Blog by Ethnic Mental Health Carer forum Chair – Matthew McKenzie
The May 2026 Ethnic Mental Health Carers Forum brought together carers, researchers, clinicians, community leaders, and representatives from mental health organisations across England. Although attendance was smaller than usual, the discussion was rich, honest, and highly informative, covering Mental Health Act reform, carers’ experiences, service inequalities, innovative approaches to care, and new research opportunities.
For those who were unable to attend, this blog provides a comprehensive overview of the meeting, including key presentations, audience questions, responses from speakers, and useful resources shared during the session.
Opening Remarks
As the chair, I welcomed attendees and outlined the agenda. The meeting focused on following:
- Mental Health Act research and reform
- Carers’ experiences supporting loved ones through detention
- Findings from a major East Sussex carers research project
- Resources for carers under the Mental Health Act
- Electronic Health Records and future developments
- Wider discussions on racial trauma, inequalities, and service improvement
The meeting also provided opportunities for networking, sharing lived experiences, and highlighting innovative projects happening across the country.
Research Study: Supporting a Loved One Through Mental Health Detention
Dr Maeve Conneely from University College London opened the meeting with a presentation on a new research study exploring the experiences of people who have been assessed or detained under the Mental Health Act, as well as the experiences of family members and carers who supported them through that process. The study has been commissioned as part of the wider programme of Mental Health Act reform and aims to understand how the current “Nearest Relative” provisions operate in practice before changes are introduced under the new legislation.

Dr Conneely explained that researchers are particularly interested in hearing from carers who were involved in supporting a loved one but who were not formally recognised as the “Nearest Relative” under the existing legal framework. She highlighted that these experiences are especially important because they can reveal where carers have been excluded from decision-making, denied access to information, or prevented from contributing to assessments despite playing a significant role in supporting the individual concerned. The study is open to anyone aged 16 or over who has direct experience of Mental Health Act assessments, detentions, Community Treatment Orders, holding powers, or related interventions, whether as a patient or as a supporter.
The research is linked to ongoing reforms of the Mental Health Act and seeks to understand how the “Nearest Relative” provisions currently operate before changes are implemented.
Who Can Take Part?
The study is looking for:
- People who have been detained under the Mental Health Act
- Family members and carers who supported someone during detention or assessment
- Individuals who should have been involved as a nearest relative but were not
- Anyone aged 16 or over with relevant experience
Interviews are conducted online and participants receive a £30 shopping voucher as a thank-you for their time.
Key Question from Participants
Q: Does the study include situations where someone should have been involved but wasn’t?
Response: Yes. Researchers are particularly interested in understanding experiences where carers or family members were excluded from decision-making processes despite playing a significant caring role.
Another Important Question
Q: Do carers need permission from the person who was detained before participating?
Response: No. Carers are sharing their own experiences and therefore only need to provide their own consent.
Discussion Themes
Participants highlighted:
- Long-standing inequalities affecting Black communities under the Mental Health Act.
- The overuse of psychiatric labels without sufficient exploration of trauma.
- The need to understand why some individuals receive significantly different experiences of care, including access to private mental health facilities.
- Concerns about trust in mental health services and the lasting impact of poor experiences across generations.
Several carers committed to taking part in the study to ensure lived experience informs future policy.
East Sussex Carers Research Project: What Carers Told Us
Age Angiolini presented findings from a year-long carers-led research project examining the experiences of family carers supporting people with serious mental illness across East Sussex. The study was developed in response to repeated concerns raised by carers at local support meetings and sought to capture their experiences of interacting with mental health services provided by the Sussex Partnership Foundation Trust (SPFT).

Although the research received 71 responses, representing only a proportion of the carers population in the region, the findings revealed a striking consistency in the challenges carers face. The survey explored themes including carers’ involvement in care planning, communication with services, consent and confidentiality, quality of care, crisis support, and priorities for improvement. Among the most significant findings were that 72% of carers reported being only sometimes involved or not involved at all in their loved one’s care, 73% felt services relied too heavily on carers, and 72% said they regularly had to advocate to secure appropriate support. The research concluded that many carers feel undervalued, excluded from decision-making, and left carrying significant responsibilities without adequate recognition or support.
The study gathered responses from carers supporting people with:
- Schizophrenia
- Bipolar disorder
- ADHD
- Autism
- Complex neurodiverse conditions
Although the sample size was relatively modest, the findings revealed significant and consistent concerns.
Key Findings from the report
Carers Feel Excluded
- 72% reported being only sometimes involved or not involved at all.
- 73% felt services relied too heavily on carers.
- 72% said they had to advocate strongly to secure appropriate care.

Communication Failures
Participants reported poor communication between:
- Mental health services
- Assessment teams
- Social services
- Mental health liaison teams
Many carers described communications as inconsistent, unclear, and difficult to navigate.
Consent and Confidentiality
A recurring concern was that confidentiality procedures are often applied rigidly, preventing carers from sharing vital information during crises.
Carers argued that this can actively undermine effective care.
Quality of Care Concerns
The research found:
- 90% reported insufficient care.
- Significant concerns around continuity of care.
- A strong desire for dedicated care coordinators.
- Widespread frustration with crisis services.
Crisis Support is Not Working

Many carers reported that:
- NHS 111 is often inadequate for mental health crises.
- A&E is frequently unsuitable for people experiencing mental distress.
- Services remain reactive rather than preventative.
Calls for Change
Recommendations included:
- Better crisis pathways
- Improved coordination between services
- More trauma-informed approaches
- Greater therapeutic support
- Increased family involvement
- Better support for neurodiverse individuals
The presentation sparked considerable discussion, with many attendees noting that the findings reflected experiences they had encountered for years.
Carers Speak Out: Frustration, Trauma and the Need for Change
One of the most powerful aspects of the meeting was hearing directly from carers.
Several participants reflected on decades of involvement with mental health services and expressed concern that despite repeated reviews, consultations, and reforms, many of the same issues continue to persist.
Common themes included:
- Institutional racism
- Poor communication
- Exclusion of carers
- Over-medicalisation
- Lack of trauma-informed care
- Inadequate support during crises
A number of attendees emphasised that families often become de facto care coordinators, managing appointments, services, medications, and crises while receiving little support themselves.
One participant observed:
“They plan, medicate and treat. We care. Our worlds don’t meet.”
Others highlighted the impact of racial trauma and the way mental health services can fail to recognise the cultural context of distress.
Open Dialogue: A Different Way Forward?

Ren Reins introduced the concept of Open Dialogue, an internationally recognised approach to mental health care that focuses on relationships, networks, and collaborative conversations.
Open Dialogue aims to:
- Bring families and professionals together
- Reduce fragmentation between services
- Focus on lived experience
- Build trust
- Improve recovery outcomes
Ren explained that major NHS-funded trials are underway and encouraged carers to learn more about the approach.
The discussion generated significant interest, particularly from attendees looking for alternatives to traditional medical models of care.
Nearest Relative Resources Project
Professor Judy Laing from the University of Bristol provided an update on an innovative project designed to support family members and carers who hold, or may hold, responsibilities under the Mental Health Act’s “Nearest Relative” provisions. Drawing on previous research with carers and mental health professionals, Professor Laing explained that many family members who find themselves in the Nearest Relative role often receive little information, guidance, or emotional support despite carrying significant legal responsibilities. In response, her team secured funding to develop a free, co-produced online resource that helps carers understand their rights, responsibilities, and options when supporting a loved one through mental health assessment, detention, and treatment.

Developed in partnership with carers, family members, mental health professionals, and organisations including Mind, Rethink Mental Illness, and Carers Trust, the website provides practical information, downloadable tools, guidance for conversations with professionals, and resources to help carers look after their own wellbeing. Professor Laing stressed that the project has been shaped directly by the experiences of those who have undertaken the role themselves, ensuring that the guidance reflects the realities and challenges carers face in practice rather than simply explaining legal processes.
The project emerged from research identifying significant gaps in information and support for people carrying out the “Nearest Relative” role.
What Has Been Developed?
The project has created a free online resource containing:
- Information about legal rights
- Guidance on conversations with professionals
- Practical tools for meetings
- Support for carers’ wellbeing
- Resources explaining upcoming legal changes
The materials have been co-produced with carers and family members.
Questions Raised
How are diverse communities included?
Participants asked how the project ensures equity and accessibility.
Professor Laing explained that:
- People from ethnic minority backgrounds have contributed to development.
- Resources are being improved to increase accessibility.
- Additional funding is supporting work around inclusion and accessibility.
- Translation and alternative formats are being explored.
How is the project promoted?
Discussion focused on ensuring communities are aware of available support rather than resources existing only online.
Professor Laing outlined efforts involving:
- Mind
- Carers Trust
- Mental health services
- Local media
- Carer forums
How will the new Nominated Person role protect carers who have traditionally been involved in supporting a loved one?
Several participants expressed concern that replacing the Nearest Relative role could unintentionally weaken the involvement of family members who have historically provided substantial support during periods of mental ill-health. Questions were raised about situations where a person may choose someone other than their primary carer to act as their Nominated Person, potentially reducing carers’ ability to access information or participate in key decisions. Professor Laing acknowledged that these concerns have been raised by many carers and explained that the practical details of how the new system will operate are still being developed. She stressed the importance of carers contributing their experiences to ensure that future guidance recognises the valuable role families often play in supporting recovery and maintaining continuity of care.
What support is available when professionals fail to recognise or understand carers’ legal rights?
Attendees also discussed the reality that many mental health professionals are not always familiar with the legal powers and rights associated with the Nearest Relative role. Participants described situations where carers were excluded from discussions, not informed of important decisions, or felt unable to challenge professional opinions because they lacked confidence in their understanding of the law. In response, Professor Laing highlighted that one of the main objectives of the Bristol resources project is to bridge this knowledge gap by providing practical tools, suggested questions, and clear explanations of carers’ rights. She noted that the project is also developing resources aimed at professionals themselves, with the goal of increasing awareness and ensuring that carers’ legal rights are better understood and respected across mental health services.
Attendees welcomed the commitment to increasing visibility.
Electronic Health Records and Future Developments
Dr Anna De Simoni, an Academic GP and Associate Professor of Primary Care at Queen Mary University of London, presented an early-stage research proposal focused on how electronic health records could be used to better understand and map the social support networks surrounding people living with multiple long-term health conditions.
Dr De Simoni sought direct feedback from carers to help shape the project before a formal funding application is submitted. She explained that while healthcare professionals can usually identify a patient’s next of kin and household members through existing GP records, they often have very limited understanding of the wider support networks that play a vital role in a person’s wellbeing.
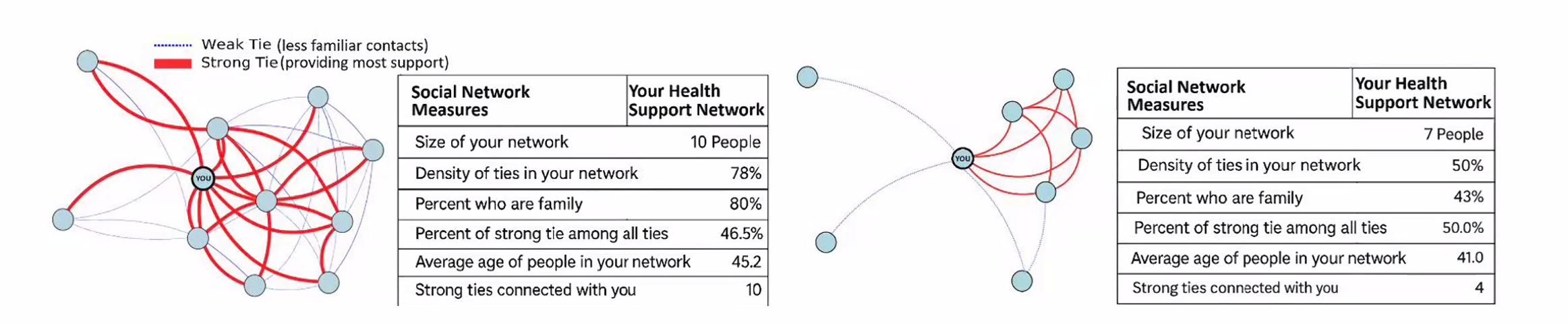
These networks may include family members, neighbours, friends, faith groups, community organisations, carers, and others who provide practical and emotional support. The research aims to explore whether technology and electronic health records can help healthcare professionals better recognise these support systems and use that information to improve care planning, reduce unnecessary hospital admissions, and enhance quality of life for people living with complex health conditions.
The discussion generated considerable interest, particularly regarding:
- Information sharing
- Integration across services
- Support for carers
- Data protection concerns
- Improving continuity of care
Several participants expressed enthusiasm about the potential benefits while also raising questions regarding privacy and access to NHS information.
Questions and Answers from Dr Anna De Simoni’s Presentation
Q: What problem is this research trying to solve?
A: Dr De Simoni explained that healthcare professionals often know very little about the wider support network surrounding a patient. While medical records may identify a next of kin or people living in the same household, they rarely capture the full picture of who is actually providing practical, emotional, or day-to-day support. The project aims to better understand these social networks and use that information to improve care planning and patient outcomes.
Q: Who is the research aimed at?
A: The initial focus is on people living with multiple long-term health conditions, including illnesses such as COPD and other complex health needs e.g mental health. The project seeks to understand how stronger recognition of support networks could improve quality of life, reduce hospital admissions, and support people to remain independent for longer.
Q: How would patients contribute information about their support network?
A: The proposal includes the use of a Universal Care Plan through the NHS App. Patients would be able to enter information themselves about what matters to them, who supports them, how they prefer to be treated, and what should happen if their health deteriorates. This information could then be viewed and updated by relevant healthcare professionals.
Q: What role could carers play within the proposed system?
A: Participants highlighted that carers often provide the majority of practical support but are frequently invisible within healthcare systems. The proposed approach could make carers more visible by helping professionals understand who is involved in supporting a patient and what role they play in maintaining wellbeing and independence.
Q: How will patient confidentiality and data protection be managed?
A: Concerns were raised about privacy and the security of NHS data. Dr De Simoni explained that information governance, GDPR compliance, and data protection would be central to the project. Specialists in privacy and information governance would be involved to ensure that any information collected is handled safely, appropriately, and with proper consent.
Key Discussion: Why Are Carers Still Fighting the Same Battles?
A recurring theme throughout the meeting was the sense that many challenges identified today are the same challenges carers raised ten or twenty years ago.
Questions included:
- Why are services still fragmented?
- Why do carers continue to feel excluded?
- Why are communication problems so persistent?
- Why is trauma often overlooked?
- Why do inequalities remain entrenched?
Participants reflected on whether the issue is primarily one of resources, leadership, service design, or culture.
Many agreed that meaningful change requires carers to remain actively involved in shaping policy and service delivery.
Resources and Links Shared During the Meeting
Mental Health Act Research Study
Email:
nrmha@ucl.ac.uk
Eligibility:
People aged 16+ who have experience supporting someone assessed or detained under the Mental Health Act.
Nearest Relative Resources Website
Nearest Relative Resources Impact Report
POPs Facebook Group
https://www.facebook.com/groups/POPSUnitedKingdom
A carers support group recommended during discussion as a source of peer support and shared experience.
Final Reflections
The May 2026 Ethnic Mental Health Carers Forum highlighted both the challenges carers continue to face and the determination across the sector to improve outcomes.
From Mental Health Act reform and carers’ rights to innovative approaches such as Open Dialogue, the meeting demonstrated the importance of bringing together lived experience, research, policy, and practice.
Several speakers reminded attendees that change often begins with carers sharing their stories, participating in research, challenging poor practice, and helping shape future services.
The forum remains an important space where those voices can be heard.