By Matthew McKenzie – Chair of Carers Hospital Discharge group
Thanks to everyone who attended our July Hospital Carer Discharge Meeting. We welcomed representatives from NHS trusts, local authorities, carers organisations, Healthwatch, and voluntary sector partners from across London. As always, the purpose of the meeting was to share developments, learn from each other’s work, and strengthen collaboration to improve hospital experiences and discharge planning for unpaid carers.
Although every organisation is at a different stage of development, one message came through very clearly: supporting unpaid carers is becoming an increasingly important priority across hospitals, councils and the NHS.
A Strong Focus on Earlier Carer Identification
One of the recurring themes throughout the meeting was the importance of identifying carers as early as possible during a patient’s hospital journey.

Many hospitals continue to recognise that carers are often identified too late—sometimes only when discharge is already taking place. Earlier identification allows staff to:
- involve carers in care planning
- understand the practical support available at home
- recognise carers’ own support needs
- prevent unsafe or delayed discharges
- improve communication between hospital teams and families.
Lewisham & Greenwich NHS Trust provided an update on its Standard Operating Procedure (SOP) designed to improve the identification and involvement of unpaid carers. Although implementation has been delayed because of competing organisational priorities, the framework remains in place and includes:
- earlier identification of carers on admission
- recording carers within hospital systems
- involving carers in discharge planning
- ensuring carers understand care needs following discharge
- connecting carers with local authority assessments and community support.
Alongside this, the Trust continues reviewing its Carers Charter and strengthening relationships with voluntary organisations across Lewisham, Greenwich and Bexley to improve partnership working. Training for ward staff is also beginning with support from local councils to improve awareness of carers and available services.
This demonstrates that improving hospital discharge is not simply about creating new policies, but embedding carer awareness throughout everyday clinical practice.
Excellent Examples of Partnership Working
Several organisations shared encouraging examples of collaboration across health and social care.
The North Central London Carer Support Project described a wide range of initiatives already underway across several NHS trusts.
These include:
- weekly co-delivered carer awareness sessions with Camden Carers at University College London Hospital
- regular online training sessions at Whittington Hospital attracting around forty staff members each session
- development of an e-learning programme for professionals working with carers
- greater involvement of patient experience teams in monitoring referrals to carers organisations.

Particularly encouraging was the decision to begin monitoring hospital referral numbers to carers organisations as a performance measure. Measuring referrals each month provides a practical way of understanding whether carers are actually being identified and connected to support rather than relying solely on policy documents.
Camden Carers also highlighted continued outreach into GP surgeries through dedicated engagement work, recognising that many carers first come into contact with primary care long before hospital admission.
Learning from Cancer Carers
Healthwatch representatives shared plans for a significant research project exploring the experiences of carers supporting someone with cancer. The study is expected to begin later this year and will gather the views of carers across several London boroughs before producing recommendations for NHS trusts and publishing the findings publicly. The aim is to better understand what is working well for carers, where support can be strengthened, and how healthcare services can respond more effectively to the realities faced by those caring for someone undergoing cancer treatment.
The discussion highlighted the importance of ensuring that the voices of unpaid carers are heard throughout the research process. Caring for someone with cancer can involve navigating complex treatment pathways, managing appointments across multiple services, providing emotional support, and balancing caring responsibilities alongside work and family life. Research such as this provides an opportunity to capture those lived experiences and translate them into practical recommendations that can improve communication, discharge planning, access to information, and the support available to carers across NHS services.
As Chair of the Cancer Caregiver Forum, I also highlighted opportunities for researchers and NHS organisations to work more closely with existing cancer carer networks to ensure lived experience remains central to future improvements.
Hospital Discharge Remains a National Priority
Several organisations reflected on how hospital discharge continues to be one of the biggest concerns raised by unpaid carers.
Chelsea and Westminster Hospital NHS Foundation Trust
Chelsea and Westminster Hospital explained that feedback from carers is regularly discussed through its Patient Experience Group, with hospital discharge continuing to be one of the most common issues raised by families. Representatives acknowledged that while significant work has taken place, there remains more to do to ensure carers are consistently recognised, listened to, and involved throughout a patient’s stay in hospital.
The Trust also highlighted the important role that carers play in shaping future improvements. By regularly hearing directly from carers through patient experience forums, the hospital is building a better understanding of the practical challenges families face before, during and after discharge. Although their Carers Lead was unable to attend this meeting, the Trust expressed a strong commitment to continuing engagement with regional partners and learning from initiatives taking place across London to strengthen discharge planning and carer support.
Richmond Carers Centre
Richmond Carers Centre reported strong referral links with Kingston Hospital, particularly through dementia services, while also developing opportunities for joint education sessions where hospital staff and carers can better understand each other’s experiences of discharge planning.
Alongside its close working relationship with Kingston Hospital, Richmond Carers Centre continues to raise professional awareness across the borough, encouraging more organisations to identify unpaid carers and refer them for support. The team reflected on ideas gathered from national conferences, including improving engagement with diverse communities and strengthening links with GP practices and Primary Care Networks. Although capacity remains a challenge, Richmond Carers Centre continues to explore new ways of increasing visibility so that carers receive information, advice and emotional support as early as possible rather than only after a hospital discharge has taken place.
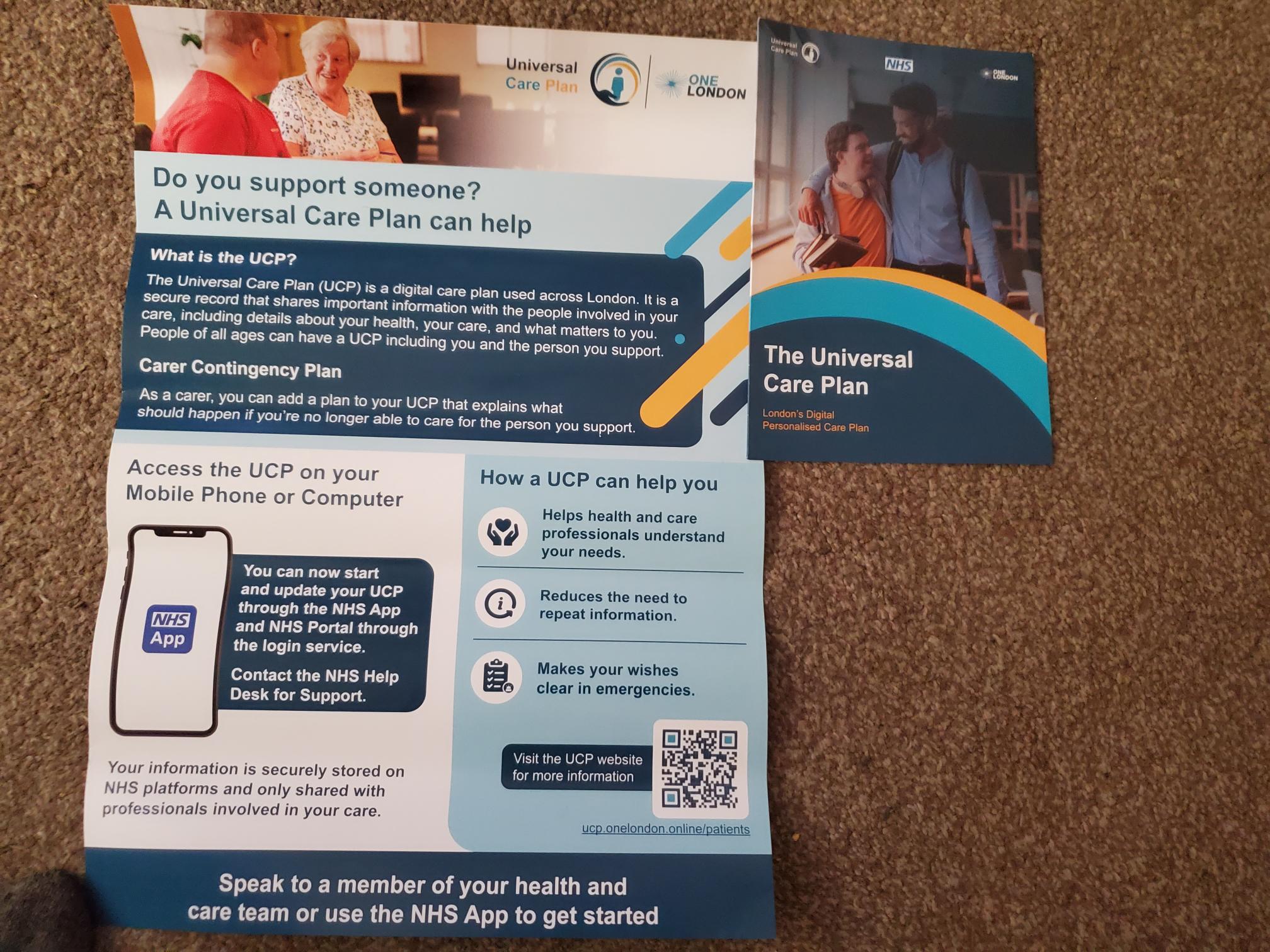
Universal Care Plan and Care Contingency Plan (UCP/CCP)
An important update was shared regarding the Universal Care Plan (UCP) and Care Contingency Plan (CCP), which are being developed through NHS England to improve how carers are identified and supported across health services. Attendees heard that the programme is currently being piloted in London and aims to allow unpaid carers to record emergency contingency arrangements and important caring information digitally through the NHS App and GP systems. The long-term ambition is for this information to be accessible across different parts of the NHS, helping professionals better understand both the needs of the person receiving care and the vital role played by their unpaid carer. Representatives who attended the recent NHS England workshop described the programme as a positive and promising development, with training opportunities expected to become available as the rollout progresses.
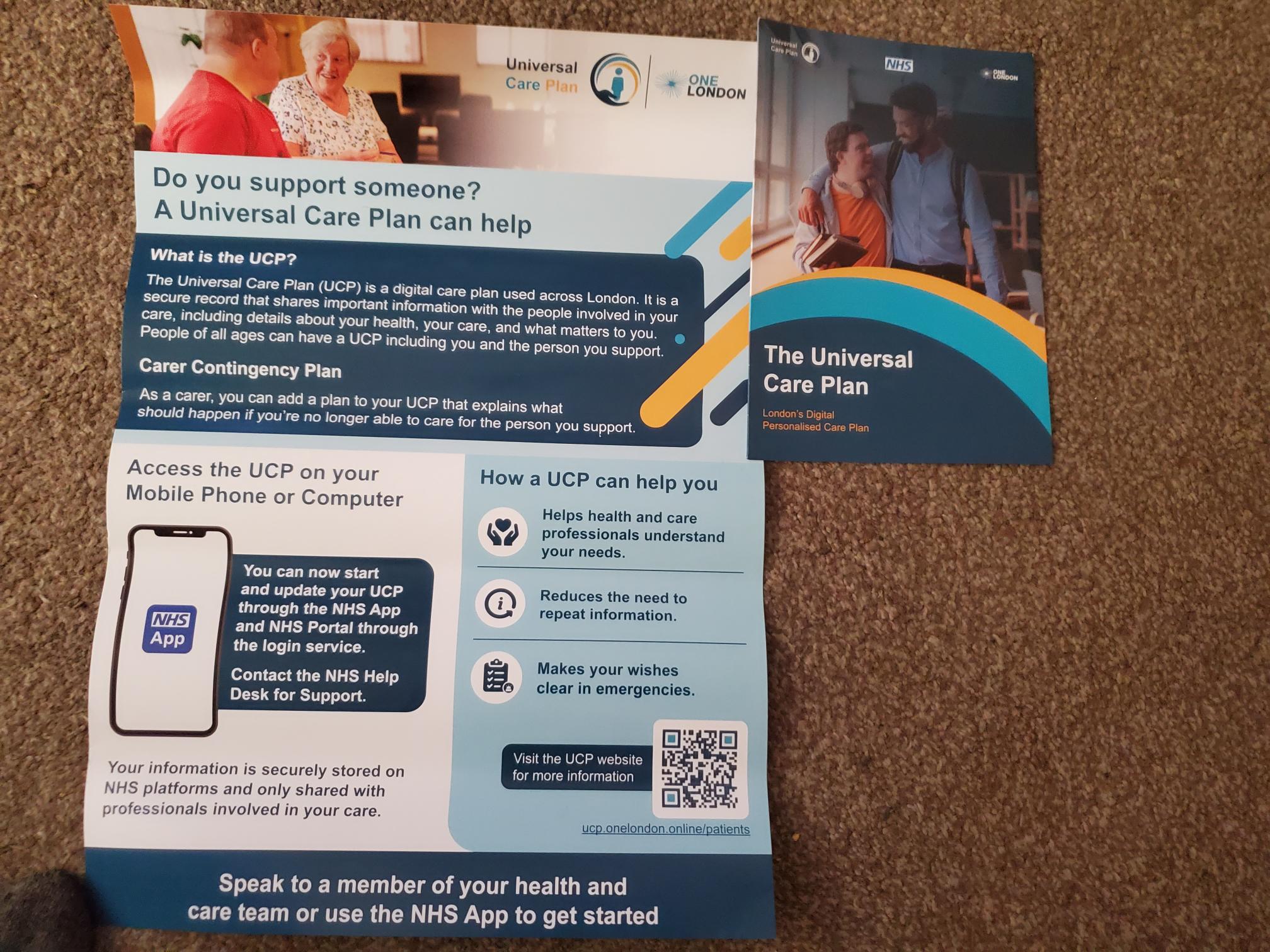
The discussion also highlighted that increasing awareness will be just as important as the technology itself. Many carers remain unaware that care planning and contingency planning can help prepare for emergencies where they may suddenly be unable to provide care. By encouraging hospitals, GP practices and carers organisations to promote the Universal Care Plan and Care Contingency Plan, there is an opportunity to improve continuity of care, reduce avoidable crises, and ensure that carers’ knowledge and wishes are better recognised within the wider health and care system. As these initiatives develop, organisations across London will have an important role in helping carers understand how to access and make effective use of these new digital planning tools.
Southwark Council
Southwark Council also described ongoing partnership work with Guy’s & St Thomas’ and King’s College Hospital. King’s College Hospital is currently developing a Care and Support Navigator service designed to support patients while they remain on waiting lists, assist with discharge planning, and improve signposting into community services once patients return home.
The Council explained that while its refreshed Carers Strategy is not solely focused on hospital discharge, close partnership working with local NHS trusts remains a key priority. Through the Southwark Carer Collaborative, which meets quarterly with representatives from King’s College Hospital and Guy’s & St Thomas’, organisations are sharing developments, identifying opportunities for joint working, and ensuring carers remain firmly on the agenda. Southwark also confirmed that the newly launched Cross-Government Unpaid Carers Action Plan is already helping to inform the direction of its refreshed strategy, demonstrating how national policy is beginning to influence local planning and partnership working.
National Developments – A Significant Moment for Unpaid Carers
Perhaps the most significant national development discussed during the meeting was the publication of the UK Government’s first Cross-Departmental Unpaid Carers Action Plan, launched on early July.
Although many details will continue developing over the coming months, the plan represents an important step because responsibility for unpaid carers is now being considered across multiple government departments rather than solely within health and social care.
Key priorities include:
- improving identification of unpaid carers
- increasing referrals into carers support services
- strengthening employment support for working carers
- making greater use of digital systems including the NHS App.
Alongside this sits the development of the Universal Care Plan and Carers Contingency Plan. Early pilots suggest these tools could allow carers to record emergency contingency arrangements and important caring information digitally, making that information more accessible across health services when needed. Training opportunities are expected to become available as the programme expands.
Looking Ahead
Although considerable progress is being made, many of the discussions reinforced that improving hospital discharge requires sustained partnership between NHS trusts, councils, carers organisations and, most importantly, unpaid carers themselves.
Future meetings will continue sharing practical examples of good practice, highlighting successful projects, and identifying opportunities for organisations to learn from one another.
At our September meeting we look forward to welcoming Carers UK, who will provide regarding hospitals and unpaid carers.
Thank you once again to everyone who contributed to the July meeting. Your willingness to share ideas, successes and challenges continues to strengthen our collective efforts to ensure unpaid carers are recognised, valued and fully involved throughout the hospital discharge process.