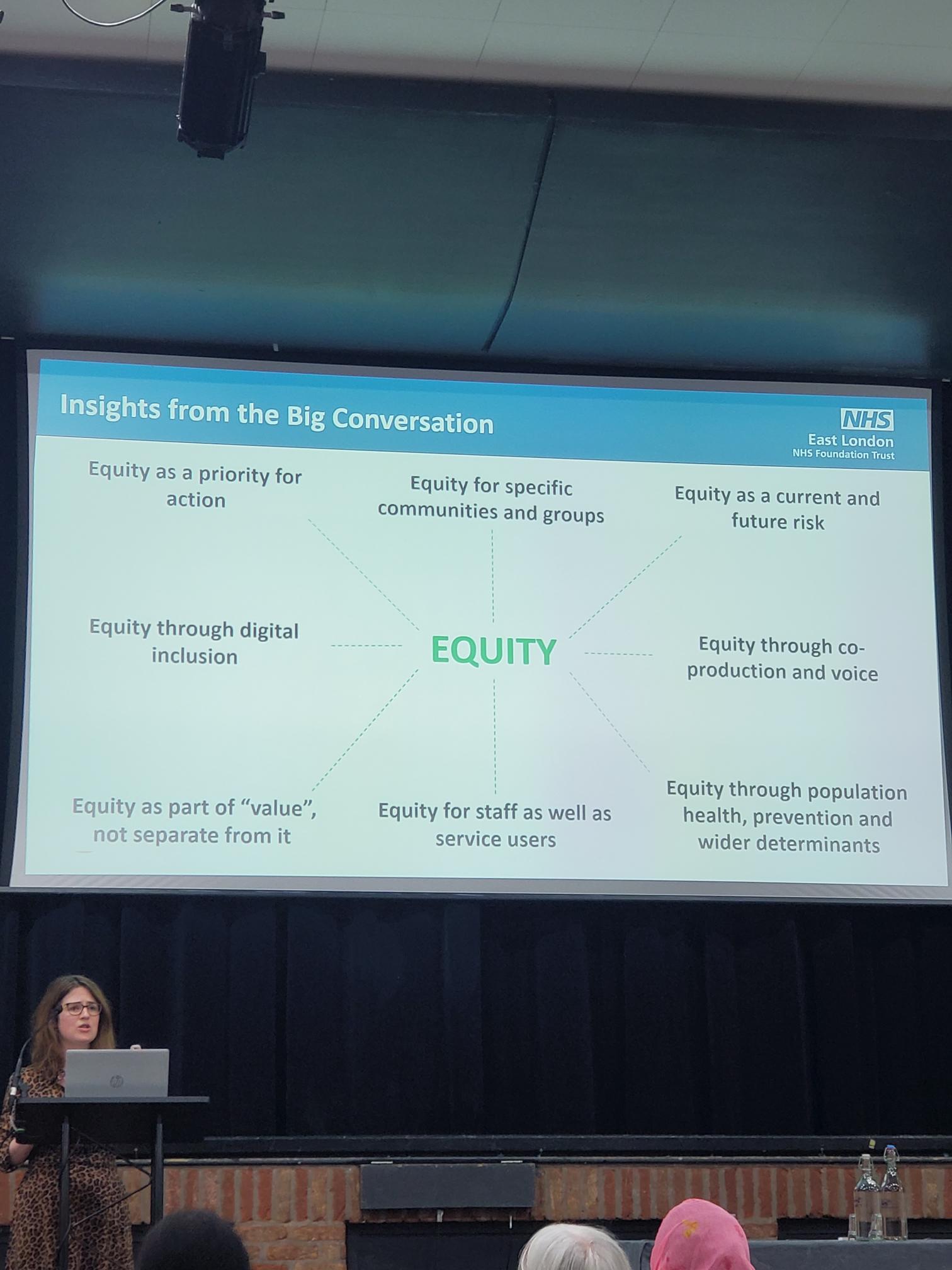
Building the Strategy Through the “Big Conversation”
A major feature of the strategy development process was the Trust’s extensive engagement exercise known as the “Big Conversation.” This programme was designed to ensure that the final strategy reflected the experiences, priorities and aspirations of the people who use and deliver services.
What People Told ELFT
One of the strongest messages emerging from the Big Conversation was the importance of equity. Participants consistently identified inequalities in access, experience and outcomes as issues that required sustained attention and action.
The engagement process highlighted several key themes:
Equity as a priority for action.
Equity for specific communities and groups.
Equity as a current and future risk.
Equity through co-production and lived experience.
Equity through population health and prevention.
Equity for staff as well as service users.
Equity through digital inclusion.
Equity as an essential part of value, not separate from it.
Carrie explained that these findings reinforced the need for equity to be visible throughout the Trust’s strategic objectives and operational plans. Participants wanted to see measurable action rather than broad commitments, with a focus on understanding and addressing disparities experienced by different communities.
The ELFT Strategy 2026–2031
The new strategy builds upon ELFT’s existing values and commitment to high-quality care. Serving approximately 1.8 million people across East London, Bedfordshire and Luton, the Trust recognised that reducing inequalities must remain central to its future ambitions.
The strategy identifies four broad priorities for the next five years:
Improve the quality and experience of care.
Make ELFT a great place to work.
Advance equity in all that we do.
Work with partners and communities to improve lives.
Of these priorities, the commitment to advancing equity was particularly relevant to the themes of the PCREF conference.
Priority Three: Advance Equity in All We Do
Carrie described this priority as a commitment to ensuring that equity becomes embedded within everyday practice rather than being treated as a specialist programme.
By 2031, ELFT aims to ensure that:
Teams routinely analyse access, experience and outcomes by population group.
Services take action when disparities are identified.
Progress continues against PCREF commitments.
The Trust’s Anti-Racism Plan and Charter are actively implemented.
Equity and inclusion are strengthened across the workforce.
Inequalities experienced by racialised communities are reduced.
The strategy recognises that data alone is not enough. Equity must be considered throughout service design, quality improvement, workforce development and organisational decision-making.
West London NHS Trust
Presented by Debbie Best (PCREF Lead), Natalie Mark (Living Experience PCREF Lead) and Dr Anne Aiyegbusi, West London NHS Trust delivered one of the most powerful and thought-provoking presentations of the conference. Their session focused on racial trauma, exploring how racism affects patients, carers and staff, and how organisations can create safe spaces to acknowledge, understand and respond to those experiences.
The presentation was rooted in the recognition that racial inequalities remain deeply embedded within mental health services. The team explained that their work developed in response to persistent concerns around disproportionate referrals, detention rates and restrictive interventions experienced by racialised communities. They also highlighted how mistrust of services and experiences of re-traumatisation continue to affect people’s willingness to engage with mental health support. Importantly, they stressed that racial trauma is not only experienced by service users but also by carers and staff, many of whom continue to navigate systems that can reproduce inequity.
Why This Work Matters
West London NHS Trust identified several key issues that informed the development of their racial trauma programme:
Disproportionate rates of referrals and detention among racialised communities.
Higher levels of restrictive interventions within mental health pathways.
Mistrust of services due to previous negative experiences.
The risk of re-traumatisation through interactions with healthcare systems.
The impact of racism on patients, carers and staff alike.
A particularly striking message from the presentation was that many racialised staff attending the workshops were not learning about racial trauma as a new concept. Instead, they were reflecting on experiences that formed part of their everyday reality. This observation reinforced the importance of creating environments where these experiences can be discussed openly and safely.
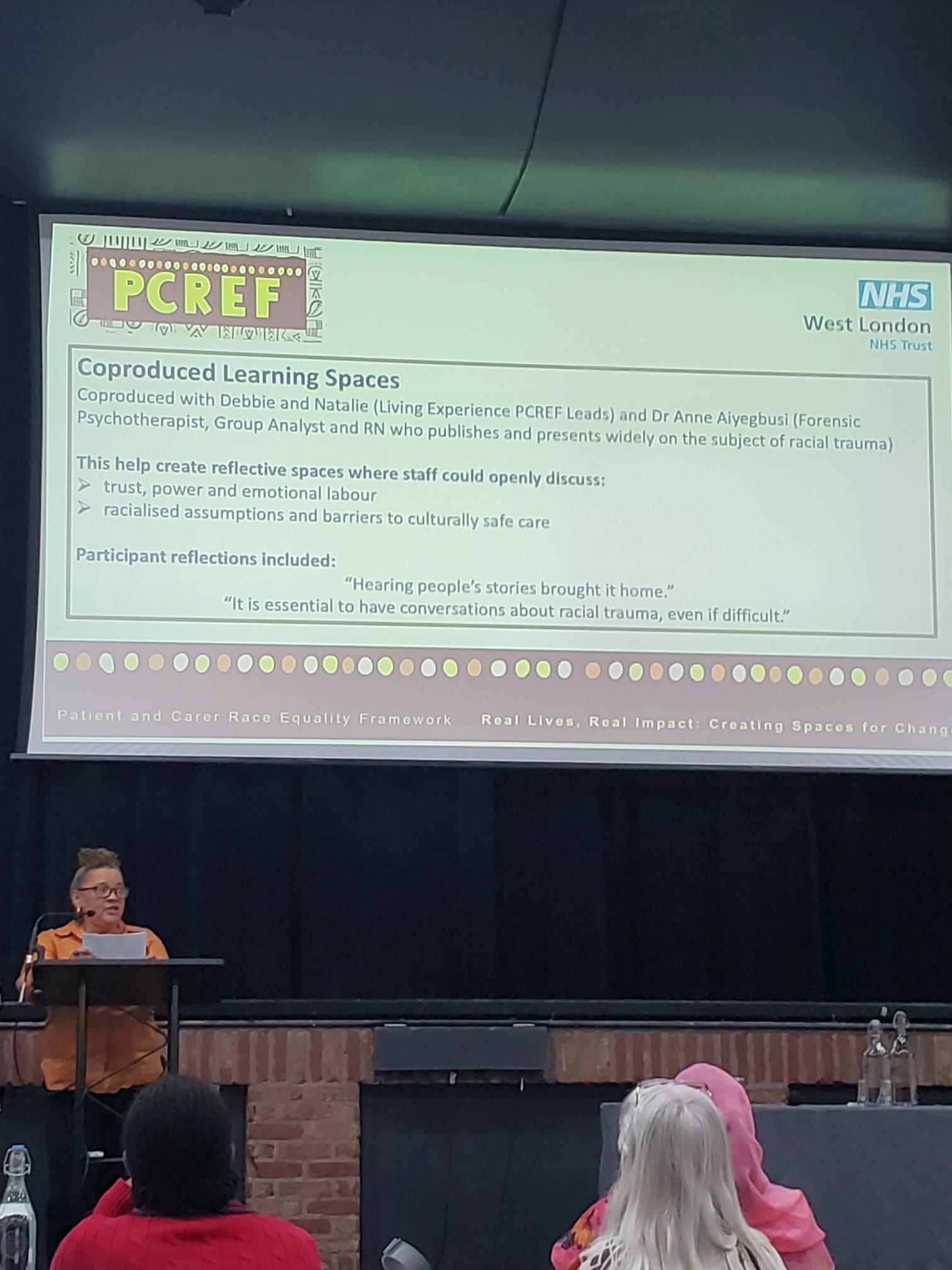
Co-produced Learning Spaces
The racial trauma workshops were developed through a co-production approach involving Debbie Best, Natalie Mark and Dr Anne Aiyegbusi, a forensic psychotherapist, group analyst and registered nurse who has published extensively on racial trauma. Together they designed reflective learning spaces where participants could explore difficult but essential conversations around race, identity and mental health.
The workshops encouraged participants to discuss:
Trust, power and emotional labour.
Racialised assumptions within healthcare.
Barriers to culturally safe care.
Experiences of racism in professional and personal settings.
Organisational responsibilities in responding to racial trauma.
Feedback from participants demonstrated the impact of these conversations. Attendees reported that hearing people’s lived experiences brought the issues to life in ways that data alone could not achieve. Many described the workshops as challenging but necessary, with one participant stating that conversations about racial trauma are essential even when they are uncomfortable.
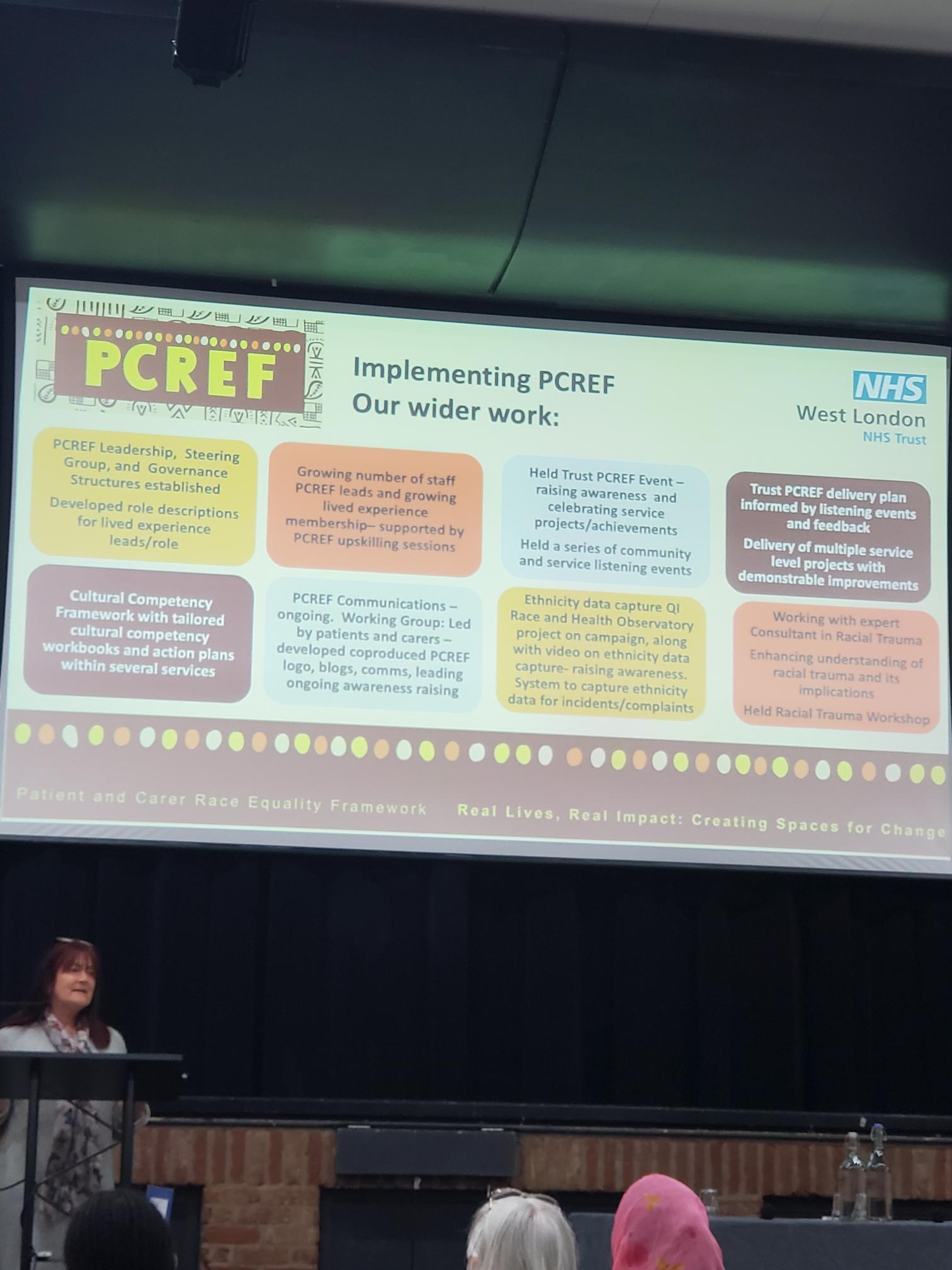
Wider PCREF Implementation at West London NHS Trust
Alongside the racial trauma work, the presentation highlighted wider progress being made through PCREF implementation across the Trust.
Key achievements included:
Establishing PCREF leadership, steering groups and governance structures.
Increasing the number of PCREF leads and lived experience members.
Delivering Trust-wide PCREF awareness events.
Running community listening events and engagement activities.
Developing a Cultural Competency Framework and tailored action plans.
Creating co-produced communications led by patients and carers.
Improving ethnicity data collection and reporting systems.
Working with specialist racial trauma consultants to strengthen organisational understanding.
Particularly noteworthy was the emphasis on co-production. Patients and carers were not simply consulted but actively involved in shaping communications, governance structures, learning programmes and strategic priorities. This demonstrated a commitment to ensuring that those most affected by inequalities have a meaningful voice in driving change.
Key Learning from West London NHS Trust
The West London presentation demonstrated that addressing racial inequalities requires more than policy changes alone. It requires organisations to create spaces where difficult conversations can happen safely, where lived experience is valued as expertise and where learning leads directly to action.
Their work showed that racial trauma is not solely an individual experience but an organisational challenge that requires leadership, accountability and sustained commitment. By combining co-production, cultural competency, workforce development and organisational reflection, West London NHS Trust is helping to create the conditions for more equitable and culturally safe mental health services.
Oxleas NHS Foundation Trust
Reducing Inequalities in Restrictive Practice: From Data to Action
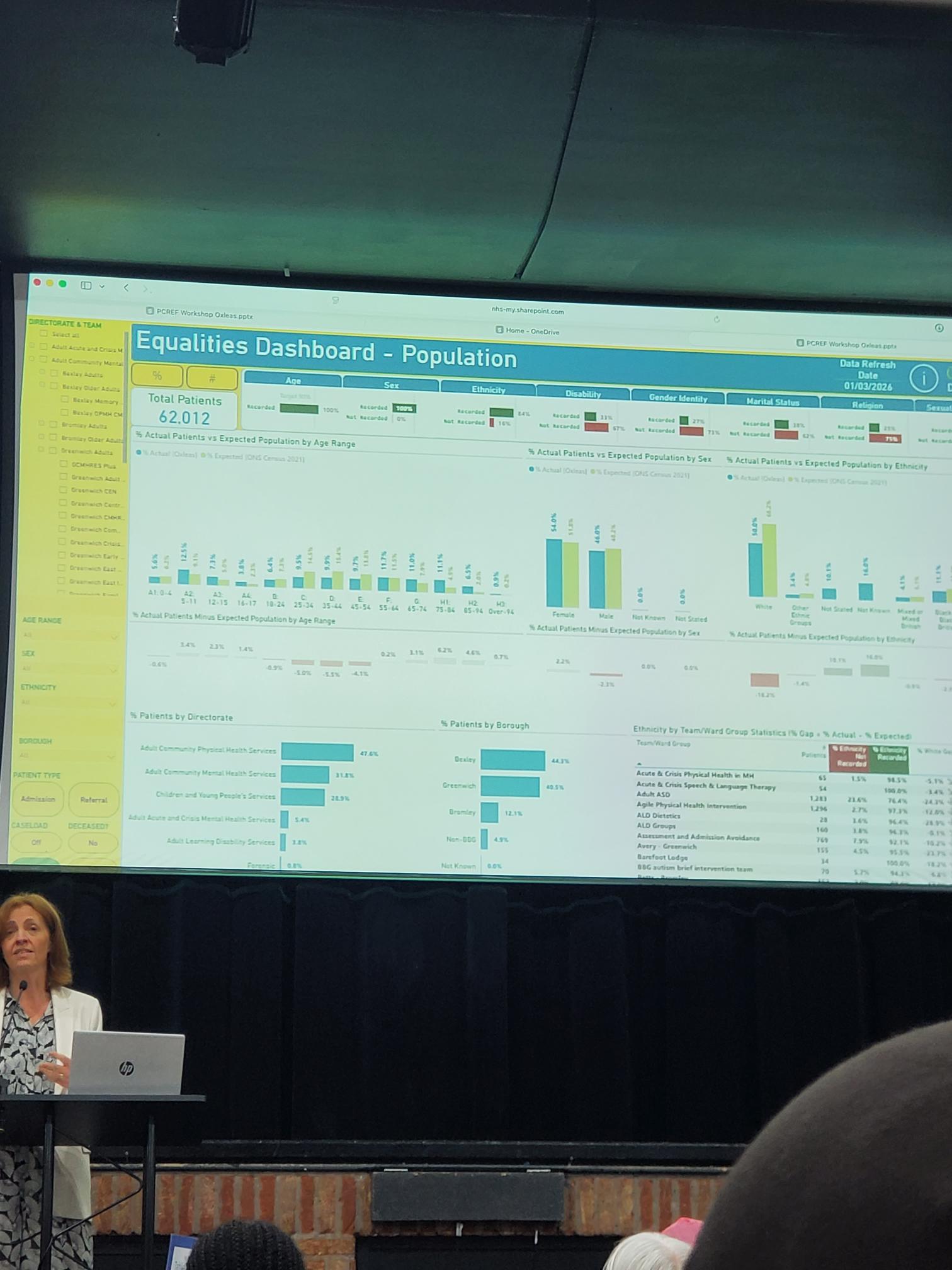
Presented by Oxleas NHS Foundation Trust, this session focused on reducing inequalities in restrictive practice through the lens of the Patient and Carer Race Equality Framework (PCREF). The presentation explored how data, lived experience, trauma-informed care and practical service improvements can work together to reduce the use of restraint, seclusion and restrictive interventions while addressing racial disparities.
The presenters explained that restrictive practices are not experienced equally across all communities. Evidence shows that people from some racialised groups are more likely to experience restrictive interventions, making this both a safety issue and a race equity issue. Oxleas therefore sought to identify practical actions that could improve care while simultaneously reducing inequalities.
Listening to Staff and Stakeholders
As part of their PCREF work, Oxleas engaged staff, service users and stakeholders to identify priorities for change. The feedback was grouped and ranked to establish the strongest starting points for improvement.
The consultation identified two immediate workstreams:
Debrief and Escalation
Trauma-Informed Care
The presentation emphasised that participants did not ask for abstract policy changes. Instead, they identified practical improvements that could be implemented directly within services.
Highest-Ranked Priorities
The most frequently identified priorities included:
A key message from the slide was that stakeholders wanted changes that would directly affect day-to-day care, staff behaviour and patient experience.
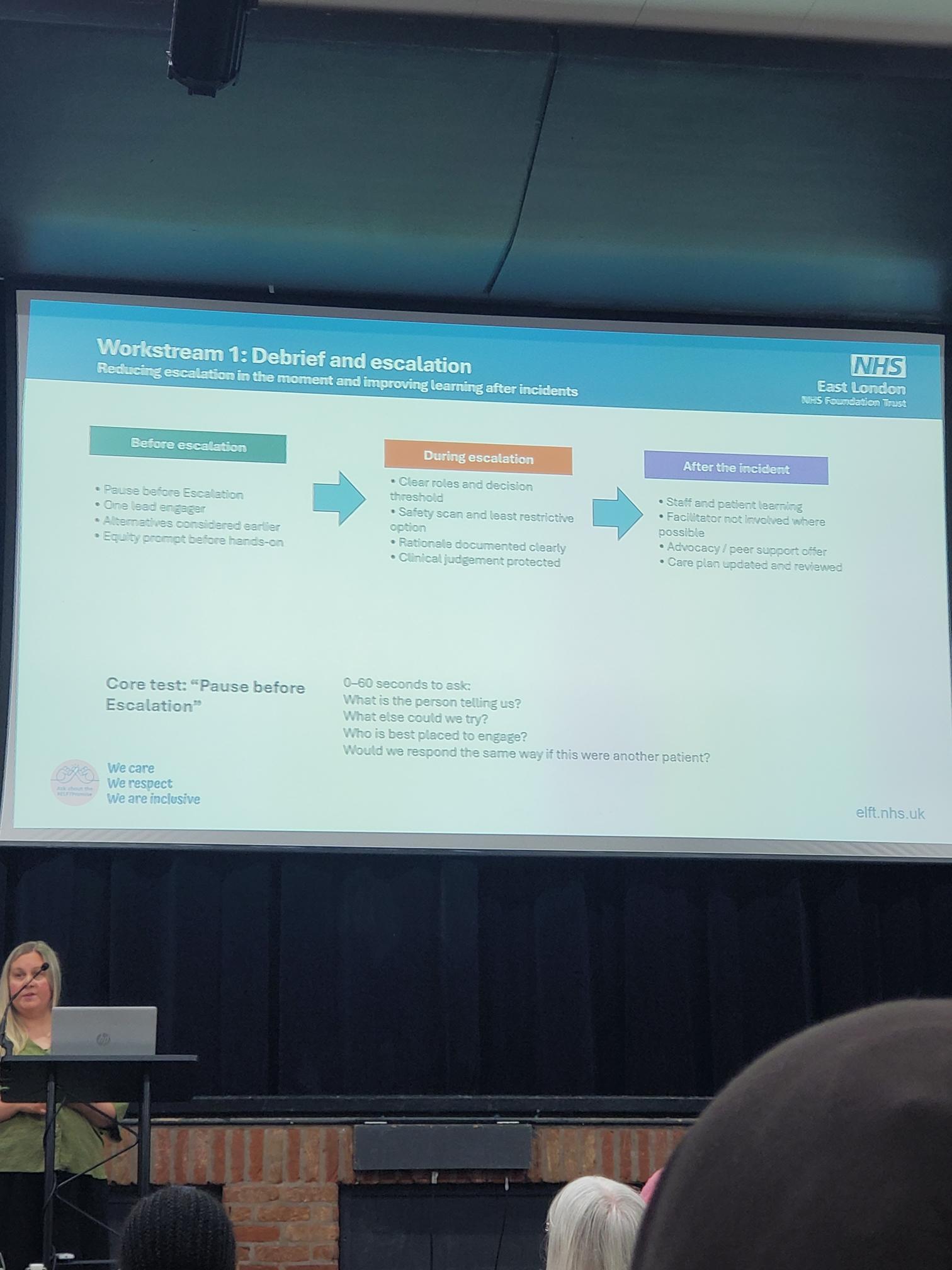
Workstream One: Debrief and Escalation
The first workstream focused on reducing escalation in the moment and improving learning after incidents occur.
The framework was organised into three stages:
Before Escalation
Staff are encouraged to:
Pause before escalating situations.
Ensure one lead staff member takes responsibility.
Consider alternatives earlier.
Use an equity prompt before moving to hands-on interventions.
The emphasis was on slowing decision-making enough to ensure staff are responding to the person’s needs rather than reacting automatically.
During Escalation
The presentation highlighted the importance of:
Clear staff roles.
Defined decision-making thresholds.
Safety scanning.
Choosing the least restrictive option available.
Clear documentation of rationale.
Protecting clinical judgement while maintaining accountability.
The objective is to ensure restrictive interventions are only used when absolutely necessary and are proportionate to the situation.
After the Incident
Learning after incidents was considered equally important.
Actions included:
Joint staff and patient learning.
Independent facilitation where possible.
Advocacy and peer support.
Reviewing and updating care plans.
The focus was not simply on recording incidents but on understanding what happened and preventing repetition.
Next Steps
The presentation concluded with a clear action plan for the coming period.
Planned Actions
Agree a Trust-wide escalation and post-incident learning standard.
Begin testing the “Pause Before Escalation” approach on selected wards.
Finalise a Trust Trauma-Informed Care (TIC) protocol and minimum training standard.
Strengthen dashboard reporting and improve protected-characteristics data quality.
Embed lived experience into the design and review of changes.
These actions reflect the Trust’s commitment to moving from discussion to implementation.
Learning Across London
The presenters also highlighted the importance of collaboration across London’s mental health trusts.
Areas identified for collaboration included:
Common data definitions.
Co-produced interventions.
Trauma-informed escalation practice.
Culturally informed post-incident learning.
Peer review of ward-level improvement projects.
This reflected one of the key themes running throughout the conference: that race equity work is strengthened when trusts learn from each other rather than working in isolation.
North East London NHS Foundation Trust (NELFT)
North East London NHS Foundation Trust (NELFT) presented its PCREF work through the lens of national competencies, demonstrating how race equity can be embedded into everyday clinical practice rather than being treated as a standalone initiative. The presentation, delivered by Erica Deti, Patient and Carer Race Equality Lead, highlighted the importance of developing a workforce that is confident, culturally competent and able to respond effectively to the needs of diverse communities. NELFT emphasised that meaningful change requires organisations to move beyond awareness and into practical action, ensuring that race equity is reflected in leadership, service design and frontline care.
A key focus of the presentation was the development and implementation of national PCREF competencies, designed to support staff at all levels in understanding racial inequalities and their impact on mental health outcomes. Erica explained how these competencies help staff build the knowledge, skills and confidence needed to challenge inequity, engage meaningfully with service users and carers, and contribute to culturally responsive services. The Trust also stressed the importance of involving people with lived experience throughout this process, ensuring that learning is informed by real experiences rather than theoretical concepts alone.
The presentation reinforced the message that achieving race equity is a continuous journey rather than a destination. NELFT shared examples of how the Trust is embedding co-production, reflective practice and accountability into its approach, while encouraging staff to consider how their decisions influence patient experiences and outcomes. By focusing on workforce development, lived experience leadership and organisational learning, NELFT demonstrated how PCREF can act as a catalyst for long-term cultural change, helping to create services that are safer, fairer and more responsive to the communities they serve.
A second NELFT presentation was delivered from local community organisations and Project Zero. This session focused on partnership working with local barbershops, voluntary organisations and community groups as a means of improving engagement with racialised communities. The speakers described how trusted community settings can help bridge gaps between services and populations that may feel excluded from traditional healthcare pathways.
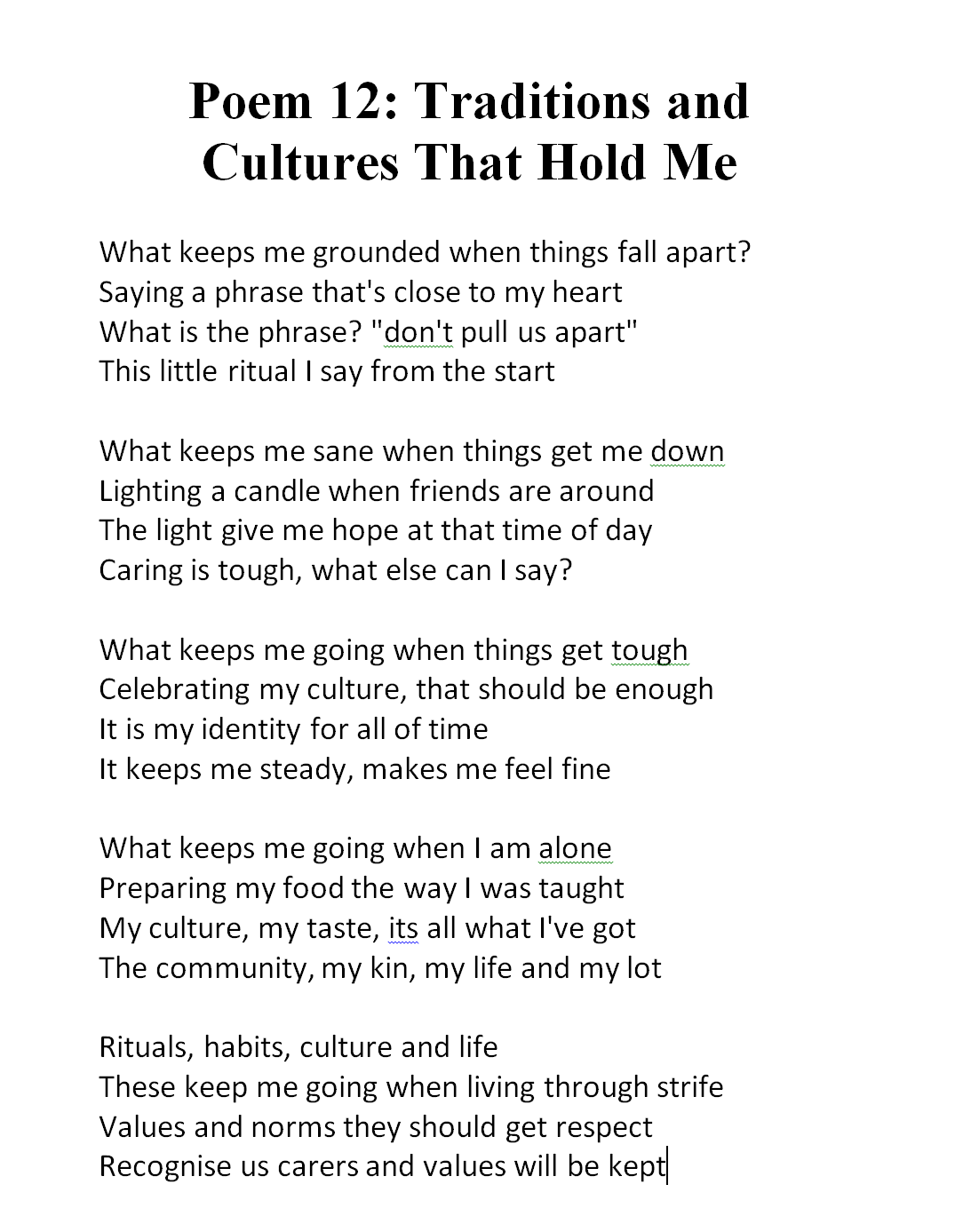
Carer Spotlight
Matthew McKenzie and PCREF Carer Poetry
One of the most powerful moments of the afternoon came during the Carer Spotlight, where carers used poetry to share personal experiences of supporting loved ones through mental health services. The session moved beyond statistics, policies and organisational frameworks to remind attendees of the human stories that sit behind every discussion about race equity, access and care. The poetry was delivered by Matthew McKenzie and fellow carers, creating a reflective and emotional space that grounded the conference in lived experience. Through spoken word and personal reflection, the audience was invited to consider what it truly means to care, advocate and persevere within systems that do not always recognise the voices of carers.
A recurring theme across the poems was the often invisible role of carers. Several pieces explored the emotional labour involved in supporting a family member through periods of crisis, while also navigating complex services and systems.
Here is the poem from Matthew McKenzie taken from his collaborative book (in development) – Unpaid, Unseen and Yet Unbroken
The poems highlighted feelings of exhaustion, responsibility and uncertainty, but also resilience and determination. Listeners heard about the challenges of balancing personal wellbeing with caring responsibilities, and the reality that carers frequently become experts in supporting their loved ones while receiving little recognition themselves. The poetry gave voice to experiences that are often hidden from formal reports and performance data, yet have a profound impact on individuals and families.
Another important theme was the need for genuine partnership between services, service users and carers. The poems reflected frustrations when carers felt excluded from conversations, ignored during decision-making or treated as outsiders despite their deep understanding of the person they support. At the same time, they celebrated examples of compassionate practice, where professionals listened, worked collaboratively and recognised carers as valuable partners in recovery. These reflections connected strongly with the wider messages of PCREF, reinforcing that co-production is most effective when carers are respected, included and treated as equal contributors rather than passive observers.
Central and North West London NHS Foundation Trust (CNWL)
Presented by J’nelle James, Acting Assistant Director of Culture and Equality, Diversity and Inclusion, Central and North West London NHS Foundation Trust (CNWL) showcased one of the conference’s most innovative examples of co-production through the Black Men’s Wellbeing Festival 2026. The presentation focused on how Milton Keynes Talking Therapies worked with Black men, community leaders and local organisations to improve engagement with NHS mental health services. Rather than expecting communities to come to services, CNWL demonstrated how services can go out into communities, build relationships and create spaces where conversations about mental health feel safe, relevant and culturally meaningful.
The presentation explained that the project began during Black History Month in October 2022, when Milton Keynes Talking Therapies hosted a free face-to-face wellbeing session for Black men at Stantonbury Health Centre. The event explored themes including racial trauma, stigma, family relationships, cultural influences and self-worth. What began as a single wellbeing session quickly revealed a significant unmet need within the community. Participants spoke openly about barriers to accessing support and the lack of culturally relevant mental health conversations, leading the team to recognise that a longer-term programme of engagement was needed.
CNWL emphasised that trust cannot be created through a single event or consultation exercise. Instead, trust is earned through visibility, consistency and genuine partnership. The Trust described a three-year journey of listening, learning and working alongside local communities, which ultimately led to the development of the Black Men’s Wellbeing Festival. The project became an example of how PCREF principles can be applied in practice by ensuring that communities are involved in shaping solutions rather than simply being consulted after decisions have already been made.
Building Trust Through Co-Production
A central message throughout the presentation was that “trust isn’t built overnight.” The festival emerged through a deliberate process of relationship-building and community engagement. CNWL outlined six stages that helped transform an initial wellbeing event into a large-scale community-led initiative.
The first stage focused on initial engagement, beginning with the October 2022 wellbeing session. Following this, the team moved into a listening and learning phase, hosting webinars, training sessions and community discussions to understand what Black men wanted from mental health services. Rather than assuming solutions, the Trust spent time listening to experiences and identifying priorities directly from community members.
The next stages involved meeting people in community spaces, strengthening relationships with local organisations and businesses, amplifying messages through trusted community networks and broadening engagement across Milton Keynes. The presentation highlighted that every stage was developed collaboratively with community partners, ensuring that ownership of the programme remained shared rather than NHS-led.
Key Stages of the Journey
Initial engagement through Black History Month wellbeing events.
Listening sessions and community conversations.
Presence at local community gatherings and celebrations.
Building partnerships with local organisations and businesses.
Using trusted networks to amplify messages.
Expanding engagement through media, events and outreach.
The Black Men’s Wellbeing Festival 2026
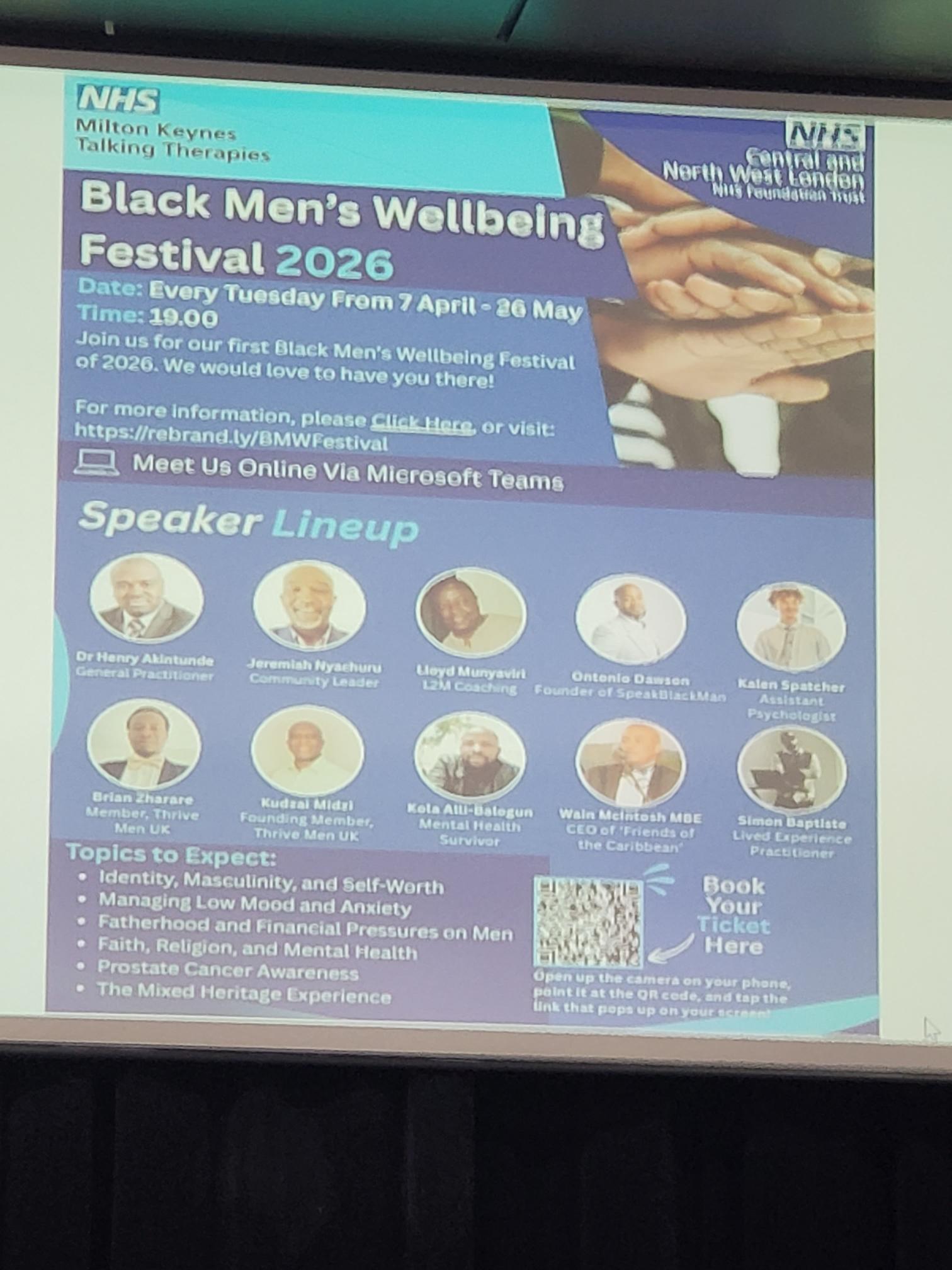
The culmination of this work was the launch of the Black Men’s Wellbeing Festival 2026, a community-led programme designed to improve access and engagement for Black men within mental health services. Running weekly between April and May 2026, the festival brought together clinicians, community leaders, lived experience speakers and local organisations to create open conversations about wellbeing, identity and mental health.
The programme tackled subjects that participants themselves had identified as important. Rather than focusing solely on clinical mental health conditions, the festival explored the wider social, cultural and personal experiences that influence wellbeing. This reflected a more holistic understanding of mental health and recognised that issues such as identity, masculinity, family expectations and discrimination all play an important role in people’s wellbeing.
The festival also demonstrated how NHS services can become more accessible when support is delivered in partnership with trusted community figures. By bringing together professionals and community leaders, CNWL created opportunities for conversations that may not otherwise take place within traditional healthcare settings.
North London NHS Foundation Trust
Equity and Health Inequalities Strategy 2026–2030: “Inclusion in Action”
North London NHS Foundation Trust presented its new Equity and Health Inequalities Strategy 2026–2030, centred on the theme of “Inclusion in Action.” The presentation highlighted the Trust’s ambition to embed equity into every aspect of organisational culture, leadership, workforce development and service delivery. Rather than treating equality and health inequalities as separate workstreams, the strategy positions inclusion as a fundamental principle underpinning better mental health outcomes, improved staff experiences and stronger communities. The Trust’s vision was summarised through the phrase: “Better Mental Health. Better Lives. Better Communities.”
A key theme throughout the presentation was the recognition that addressing inequalities requires action at both organisational and system levels. The strategy aligns with the Trust’s broader five-year organisational goals and is supported by the North London Way, Trust values, leadership framework and staff network structures. The presenters emphasised that lived experience, staff insight and community partnership have been central to shaping the strategy, ensuring that it reflects the realities of the diverse populations served across North Central London.
The presentation also highlighted the importance of shared accountability. Equity was presented not as the responsibility of specialist equality teams alone, but as a collective responsibility across leadership, clinical services, operational teams and partner organisations. Through this approach, the Trust aims to create sustainable cultural change while reducing inequalities experienced by both service users and staff.
Strategic Ambitions and Organisational Change
A major focus of the presentation was how the Trust intends to turn principles into practical action. The strategy builds upon existing organisational priorities while introducing a stronger and more explicit focus on equity and inclusion. The presenters described a framework that links the Trust’s strategic aims, leadership expectations, workforce culture and service improvement activity into a single coherent approach.
The strategy is closely connected to the work of the Staff Networks Alliance, which brings together a range of staff networks representing diverse communities and experiences. The Trust described these networks as essential partners in shaping policy, challenging inequalities and ensuring that organisational decisions are informed by lived experience. This collaborative model reflects a commitment to co-production and shared leadership rather than top-down decision making.
The presentation emphasised a set of organisational values that support inclusive practice, including visibility, accountability, compassion, collaboration and empowerment. These principles are intended to guide both staff behaviour and organisational decision-making. By embedding these values throughout the Trust, leaders hope to create a culture where inclusion becomes a routine part of everyday practice rather than a separate programme of work.
Building on Existing Foundations
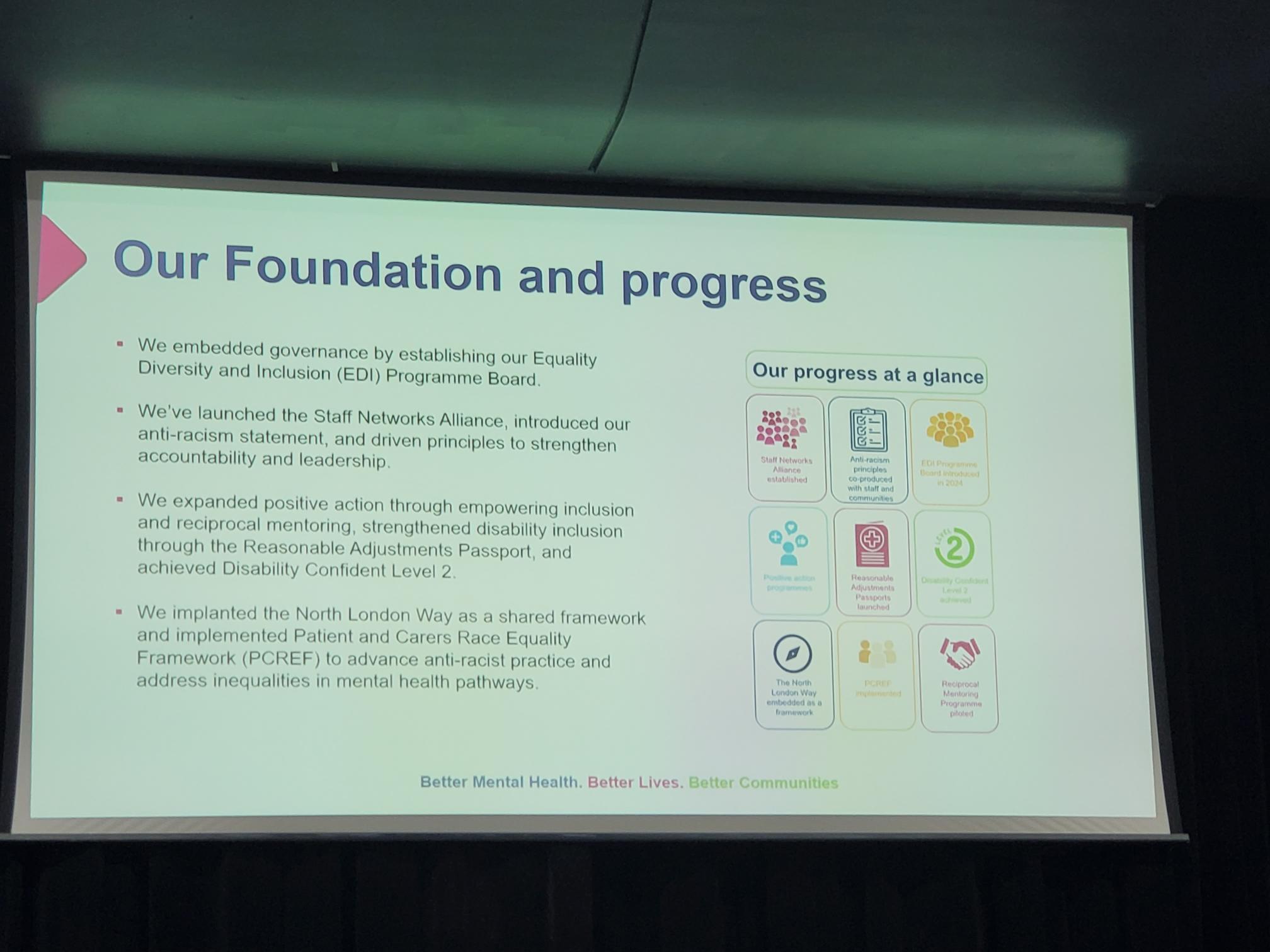
The final section of the presentation focused on progress already achieved and the foundations that have been established to support future work. The Trust outlined a number of significant developments, including the creation of an Equality, Diversity and Inclusion (EDI) Programme Board, which provides governance and oversight for inclusion and health inequalities initiatives. This governance structure helps ensure that equity remains a strategic priority and is monitored at senior levels of the organisation.
The Trust has also introduced several initiatives aimed at strengthening accountability and supporting underrepresented groups. These include the launch of the Staff Networks Alliance, the development of anti-racism principles, positive action programmes, reciprocal mentoring opportunities and improvements in disability inclusion through the Reasonable Adjustments Passport scheme. The Trust reported achieving Disability Confident Level 2 status, reflecting progress in creating a more inclusive workplace environment.
Importantly, the presentation highlighted the implementation of the Patient and Carer Race Equality Framework (PCREF) as a key mechanism for advancing anti-racist practice and addressing inequalities within mental health pathways. Alongside embedding the North London Way as a shared organisational framework, the Trust views PCREF as a central component of its strategy for reducing inequities and improving outcomes. The overall message was that meaningful progress has already begun, but sustained effort, partnership and accountability will be required to achieve the ambitions set out in the Equity and Health Inequalities Strategy 2026–2030.
A recurring message from the closing discussion was that race equity remains everybody’s responsibility. While significant progress has been made, panellists acknowledged that much work remains. Delegates left with a renewed commitment to collaboration, stronger partnerships with carers and communities, and a shared determination to ensure that PCREF continues to drive meaningful and measurable change across London’s mental health services.
Blog by Ethnic Mental Health Carer forum Chair – Matthew McKenzie
The May 2026 Ethnic Mental Health Carers Forum brought together carers, researchers, clinicians, community leaders, and representatives from mental health organisations across England. Although attendance was smaller than usual, the discussion was rich, honest, and highly informative, covering Mental Health Act reform, carers’ experiences, service inequalities, innovative approaches to care, and new research opportunities.
For those who were unable to attend, this blog provides a comprehensive overview of the meeting, including key presentations, audience questions, responses from speakers, and useful resources shared during the session.
Opening Remarks
As the chair, I welcomed attendees and outlined the agenda. The meeting focused on following:
Mental Health Act research and reform
Carers’ experiences supporting loved ones through detention
Findings from a major East Sussex carers research project
Resources for carers under the Mental Health Act
Electronic Health Records and future developments
Wider discussions on racial trauma, inequalities, and service improvement
The meeting also provided opportunities for networking, sharing lived experiences, and highlighting innovative projects happening across the country.
Research Study: Supporting a Loved One Through Mental Health Detention
Dr Maeve Conneely from University College London opened the meeting with a presentation on a new research study exploring the experiences of people who have been assessed or detained under the Mental Health Act, as well as the experiences of family members and carers who supported them through that process. The study has been commissioned as part of the wider programme of Mental Health Act reform and aims to understand how the current “Nearest Relative” provisions operate in practice before changes are introduced under the new legislation.
Dr Conneely explained that researchers are particularly interested in hearing from carers who were involved in supporting a loved one but who were not formally recognised as the “Nearest Relative” under the existing legal framework. She highlighted that these experiences are especially important because they can reveal where carers have been excluded from decision-making, denied access to information, or prevented from contributing to assessments despite playing a significant role in supporting the individual concerned. The study is open to anyone aged 16 or over who has direct experience of Mental Health Act assessments, detentions, Community Treatment Orders, holding powers, or related interventions, whether as a patient or as a supporter.
The research is linked to ongoing reforms of the Mental Health Act and seeks to understand how the “Nearest Relative” provisions currently operate before changes are implemented.
Who Can Take Part?
The study is looking for:
People who have been detained under the Mental Health Act
Family members and carers who supported someone during detention or assessment
Individuals who should have been involved as a nearest relative but were not
Anyone aged 16 or over with relevant experience
Interviews are conducted online and participants receive a £30 shopping voucher as a thank-you for their time.
Key Question from Participants
Q: Does the study include situations where someone should have been involved but wasn’t?
Response: Yes. Researchers are particularly interested in understanding experiences where carers or family members were excluded from decision-making processes despite playing a significant caring role.
Another Important Question
Q: Do carers need permission from the person who was detained before participating?
Response: No. Carers are sharing their own experiences and therefore only need to provide their own consent.
Discussion Themes
Participants highlighted:
Long-standing inequalities affecting Black communities under the Mental Health Act.
The overuse of psychiatric labels without sufficient exploration of trauma.
The need to understand why some individuals receive significantly different experiences of care, including access to private mental health facilities.
Concerns about trust in mental health services and the lasting impact of poor experiences across generations.
Several carers committed to taking part in the study to ensure lived experience informs future policy.
East Sussex Carers Research Project: What Carers Told Us
Age Angiolini presented findings from a year-long carers-led research project examining the experiences of family carers supporting people with serious mental illness across East Sussex. The study was developed in response to repeated concerns raised by carers at local support meetings and sought to capture their experiences of interacting with mental health services provided by the Sussex Partnership Foundation Trust (SPFT).
Although the research received 71 responses, representing only a proportion of the carers population in the region, the findings revealed a striking consistency in the challenges carers face. The survey explored themes including carers’ involvement in care planning, communication with services, consent and confidentiality, quality of care, crisis support, and priorities for improvement. Among the most significant findings were that 72% of carers reported being only sometimes involved or not involved at all in their loved one’s care, 73% felt services relied too heavily on carers, and 72% said they regularly had to advocate to secure appropriate support. The research concluded that many carers feel undervalued, excluded from decision-making, and left carrying significant responsibilities without adequate recognition or support.
The study gathered responses from carers supporting people with:
Schizophrenia
Bipolar disorder
ADHD
Autism
Complex neurodiverse conditions
Although the sample size was relatively modest, the findings revealed significant and consistent concerns.
Key Findings from the report
Carers Feel Excluded
72% reported being only sometimes involved or not involved at all.
73% felt services relied too heavily on carers.
72% said they had to advocate strongly to secure appropriate care.
Communication Failures
Participants reported poor communication between:
Mental health services
Assessment teams
Social services
Mental health liaison teams
Many carers described communications as inconsistent, unclear, and difficult to navigate.
Consent and Confidentiality
A recurring concern was that confidentiality procedures are often applied rigidly, preventing carers from sharing vital information during crises.
Carers argued that this can actively undermine effective care.
Quality of Care Concerns
The research found:
90% reported insufficient care.
Significant concerns around continuity of care.
A strong desire for dedicated care coordinators.
Widespread frustration with crisis services.
Crisis Support is Not Working
Many carers reported that:
NHS 111 is often inadequate for mental health crises.
A&E is frequently unsuitable for people experiencing mental distress.
Services remain reactive rather than preventative.
Calls for Change
Recommendations included:
Better crisis pathways
Improved coordination between services
More trauma-informed approaches
Greater therapeutic support
Increased family involvement
Better support for neurodiverse individuals
The presentation sparked considerable discussion, with many attendees noting that the findings reflected experiences they had encountered for years.
Carers Speak Out: Frustration, Trauma and the Need for Change
One of the most powerful aspects of the meeting was hearing directly from carers.
Several participants reflected on decades of involvement with mental health services and expressed concern that despite repeated reviews, consultations, and reforms, many of the same issues continue to persist.
Common themes included:
Institutional racism
Poor communication
Exclusion of carers
Over-medicalisation
Lack of trauma-informed care
Inadequate support during crises
A number of attendees emphasised that families often become de facto care coordinators, managing appointments, services, medications, and crises while receiving little support themselves.
One participant observed:
“They plan, medicate and treat. We care. Our worlds don’t meet.”
Others highlighted the impact of racial trauma and the way mental health services can fail to recognise the cultural context of distress.
Open Dialogue: A Different Way Forward?
Ren Reins introduced the concept of Open Dialogue, an internationally recognised approach to mental health care that focuses on relationships, networks, and collaborative conversations.
Open Dialogue aims to:
Bring families and professionals together
Reduce fragmentation between services
Focus on lived experience
Build trust
Improve recovery outcomes
Ren explained that major NHS-funded trials are underway and encouraged carers to learn more about the approach.
The discussion generated significant interest, particularly from attendees looking for alternatives to traditional medical models of care.
Nearest Relative Resources Project
Professor Judy Laing from the University of Bristol provided an update on an innovative project designed to support family members and carers who hold, or may hold, responsibilities under the Mental Health Act’s “Nearest Relative” provisions. Drawing on previous research with carers and mental health professionals, Professor Laing explained that many family members who find themselves in the Nearest Relative role often receive little information, guidance, or emotional support despite carrying significant legal responsibilities. In response, her team secured funding to develop a free, co-produced online resource that helps carers understand their rights, responsibilities, and options when supporting a loved one through mental health assessment, detention, and treatment.
Developed in partnership with carers, family members, mental health professionals, and organisations including Mind, Rethink Mental Illness, and Carers Trust, the website provides practical information, downloadable tools, guidance for conversations with professionals, and resources to help carers look after their own wellbeing. Professor Laing stressed that the project has been shaped directly by the experiences of those who have undertaken the role themselves, ensuring that the guidance reflects the realities and challenges carers face in practice rather than simply explaining legal processes.
The project emerged from research identifying significant gaps in information and support for people carrying out the “Nearest Relative” role.
What Has Been Developed?
The project has created a free online resource containing:
Information about legal rights
Guidance on conversations with professionals
Practical tools for meetings
Support for carers’ wellbeing
Resources explaining upcoming legal changes
The materials have been co-produced with carers and family members.
Questions Raised
How are diverse communities included?
Participants asked how the project ensures equity and accessibility.
Professor Laing explained that:
People from ethnic minority backgrounds have contributed to development.
Resources are being improved to increase accessibility.
Additional funding is supporting work around inclusion and accessibility.
Translation and alternative formats are being explored.
How is the project promoted?
Discussion focused on ensuring communities are aware of available support rather than resources existing only online.
Professor Laing outlined efforts involving:
Mind
Carers Trust
Mental health services
Local media
Carer forums
How will the new Nominated Person role protect carers who have traditionally been involved in supporting a loved one?
Several participants expressed concern that replacing the Nearest Relative role could unintentionally weaken the involvement of family members who have historically provided substantial support during periods of mental ill-health. Questions were raised about situations where a person may choose someone other than their primary carer to act as their Nominated Person, potentially reducing carers’ ability to access information or participate in key decisions. Professor Laing acknowledged that these concerns have been raised by many carers and explained that the practical details of how the new system will operate are still being developed. She stressed the importance of carers contributing their experiences to ensure that future guidance recognises the valuable role families often play in supporting recovery and maintaining continuity of care.
What support is available when professionals fail to recognise or understand carers’ legal rights?
Attendees also discussed the reality that many mental health professionals are not always familiar with the legal powers and rights associated with the Nearest Relative role. Participants described situations where carers were excluded from discussions, not informed of important decisions, or felt unable to challenge professional opinions because they lacked confidence in their understanding of the law. In response, Professor Laing highlighted that one of the main objectives of the Bristol resources project is to bridge this knowledge gap by providing practical tools, suggested questions, and clear explanations of carers’ rights. She noted that the project is also developing resources aimed at professionals themselves, with the goal of increasing awareness and ensuring that carers’ legal rights are better understood and respected across mental health services.
Attendees welcomed the commitment to increasing visibility.
Electronic Health Records and Future Developments
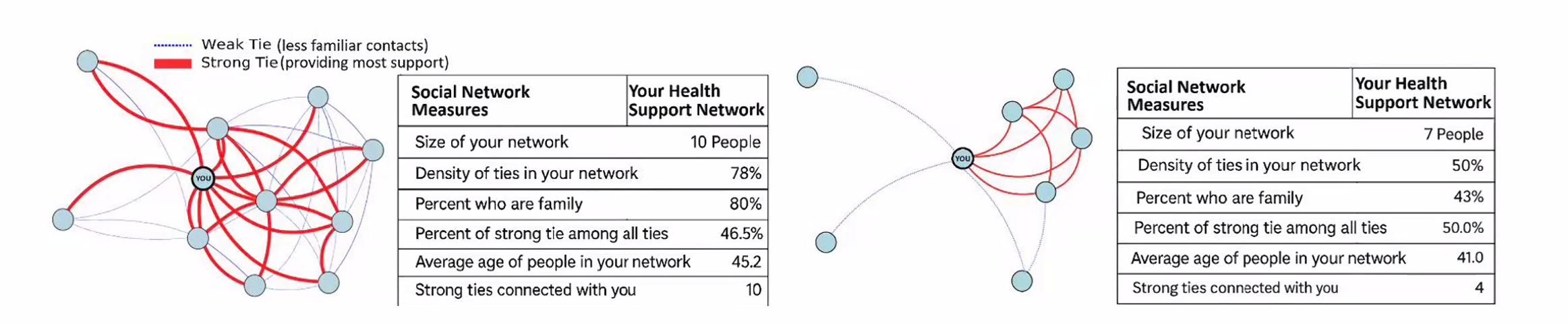
Dr Anna De Simoni, an Academic GP and Associate Professor of Primary Care at Queen Mary University of London, presented an early-stage research proposal focused on how electronic health records could be used to better understand and map the social support networks surrounding people living with multiple long-term health conditions.
Dr De Simoni sought direct feedback from carers to help shape the project before a formal funding application is submitted. She explained that while healthcare professionals can usually identify a patient’s next of kin and household members through existing GP records, they often have very limited understanding of the wider support networks that play a vital role in a person’s wellbeing.
These networks may include family members, neighbours, friends, faith groups, community organisations, carers, and others who provide practical and emotional support. The research aims to explore whether technology and electronic health records can help healthcare professionals better recognise these support systems and use that information to improve care planning, reduce unnecessary hospital admissions, and enhance quality of life for people living with complex health conditions.
The discussion generated considerable interest, particularly regarding:
Information sharing
Integration across services
Support for carers
Data protection concerns
Improving continuity of care
Several participants expressed enthusiasm about the potential benefits while also raising questions regarding privacy and access to NHS information.
Questions and Answers from Dr Anna De Simoni’s Presentation
Q: What problem is this research trying to solve? A: Dr De Simoni explained that healthcare professionals often know very little about the wider support network surrounding a patient. While medical records may identify a next of kin or people living in the same household, they rarely capture the full picture of who is actually providing practical, emotional, or day-to-day support. The project aims to better understand these social networks and use that information to improve care planning and patient outcomes.
Q: Who is the research aimed at? A: The initial focus is on people living with multiple long-term health conditions, including illnesses such as COPD and other complex health needs e.g mental health. The project seeks to understand how stronger recognition of support networks could improve quality of life, reduce hospital admissions, and support people to remain independent for longer.
Q: How would patients contribute information about their support network? A: The proposal includes the use of a Universal Care Plan through the NHS App. Patients would be able to enter information themselves about what matters to them, who supports them, how they prefer to be treated, and what should happen if their health deteriorates. This information could then be viewed and updated by relevant healthcare professionals.
Q: What role could carers play within the proposed system? A: Participants highlighted that carers often provide the majority of practical support but are frequently invisible within healthcare systems. The proposed approach could make carers more visible by helping professionals understand who is involved in supporting a patient and what role they play in maintaining wellbeing and independence.
Q: How will patient confidentiality and data protection be managed? A: Concerns were raised about privacy and the security of NHS data. Dr De Simoni explained that information governance, GDPR compliance, and data protection would be central to the project. Specialists in privacy and information governance would be involved to ensure that any information collected is handled safely, appropriately, and with proper consent.
Key Discussion: Why Are Carers Still Fighting the Same Battles?
A recurring theme throughout the meeting was the sense that many challenges identified today are the same challenges carers raised ten or twenty years ago.
Questions included:
Why are services still fragmented?
Why do carers continue to feel excluded?
Why are communication problems so persistent?
Why is trauma often overlooked?
Why do inequalities remain entrenched?
Participants reflected on whether the issue is primarily one of resources, leadership, service design, or culture.
Many agreed that meaningful change requires carers to remain actively involved in shaping policy and service delivery.
A carers support group recommended during discussion as a source of peer support and shared experience.
Final Reflections
The May 2026 Ethnic Mental Health Carers Forum highlighted both the challenges carers continue to face and the determination across the sector to improve outcomes.
From Mental Health Act reform and carers’ rights to innovative approaches such as Open Dialogue, the meeting demonstrated the importance of bringing together lived experience, research, policy, and practice.
Several speakers reminded attendees that change often begins with carers sharing their stories, participating in research, challenging poor practice, and helping shape future services.
The forum remains an important space where those voices can be heard.
Update by Matthew McKenzie – Chair of South London Mental Health Carers Forum
The South London Mental Health Carers Group met for the month of May for a wide-ranging and thoughtful discussion covering carers’ experiences, mental health support systems, involvement opportunities, and an important research presentation focused on support networks and long-term care.
The group covers areas of Lewisham, Southwark, Lambeth & Croydon, although Mental Health Carers from outside those areas are welcime to attend
The session brought together carers, advocates, involvement leads, and guest speaker Dr Anna De Simone from Queen Mary University of London. As always, the discussion highlighted both the challenges carers continue to face and the value of shared lived experience and peer support.
Opening Discussions: Challenges in Mental Health Care Systems
The meeting began with carers sharing experiences of navigating mental health services for loved ones with complex needs. There was extensive discussion around:
difficulties accessing appropriate placements,
safeguarding concerns,
discharge planning,
lack of continuity between NHS trusts and local authorities,
and ongoing challenges around funding responsibility between different services.
A recurring issue raised was the pressure on inpatient beds and the concern that discharge decisions can sometimes feel driven more by system pressures than by clinical readiness. Carers spoke openly about the emotional impact of repeatedly having to advocate for vulnerable loved ones while navigating fragmented systems.
There was also discussion around the importance of carers being recognised and included in communication and planning processes. Participants highlighted how carers are often the people most aware of deterioration, risks, or safeguarding concerns, and how vital it is that services engage meaningfully with families and informal supporters where appropriate.
Despite frustrations, carers also acknowledged examples of good practice and supportive professionals within mental health services. Several attendees noted that they had seen gradual improvements in carer involvement and listening exercises within parts of South London and Maudsley NHS Foundation Trust (SLAM), particularly in Lambeth.
Updates on Carer Involvement and Support Activities
The group received updates from carers and representatives involved in local mental health engagement work and carers’ organisations.
Carers Week Activities
Karen from Carers Hub Lambeth shared details of upcoming Carers Week activities, including:
outreach events,
wellbeing sessions,
information stalls,
and activities for both adult and young carers.
The events aim to provide carers with opportunities for support, networking, practical advice, and wellbeing activities.
There was also discussion around changes and developments within SLAM involvement structures, including:
continuation of family and carers meetings,
changes to involvement leads,
and ongoing reviews of the involvement register.
Attendees reflected positively on the increasing recognition of carers’ voices in some forums and clinical meetings, while acknowledging that there is still much work to do to ensure consistent involvement across all boroughs and services.
Guest Presentation: Mapping Patient Support Networks
The second half of the meeting focused on a presentation from Dr Anna De Simone, GP and Associate Professor of Primary Care at Queen Mary University of London.
Anna introduced a proposed research project exploring how healthcare systems might better understand and map patients’ support networks using electronic health records and social network tools.
The research proposal focuses particularly on patients with long-term conditions such as COPD (Chronic Obstructive Pulmonary Disease), many of whom also experience multiple additional health conditions and varying levels of social isolation.
The Core Idea
Anna explained that while healthcare professionals can currently access limited information such as next of kin or household members, they often lack a fuller understanding of:
who actually supports the patient,
how reliable that support is,
whether support networks are connected or fragmented,
and how socially isolated a patient may be.
The proposed research would explore whether creating visual “maps” of support networks could help:
improve care planning,
reduce crises,
improve coordination between services,
and enhance patients’ quality of life.
The project would also examine how social prescribing, community services, online support groups, and carers fit into these wider support networks.
Carers’ Feedback on the Research Proposal
The discussion following Anna’s presentation was extremely rich and constructive, with carers offering both enthusiasm and important cautionary perspectives.
Strong Support for the Concept
Many attendees felt the project addressed an important gap in healthcare planning. Several carers spoke about how informal support networks had been essential to helping them or their loved ones survive periods of crisis.
Participants agreed that professionals often underestimate the role played by:
friends,
neighbours,
online communities,
peer groups,
and unpaid carers.
The ability to visualise these networks was seen as potentially valuable for both professionals and patients themselves.
Importance of Non-Traditional Support Networks
A strong theme throughout the discussion was that support does not always come from family.
Some carers explained that family relationships can sometimes be unsafe or abusive, and that support may instead come from trusted friends, neighbours, carers’ groups, or online communities.
The group stressed that any future system should avoid assuming that family automatically equals safety or support.
Online Communities and Digital Support
Participants also highlighted the increasing importance of online support systems.
Several carers explained that:
Zoom groups,
Facebook communities,
online peer support,
and digital communication can provide essential social connection, especially for disabled or isolated people.
One participant noted that online support networks had directly helped them access practical support and reduce isolation when physical mobility was limited.
At the same time, carers cautioned that not everyone has equal access to digital services. Concerns were raised about:
digital exclusion,
accessibility barriers,
lack of digital skills,
and the risk of widening inequalities.
The importance of offering both digital and non-digital forms of support was strongly emphasised.
Privacy, Consent, and Mental Health
Carers also discussed potential challenges around privacy and consent, particularly for people experiencing paranoia or severe mental illness.
Some attendees noted that patients may not always feel comfortable sharing details about their social networks, and that trust and safeguarding would need to be central to any future system.
There was discussion about the delicate balance between:
confidentiality,
safety,
carer involvement,
and patient autonomy.
Role of Social Prescribers
The group generally agreed that social prescribers could play an important role in helping patients map support networks, because they often have more time and a stronger focus on community support than standard GP appointments allow.
However, concerns were raised about long-term funding and sustainability for social prescribing services.
Looking Ahead
Anna thanked the group for their detailed feedback and explained that carers’ insights would help shape the next stage of the research proposal before submission later this year.
There was strong interest from attendees in remaining involved should the project move forward, particularly around future patient and public involvement opportunities.
The meeting once again demonstrated the depth of knowledge, experience, and expertise held by unpaid carers. The discussion reflected not only the challenges carers continue to face, but also the importance of ensuring carers are recognised as essential partners in both healthcare delivery and future research.
If you’ve supported someone through a stay in mental health services, your experience could help improve care for others.
Researchers at The University of Manchester are inviting people with lived experience—including carers to take part in an online workshop focused on improving how mental health services support people during hospital discharge, particularly for individuals from Black heritage communities.
Reason for research
Evidence shows that people from Black communities often face poorer outcomes in mental health care, including barriers to access and challenges during discharge from hospital.
To address this, researchers are working to make future services and research more inclusive, culturally responsive, and grounded in real experiences. Hearing directly from carers is a key part of that work .
Who is running this?
The workshop is being led by Dr Natasha Tyler, a Research Fellow at The University of Manchester, as part of work linked to improving future research and care approaches.
The session will also be supported by facilitators with lived experience, including carers, to ensure discussions are grounded and meaningful .
Who can take part?
You may be interested if you:
Have cared for someone who has been an inpatient in adult mental health services
Have experience of discharge from mental health care
Want to share your perspective to improve future support
What’s involved?
Format: Online (MS Teams)
Duration: 2 hours
Dates: Sessions planned between 23rd April and 8th May 2026
Payment: £60 as a thank-you for your time
Participants will receive questions in advance to help prepare for the discussion.
Why get involved?
Taking part is a chance to:
Help shape future mental health research and services
Ensure carers’ voices are included in decision-making
Contribute to reducing inequalities in care
Share your experience in a supportive environment
How to express interest
If you’d like to take part, you can follow the link in the invitation to share your availability or contact the research team directly.
By Matthew McKenzie – Triangle of Care Community Chair.
The meeting opened with a welcome to carers, professionals, and partner organisations, reinforcing the importance of the Community Group as a collaborative and inclusive space. The Chair highlighted the ongoing commitment to co-production, ensuring that lived experience remains central to all Triangle of Care development and decision-making.
The purpose of the meeting was outlined, with emphasis on shared learning, constructive challenge, and influencing national work. Members were reminded that discussions within the group directly inform improvements to Triangle of Care standards, guidance, and implementation across services.
2. Triangle of Care Update (with Q&A)
Mary Patel – Carers Trust
The Triangle of Care update focused on how the programme continues to evolve as a learning-led, improvement-focused framework rather than a compliance or inspection tool. Members were reminded that the Triangle of Care is designed to support services to reflect honestly on how well carers are recognised, involved, and supported, and to identify practical actions for improvement.
The update highlighted the growing maturity of the self-assessment and peer review process. Increasingly, organisations are using the framework not only to evidence good practice but to challenge themselves, learn from others, and embed carer partnership more consistently across teams and pathways.
Self-Assessment and Peer Review: What’s Working Well
The self-assessment process continues to be a key entry point for organisations engaging with the Triangle of Care. Where we were updated on how self-assessment encourages teams to pause and reflect on everyday practice, policies, and culture, rather than relying solely on written procedures. When combined with peer review, this reflection is strengthened by external challenge and lived-experience insight.
As part of the update, members were updated on emerging learning from Triangle of Care reports, including self-assessment submissions and peer review feedback. These reports were described as an important source of insight into how carer involvement is experienced on the ground, highlighting both areas of strong practice and recurring challenges across services
NOTE: These include reports going back 6 months, so not all NHS trusts listed
Peer review was described as most effective when organisations approach it with openness and curiosity. Lived-experience peer reviewers play a crucial role in asking different questions, highlighting blind spots, and grounding discussions in real-world carer experience.
A key discussion point was how to balance national consistency with local flexibility. Members acknowledged that while the Triangle of Care provides a shared framework and standards, services operate within different contexts, populations, and resource constraints.
Triangle of care and Patient Carer Race Equality Framework updates
The Triangle of Care and PCREF Phase 2 pilot will be launched in April 2026, to test co-produced specialist guidance to support integration of carers from racially marginalised communities into the Triangle of Care.
Alignment with Wider System Priorities
Members discussed how Triangle of Care activity aligns with broader system developments, including Mental Health Act reform, integrated care, and equality frameworks. There was strong agreement that Triangle of Care should not sit in isolation but be embedded within wider quality improvement, safeguarding, and workforce development agendas.
The need to visibly align Triangle of Care with the Patient and Carer Race Equality Framework was reiterated. Members emphasised that carers must be able to see how equality commitments translate into tangible actions within standards, training, and evidence.
Key points
Aligning Triangle of Care with Mental Health Act reform
Embedding within wider system and quality frameworks
Stronger visibility of equality and race equity
Carer Voice and Evidence of Impact
A recurring theme was the importance of demonstrating impact. Members discussed how services can better evidence carer involvement and experience beyond policies and training records. This includes qualitative feedback, lived-experience insight, and examples of how carer input has influenced service design and delivery.
Emerging Challenges and Areas for Development
The update also acknowledged ongoing challenges, including workforce pressures, digital transformation, and uneven awareness of the Triangle of Care across organisations. Members noted that carer involvement can become fragile during periods of change unless it is firmly embedded in systems and culture.
Summary: Where the Programme Is Heading
The Triangle of Care update concluded with a shared understanding that the programme is well-established but still evolving. The focus for the next phase is on deepening impact, strengthening alignment with equality and legislative change, and supporting services to move from intention to consistent, inclusive practice.
Key discussion points
Peer review as a developmental, learning-focused process
Balancing national consistency with local flexibility
Alignment with Mental Health Act reform and equality frameworks
Keeping carer voices central to assessment and review
3. Sharing Experiences as a Peer Reviewer
Carer involved with Avon & whitlshire
A carer presented from her involvement at Avon and Wiltshire Mental Health Partnership NHS Trust, where she is involved as a lived-experience peer reviewer contributing to Triangle of Care.
She shared reflections from her role as a lived-experience peer reviewer. She spoke about the importance of authenticity, trust, and transparency in the peer review process, and how lived experience strengthens both credibility and impact. Her contribution reinforced the value of co-production and highlighted how peer review can challenge assumptions, surface good practice, and promote more carer-inclusive cultures within organisations.
The discussion reinforced that organisational openness and leadership engagement are critical to turning peer review feedback into real change. Members reflected on how hearing directly from peer reviewers deepens understanding of the practical impact of policies on carers.
Q&A / Discussion
Members asked how organisations typically respond to lived-experience feedback.
The involved carer noted that openness and leadership support were key factors in whether reviews led to meaningful change.
Discussion reinforced the importance of preparing services for peer review so that carers feel genuinely welcomed and listened to.
4. Carer Contingency Planning – Presentation and Local Practice
Mary Patel Local example: Carly Driscoll – Bradford District Care
This session focused on carer contingency planning as a key element of carer support and crisis prevention. The presentation outlined why contingency planning is critical in reducing carer anxiety, preventing emergency admissions, and ensuring continuity of care when carers are unable to continue their role.
Carer Contingency Planning (CCP), as championed by Carers Trust, is designed to support carers by planning ahead for times when they might suddenly be unable to continue caring. This might include illness, emergencies, hospitalisation, or other crises. CCP shifts the focus from reactive support during crisis moments to proactive planning that reduces anxiety and prevents avoidable breakdowns in care.
Carers Trust emphasises that CCP is a conversational, personalised process where the carer’s expertise is central. Carers know the routines, preferences, and cues that matter for the person they care for; the goal of CCP is to capture that knowledge in a way that can be shared quickly and effectively with services, families, and emergency responders when needed.
A local practice example from Bradford District Care demonstrated how contingency planning can work in practice, highlighting practical tools, partnership working, and engagement with carers. Discussion explored the benefits of clear, accessible plans, while also acknowledging challenges around awareness, consistency, and uptake
The local practice example demonstrated how contingency planning can be embedded into routine work through partnership approaches and proactive engagement with carers. Members discussed the importance of introducing plans early and reviewing them regularly.
Key features of the Bradford approach
Routine integration: CCP discussions happen early, not just in crisis moments
Partnership working: Health, social care, and voluntary sector staff work in concert
Accessible documentation: Plans are shared in forms that carers can use and update
Support for carers: Carers are supported to lead the planning, not be passive recipients
Ongoing review: Plans are revisited as needs and circumstances evolve
Benefits seen locally
Carers report feeling more confident and less anxious
Greater clarity across professionals when carers are unavailable
Fewer last-minute, unplanned crises or service escalations
Better use of local support networks when official services are stretched
Q&A / Discussion
Questions focused on how contingency plans are introduced to carers and reviewed over time.
Members raised concerns about low awareness of contingency planning among carers not already engaged with services.
Discussion highlighted the need for flexibility, recognising that carers’ circumstances can change rapidly.
5. Carer Contingency Planning – System Perspective
Sara Lewis – SW London ICB
Sara Lewis’s session focused on Carer Contingency Planning (CCP) as a core, preventative element of carer support rather than a reactive or optional add-on. CCP is a structured way of planning for what should happen if a carer is suddenly unable to continue caring due to illness, crisis, exhaustion, or an emergency. At its heart, CCP is about reducing uncertainty and anxiety for carers while ensuring continuity and safety for the person they support.
Sara emphasised that effective CCP recognises carers as partners with expert knowledge of the person they care for. The process supports carers to articulate what matters most, what routines and support are essential, and who needs to be contacted in an emergency. When done well, CCP helps prevent avoidable crises, emergency admissions, and breakdowns in care by making plans visible, accessible, and shared across relevant services.
Accessibility was a major theme, particularly the risks of digital exclusion. While digital tools can be effective, members stressed the need for non-digital options, language support, and culturally appropriate approaches to ensure equity.
Key Takeaways from Sara Lewis’s Session
Carer Contingency Planning is preventative, not reactive
CCP is built on early, ongoing conversations with carers
Plans should reflect what matters to carers and the cared-for person
CCP must be accessible, inclusive, and culturally appropriate
Digital tools can help, but must not increase exclusion
Successful CCP requires shared ownership across services
When embedded well, CCP reduces crisis, anxiety, and system pressure
Q&A / Discussion
Members questioned how to balance digital innovation with the risk of digital exclusion.
Language barriers and accessibility for carers with different communication needs were highlighted.
Discussion emphasised that contingency planning must be embedded into standard care planning processes, not treated as optional or additional.
6. Looking Ahead: Priorities for the Community Group
The “Looking Ahead” discussion focused on how the Triangle of Care Community Group can continue to influence meaningful change for carers in an evolving policy and practice landscape. Members reflected on the increasing complexity of health and care systems and the importance of ensuring that carers are not left behind as reforms, digital transformation, and workforce pressures accelerate.
A strong theme throughout the discussion was visibility, making carer involvement, equality, and partnership explicit in practice, evidence, and outcomes. Participants emphasised that carers must not only be recognised in principle but experience consistent involvement and support in real-world settings. The group agreed that the next phase of work should strengthen both strategic influence and practical implementation.
Mental Health Act Reform and Carer Involvement
Members discussed the implications of upcoming Mental Health Act reform, particularly around carers’ rights, information-sharing, and involvement in decision-making. There was recognition that Triangle of Care principles provide a strong foundation for supporting services to meet new expectations, but that further work will be needed to translate legislation into everyday practice.
The group highlighted the risk that carers could be inconsistently involved if workforce understanding is weak or if systems focus narrowly on legal compliance. Proactive guidance, training, and examples of good practice were seen as essential to ensure carers are meaningfully included rather than consulted as an afterthought.
Equality, Race Equity, and Inclusion
A central priority looking ahead is ensuring that Triangle of Care activity visibly aligns with the Patient and Carer Race Equality Framework (PCREF). Members stressed that carers from racialised and marginalised communities often face additional barriers to involvement, including mistrust, cultural misunderstandings, and unequal access to support.
The group agreed that equality must be embedded into standards, peer review evidence, and training—not treated as a parallel or optional agenda. This includes capturing meaningful data, listening to diverse carer voices, and ensuring culturally responsive practice is clearly demonstrated.
Workforce Training and Education
Workforce development was identified as a critical lever for long-term change. Members highlighted the need to strengthen carer awareness training across all roles, particularly for staff new to mental health and social care settings. Without this foundation, carer involvement remains inconsistent and dependent on individual attitudes rather than organisational culture.
There was strong support for influencing pre-registration education, including universities and training providers, to embed carer awareness earlier. This was seen as an opportunity to normalise partnership with carers from the start of professional careers rather than trying to retrofit it later.
Key points
Strengthening carer awareness across the workforce
Embedding Triangle of Care principles early in training
Influencing universities and pre-registration pathways
Moving from individual goodwill to system-wide culture change
Digital, Data, and Accessibility
Digital transformation featured prominently in the discussion, with members acknowledging both its potential and its risks. While improved data systems and digital tools can support information-sharing and coordination, there was concern that carers without digital access or confidence may be excluded.
Participants emphasised that digital solutions must be designed inclusively, with non-digital alternatives always available. Data collection should support understanding of carer experience and inequality, not become a barrier to support.
Key points
Digital tools should support, not replace, relationships
Risk of digital exclusion for some carers
Importance of non-digital alternatives
Using data to improve equity, not reinforce gaps
Young Carers and Marginalised Groups
Supporting young carers and carers from marginalised communities was highlighted as a continuing priority. Members noted that these groups are often under-identified and less likely to be involved in care planning or decision-making, despite carrying significant caring responsibilities.
The group agreed that future work should focus on visibility, early identification, and tailored approaches that recognise the specific needs and challenges faced by these carers. Partnership with education, community, and voluntary sector organisations was seen as essential.
Key points
Improving identification of young carers
Addressing barriers faced by marginalised carers
Tailored, age-appropriate and culturally sensitive support
Stronger partnership working beyond health services
Collective Commitment Moving Forward
The discussion concluded with a shared commitment to using the Community Group as a platform for influence, learning, and accountability. Members recognised the value of continuing to share practical examples alongside strategic discussion, ensuring that Triangle of Care principles are translated into everyday practice.
Looking ahead, the group aims to remain proactive, inclusive, and responsive—supporting services to recognise carers as equal partners and ensuring that no carer is left unseen or unsupported as systems evolve.
Key discussion points
Preparing for Mental Health Act reform
Embedding the Patient and Carer Race Equality Framework
Improving workforce training and education pathways
Supporting young carers and marginalised communities
Improving data and digital systems without exclusion
As Chair I thanked contributors and reaffirmed the importance of continued collaboration to ensure carers are recognised as equal partners in care, with Triangle of Care principles translated into meaningful practice across services.
For those interested to hear more about triangle of care, see details below
Our final Triangle of Care (ToC) Community Group meeting of the year brought together carers, professionals, and ToC members from across the UK to share updates, raise concerns, and discuss priorities for 2026 and beyond. Although Microsoft Teams provided some surprises, we made it work, thanks to teamwork and patience. The conversation was rich, heartfelt, and often very moving.
1. Opening & Agenda
As chair of the meeting, I acknowledged technical teething problems as the group used Teams for the first time in this format. Mary (ToC Programme Lead) welcomed attendees and explained the privacy-driven decision to hide email addresses, which also unfortunately hid attendees’ names. A fix will be implemented before the January meeting.
The agenda included:
Triangle of Care national updates (Mary)
Carer co-production and lived experience input (Matthew)
Surrey & Borders’ co-production example (postponed)
Research priority-setting presentation (Richard, University of Manchester)
Carer questions and discussion
2. Triangle of Care National Update (Mary)
Mary provided a comprehensive end-of-year update structured around ToC’s three priority areas for 2024–25.
2.1 Embedding the Relaunched Triangle of Care Framework
Growth & progress
16 new members have joined the scheme since April, bringing ToC membership to over 80.
The first Welsh hospital achieved a ToC Star Award, prompting the creation of a new Welsh-language logo and Welsh materials.
A social care pilot is underway with Livewell South West, with West Hertfordshire Teaching Hospital reviewing ToC criteria for an acute setting.
Nine Star Awards have been achieved this year, with a further 12 annual reviews approved. Many more annual reports are pending review before year-end.
Standardising data Mary emphasised the push for consistent reporting across Trusts, including:
numbers of carers identified
uptake of carer awareness training
numbers of carer champions
This will help build a national picture of impact.
Webinars ToC’s Lunch & Learn series continues, with the recent Carers Rights Day webinar (in partnership with University of Bristol) focusing on the Nearest Relative role under the Mental Health Act (MHA). Resources are available via Carers Trust’s YouTube channel.
2.2 Young Carers: Identification & Support
A major update was the successful national policy win relating to young carers and the Mental Health Act.
Mental Health Act Reform – Safety Net for Young Carers
Following campaigning by Carers Trust, the Young Carers Alliance, and ToC members who wrote to MPs:
Government has agreed to update the MHA Code of Practice to require:
identification of children when an adult is detained
sharing of information about available support
referrals for young carer needs assessments
Updates to advance choice documents will require practitioners to ask about dependent children.
Expected implementation: Summer 2026.
This win was warmly welcomed by the group.
2.3 Racially Minoritised Carers & PCREF
Mary updated members on ToC’s work to ensure carers are fully represented in the Patient & Carer Race Equality Framework (PCREF).
Key updates
A national Task & Finish Group has now completed its review of the first four ToC standards; the final standard is underway.
Piloting of new culturally sensitive criteria is planned with 10 NHS Trusts beginning April 2026.
Example of early good practice: Livewell South West is implementing a new “essential data template” that includes carers, enabling services to better identify and support racially minoritised carers.
Carers Trust is calling for a statutory duty for NHS mental health providers to implement PCREF in full, including community governance.
2.4 Changing the Narrative on Care – New Research
Mary introduced new research (supported by the Health Foundation and Oxfam GB) titled Changing the Narrative on Care, highlighting:
Although 80% of the public value unpaid care, this does not translate into policy action or investment.
Three recommended reframes:
Care is a universal experience, not a niche issue.
No care without support, make support visible and tangible.
Care is a partnership between families, communities and systems—not something families must do alone.
The full report is available on Carers Trust’s website.
I then presented an in-depth reflection on the value of authentic carer involvement, drawing on his lived experience and his role working with multiple NHS organisations.
Key points included:
Carers are not passive observers, they hold critical lived knowledge that improves services.
Real co-production goes beyond consultation; carers must be equal partners in shaping policy, documentation, training, and strategic decisions.
Examples Matthew gave from his own involvement:
redesigning welcome packs and leaflets
addressing confidentiality misapplication
involvement in recruitment panels
delivering training to staff at induction
reviewing complaints and compliments themes
advising on discharge processes and family-inclusive safety protocols
participating in research steering groups
Carers’ insight is especially essential in safeguarding, quality boards, and identifying service gaps often invisible to professionals.
4. Surrey & Borders Co-Production Example
A planned presentation from Surrey & Borders was postponed, as the relevant colleague could not attend with materials. They hope to present at a future meeting.
5. Research Priority Setting in Secure & Forensic Mental Health (Richard Kears)
Richard introduced a national project with the James Lind Alliance (JLA) aiming to identify the top 10 research priorities for secure and forensic mental health services across England, Scotland and Wales.
Who is the survey for?
Carers
People with lived experience of secure/forensic services
Staff working in these services
Anyone indirectly connected (victims, families)
Purpose
To ensure future mental health research is led by the real concerns of those most affected, not only by academics or pharmaceutical interests.
Process
National survey gathering research questions.
Analysis to identify common themes.
Second, more focused survey to refine priorities.
National workshops with carers, staff and people with lived experience to finalise the top 10.
A QR code and flyer were shared for distribution. The group expressed strong support.
6. Attendee Discussion & Questions
This was the richest section of the meeting, with many heartfelt contributions. The themes below reflect the key concerns raised.
6.1 Scotland & UK-wide ToC Alignment
A carer asked why Scotland’s ToC framework is separate and not integrated into the UK ToC accreditation model. Mary explained:
Scotland currently uses ToC only as a free policy framework.
Implementing the accreditation model in Scotland would require groundwork to assess willingness and ability of providers to fund membership.
Integration is being discussed but is not imminent.
6.2 Clarity on Co-Production
Several carers voiced concerns that:
“Co-production” is often used as a buzzword.
Some NHS Trusts label work as co-produced after completing it.
Carers need clarity on what ToC means when using the term.
Mary responded that ToC uses a ladder of engagement, distinguishing:
carer engagement
carer involvement
full co-production
Carers Trust is developing a formal principles-based statement on involvement for future meetings.
6.3 Older Carers: Visibility, Support & Inequalities
The majority of carer questions focused on the unmet needs of older adult carers, many of whom are supporting people with severe mental illness—not dementia—and often have been caring 20–40 years.
Attendees reported:
Feeling “invisible” within both policy and services.
Being incorrectly grouped under “older carers = dementia”.
Their own poor health affecting their caring ability.
Increasing struggle to get responses from professionals.
Serious concerns about who will care for their loved ones when they die.
Feeling less heard as they age, compared with younger carers or newer voices.
One carer (age 78) shared:
“I can’t retire from caring. Benefits stop at 65, but the caring doesn’t.”
Another said:
“We have to shout louder as older women to be heard—and still we aren’t.”
Mary acknowledged the seriousness of these issues and committed to:
bringing older carers’ concerns into ongoing ToC work
exploring dedicated guidance and better mainstreaming within the ToC standards
sharing good practice on carer contingency planning in upcoming meetings
I also reiterated the group’s role in surfacing policy gaps and influencing future national lobbying.
6.4 Carer Registration & Meeting Access
Several carers raised issues with:
The length of the ToC sign-up form
Not receiving meeting links despite signing up
Verification barriers when joining Teams
Mary agreed to:
review and shorten the form
clarify which fields are optional
address email deliverability issues
adjust MS Teams settings to reduce joining friction while maintaining security
6.5 Concerns About Confidentiality Misuse
One carer reported that in a CQC meeting at an NHS Trust, raising questions about communication was dismissed as “confidentiality”, preventing meaningful dialogue. I then encouraged carers to bring such examples into:
ToC Star peer reviews
Carer involvement forums
Local advocacy routes
He noted that misuse of confidentiality is a common and unacceptable barrier and must be challenged.
6.6 Petition on Antipsychotic Medication Research
Carers highlighted concerns about:
long-term prescribing of antipsychotics
lack of regular medication review
inadequate research into long-term effects
A carer shared a petition calling for investigation of psychiatric medications. Richard noted that he had signed and shared it previously.
7. Closing Remarks
Matthew thanked all attendees for their honesty, passion and persistence:
“Carers’ voices shape policies and improve care. That is exactly what this group is here to do.”
Mary acknowledged:
the importance of every concern raised
the need to better support older carers
improvements to ToC communications and meeting accessibility
that the next meeting will be in January (provisionally 19th)
The meeting closed with gratitude from carers who said they felt heard, supported, and connected.
by Matthew McKenzie – National Ethnic Mental Health Carer Forum Chair
In August, the online National Ethnic Mental Health Carer Forum came together once again to confront difficult but necessary conversations about systemic racism, discrimination, and the experiences of ethnic minority carers within health and social care. The forum, hosted by Matthew McKenzie, provided a platform for carers, professionals, and researchers to share insights, frustrations, and plans for change.
Focus on Racism and Discrimination
This month’s forum was unflinching in its focus: racism in health and mental health systems. Attendees shared powerful testimonies of racial abuse and discrimination, highlighting how these experiences undermine trust in services and affect both carers and those they support. There was a clear call for honesty – participants stressed the importance of naming racism directly, rather than disguising it behind euphemisms.
The group also discussed the overrepresentation of Black and brown people in prisons, the lack of tailored initiatives for older Black carers, and the persistent inequalities faced by ethnic minority families trying to navigate mental health and social care support.
Research and Evidence from Carers Trust
A key presentation came from Andrew of Carers Trust, who shared research into the barriers faced by Black, Asian, and minoritised ethnic carers. The findings highlighted widespread issues: discrimination, language barriers, lack of cultural competence, and difficulties in accessing benefits. Andrew emphasised the need for culturally inclusive services and stronger outreach strategies, while acknowledging feedback from the forum that research and advocacy must be explicit about racism rather than avoiding the term.
Andrew expanded on the importance of equity in benefit advice, pointing out that many carers miss out on their entitlements because information is inaccessible, overly complex, or not communicated in culturally relevant ways. He called for dedicated advice services that are not only multilingual but also sensitive to carers who may not self-identify as such.
He also spoke about the impact of social isolation on carers from ethnic minority backgrounds, who often have fewer support networks and face stigma within their own communities. Addressing this requires building trust with local organisations and ensuring carer support is visible in spaces where communities already gather, such as faith centres or community hubs.
Finally, Andrew outlined the Carers Trust’s national strategy, which involves working more closely with local carer organisations, producing research that amplifies marginalised voices, and lobbying for systemic reforms. He highlighted how this forum’s feedback directly shapes their advocacy, showing a real commitment to partnership.
Questions raised during Carers Trust’s presentation:
How can Carers Trust ensure its research explicitly names racism rather than using softer language?
What specific support can be offered to carers who do not self-identify as carers and miss out on benefits?
How can Carers Trust improve its complaints handling processes, particularly for carers facing racism and discrimination?
What role can MPs and lobbying groups play in supporting Carers Trust’s advocacy for ethnic minority carers?
How will Carers Trust ensure its multilingual materials are distributed widely enough to reach isolated communities?
Hampshire & Isle of Wight NHS Anti-Racism Initiatives
Usually NHS Mental Health trust representatives update on anti-racism initiatives at the forum. This time Hampshire and Isle of Wight engaged with minority carers.
Elton who is the Diversity and Inclusion Partner from Hampshire and Isle of Wight NHS Trust provided an update on their anti-racist programmes, including the rollout of the Patient and Carer Race Equality Framework (PCREF). The trust has begun implementing cultural competence training, engaging with local communities, and embedding anti-racism into its wider mental health services. While early in its journey, the trust is already seeing changes in communication and engagement across different wards and services.
Elton shared that the trust is actively developing training modules on implicit bias, with the aim of reaching every staff member across its services. This training is intended not as a one-off exercise but as part of a sustained culture change programme. Early feedback from staff has been encouraging, with more frontline workers recognising how unconscious bias can influence treatment decisions.
He also described the trust’s efforts to engage directly with service users and carers, ensuring that their lived experiences feed into decision-making. Listening events, surveys, and advisory panels are being used to capture diverse perspectives, with a particular focus on groups who historically felt excluded from consultation.
In addition, Elton emphasised the need for transparency and accountability. The trust will publish regular updates on its PCREF action plan, allowing communities and stakeholders to scrutinise progress. He acknowledged that this is just the beginning, but stressed that embedding anti-racism into healthcare systems requires openness, humility, and sustained commitment.
Participants raised questions about how these initiatives address specific groups, such as older Black carers and prisoners’ families, as well as concerns about public misconceptions of anti-racism work. Elton acknowledged these challenges and committed to following up with colleagues on gaps raised during the discussion.
Questions raised during NHS Trust’s presentation:
How will PCREF specifically address the needs of older Black adults who often feel invisible in services?
What is being done to support the mental health of prisoners (e.g. Albany and Parkhurst prisons) and their families within this anti-racist framework?
How will the trust prevent the public misconception that PCREF “excludes” white people?
What mechanisms are in place to ensure transparency and accountability in publishing progress updates?
How will the trust measure the long-term impact of cultural competence and implicit bias training?
Academic Research Contributions
The forum also heard from Shylet, a PhD researcher from University of Glasgow, who is focusing on learning disabilities. She presented her work on the lived experiences of Black African families caring for adults with learning disabilities, and invited participants to take part in interviews. Their contributions highlighted the importance of academic research in documenting and amplifying carers’ lived realities.
Another important theme was the financial challenges facing carers. The group discussed the complexity of benefits like Carer’s Allowance and how misinformation or fear of losing other entitlements often deters carers from claiming support. A carer expressed reluctance to claim due to concerns about how it might affect their relative’s benefits, while another highlighted the importance of valuing one’s own contribution and recognising caring work. There was frustration with bureaucratic systems that seem designed to exclude, particularly when layered with the additional barriers of language, culture, and discrimination.
Carers also highlighted the immense value of unpaid care, with estimates placing its worth at over £180 billion per year if it were to be paid for by the NHS. This figure underscored the urgent need for better recognition and support of carers’ contributions.
Strengthening Complaints and Accountability
There was a debate around how carers can raise complaints when faced with racism or poor treatment. Many participants expressed a lack of trust in formal systems like the CQC or Ombudsman, feeling that complaints disappear into bureaucracy without change. Suggestions included working with MPs, lobbying groups, or the media to ensure voices are heard.
Final Reflections
The August forum showed once again how necessary it is to hold these difficult conversations. Carers spoke bravely about racism and exclusion, professionals shared updates on anti-racist strategies, and researchers sought to bring lived experience into policy. Yet the message was clear: systemic change requires more than frameworks and research reports. It requires honesty, collaboration, and persistence.
As host, I was encouraged by the passion and determination in the room. The forum continues to grow as a national voice for ethnic minority carers, and our commitment to addressing racism head-on remains at the heart of this work.
LLS Carers Forum – July Update: Voices, Concerns & Community Strength
Welcome to the July update for the Lewisham, Lambeth, and Southwark Mental Health Carers Forum. This month’s meeting, chaired by Matthew McKenzie, provided space for powerful updates, critical reflections, and a sobering insight into national developments affecting carer support.
🔸 Growing the Carers Voice
Our forum continues to evolve, bringing together unpaid carers from across boroughs. It remains a space for empowerment, where carers can speak openly, challenge services, and influence support structures. Several attendees introduced themselves and reflected on their caring roles, often crossing borough boundaries and facing ongoing questions about their own place in the system.
🔸 Spotlight: Healthwatch Update
One of the major concerns raised was the planned abolition of Healthwatch England and its local branches, which is a development that has deeply unsettled many in our community.
Anna from Healthwatch Lambeth joined us (on her day off—thank you, Anne!) to explain what’s happening:
Healthwatch functions—listening to service users, signposting, and enter-and-view visits, which are set to be absorbed by local authorities and ICBs.
As a statutory body, Healthwatch cannot be dissolved without legislation, so operations continue for now.
Carers voiced serious concerns over the loss of Healthwatch’s independence and trust, especially as a safe channel for feedback.
Anne reminded us: Healthwatch is still active and listening. A final report on black men’s experiences in Lambeth mental health services is due by mid-August.
🔸 Key Questions Raised
How will services preserve independent feedback mechanisms once Healthwatch is gone?
What accountability structures will replace them?
What are the implications of the broader wave of health service body consolidations?
🔸 Updates from the Ground
We also heard from other carer members:
A carer from Lewisham shared feedback she submitted to the Lewisham Unpaid Carers Forum regarding carer engagement, with little response so far unfortunately highlighting an all-too-common issue.
Other Carers reflected on Lambeth’s carer engagement structures, noting some decline in carer-led decision-making over the years.
Another Carer emphasized the importance of real, consistent carer champions within NHS teams particularly in mental health crisis services.
🔸 Carers Forum Reflections
Matthew provided a helpful comparison between Lewisham and Lambeth carer engagement models. While Lewisham has a formal Unpaid Carers Forum, its independence is limited. Lambeth’s model leans more on the collaborative network and carer support groups. Both boroughs face challenges in consistency, clarity, and co-production.
A concern raised repeatedly: carer champions are often named but rarely visible and sometimes, not even known by their own teams.
📅 Next Forum: August 25 or 26
Due to the bank holiday, the next forum will likely be held on August 26. We’ll aim to have a guest speaker and will explore new ways for carers to hold services to account especially in light of the potential Healthwatch closure.
If you’d like to contribute to future discussions or attend the next forum, please reach out. This is your space.
📣 Let’s continue to speak up, stand together, and push for better mental health support for all carers.