If you weren’t able to join our June South London Mental Health Carers Group meeting, here’s a summary of the main discussions and updates. As always, the meeting brought together unpaid carers from across Lambeth, Lewisham, Southwark and Croydon to share experiences, raise concerns and keep each other informed about developments affecting mental health carers.
Why these meetings matter
One of the strongest themes throughout the meeting was the importance of carers staying connected. Many carers cannot attend every committee or involvement meeting due to their caring responsibilities, work or other commitments. By sharing updates, we can help ensure everyone remains informed about changes that may affect them and the people they support.
Several carers commented that services sometimes feel like they are “reinventing the wheel”, with the same issues being raised repeatedly. While progress can be slow, continuing to speak up and share experiences remains essential.
Updates from the Maudsley Family and Carers Committee
Carers who attended the latest South London and Maudsley (SLAM) Family and Carers Committee shared several important developments.
Review of the Involvement Register
SLAM is reviewing its Involvement Register over the coming months. Working groups will look at areas including:
Outcomes
How involvement is delivered
Governance and policy
Carers interested in influencing how services engage with families are encouraged to consider joining the register. Participation is flexible, allowing carers to contribute when they are able.
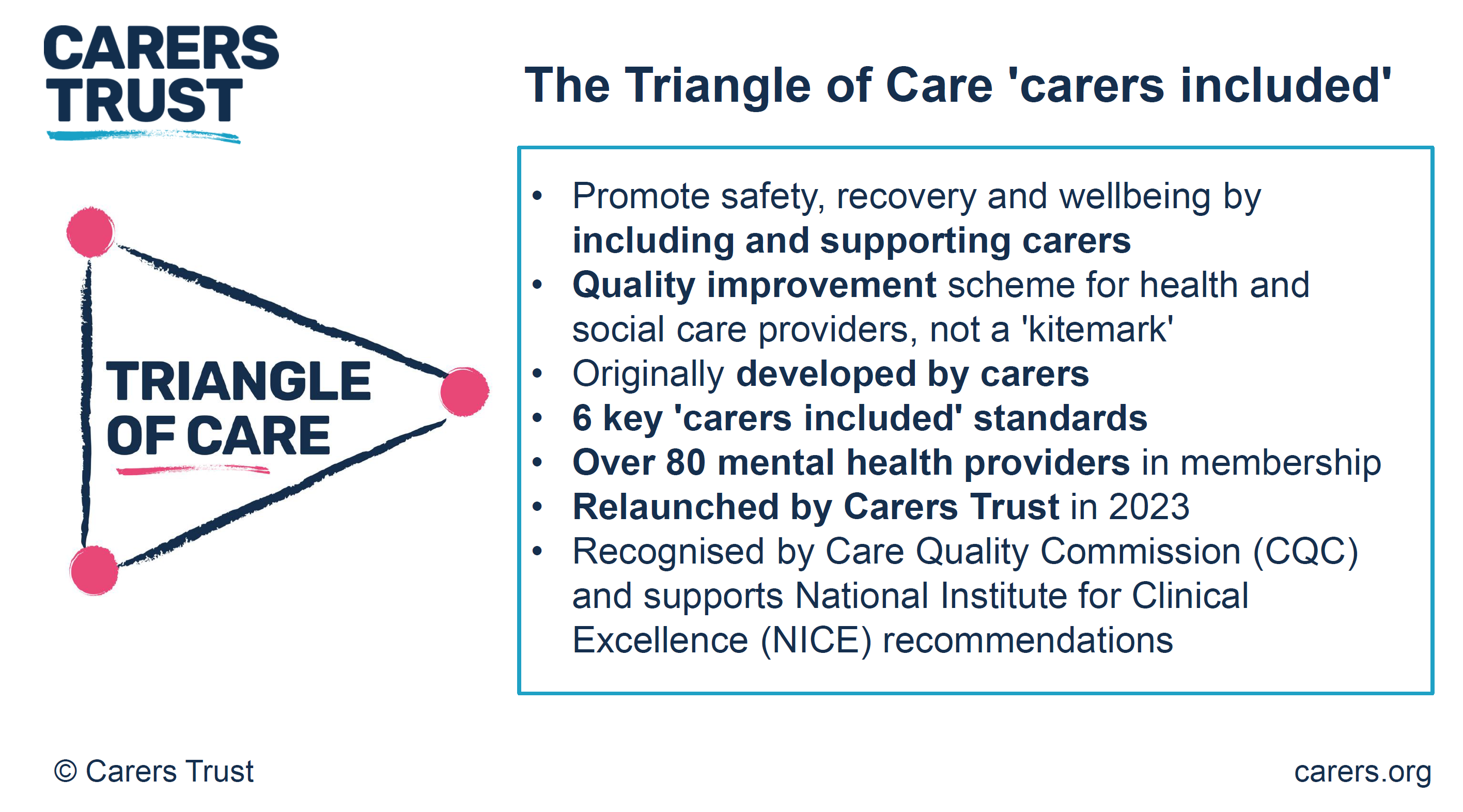
Triangle of Care
The Triangle of Care continues to be a significant focus, particularly around how carers are identified, involved and supported during someone’s mental health care.
Discussions also covered how Trusts monitor their progress and how carers’ details are recorded to ensure families receive appropriate information and support.
Information for carers
Work is continuing to improve the information provided to carers. Rather than relying on a single handbook that can quickly become outdated, there are plans to develop more flexible information resources that can be updated more easily and provided when carers actually need them.
Mental Health Act reforms
A significant part of the meeting focused on the recent changes to the Mental Health Act and what they could mean for unpaid carers.
Key topics included:
Greater emphasis on patient choice and involvement.
The introduction of the Nominated Person, replacing the traditional “Nearest Relative” in many situations.
The importance of Advance Choice Documents, allowing people to record their wishes while they are well.
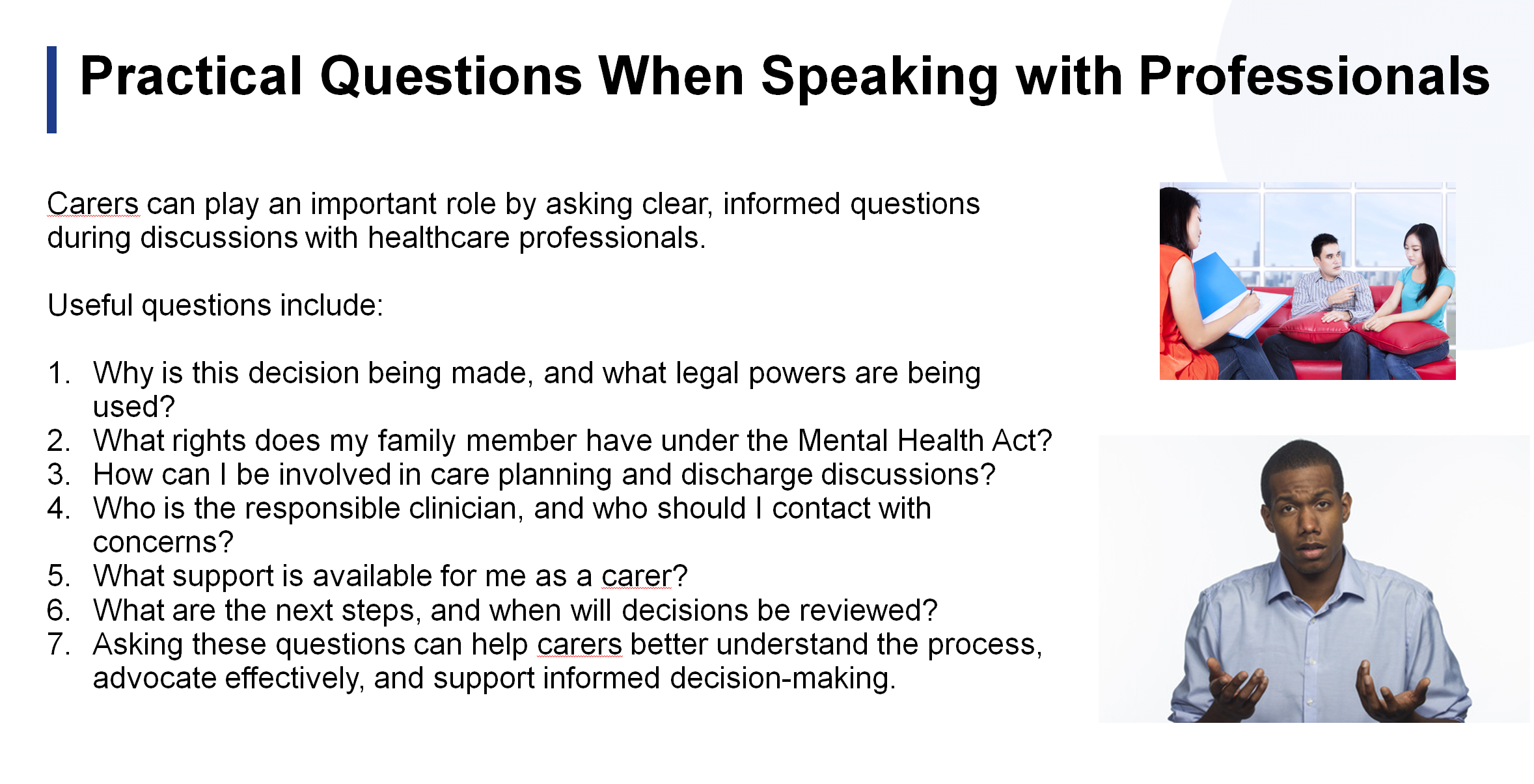
The need for carers to understand their legal rights and ask questions during admissions, treatment planning and discharge.
Carers discussed both the opportunities and concerns arising from these changes, particularly where someone may lose insight during periods of illness. There was broad agreement that carers need clear information about how the reforms will be implemented locally and how families will continue to be involved.
Advocacy and complaints
Members shared experiences of trying to access advocacy services and navigate complaints processes.
Concerns included:
Limited access to independent mental health advocacy in some boroughs.
Unclear complaints pathways.
The need for carers to be listened to, even when confidential information cannot be shared with them.
The importance of raising concerns through appropriate safeguarding and governance routes where necessary.
Several carers also shared positive experiences where persistence had led to improvements in care.
Local updates from across South London
One of the strengths of the South London Mental Health Carers Group is the opportunity for carers from different boroughs to share what is happening locally. While each area faces its own challenges, many of the issues raised were common across South London.
Lambeth
Carers discussed the continuing work of the Lambeth Living Well Collaborative, which brings together carers, service users, voluntary organisations and professionals to improve local mental health services. Members were reminded that carers are welcome to attend collaborative meetings and contribute to discussions about service improvements.
The conversation also recognised the wider pressures affecting carers beyond mental health services. Rising living costs, reductions in council tax support for many working-age residents receiving benefits, and the increasing financial pressures on families continue to affect carers’ wellbeing. These wider social issues inevitably have an impact on people’s ability to sustain their caring role.
Lewisham
Carers provided an update on Lewisham’s Community Mental Health Transformation programme. While work continues to redesign community services, concerns remain about what happens when someone is discharged from specialist mental health services back to primary care.
Several carers highlighted unanswered questions around:
How GPs will be supported to manage people with ongoing severe mental health needs.
What support carers can expect once specialist services are no longer involved.
Whether communication between secondary mental health services and GP practices is sufficiently robust.
These are important questions that carers hope local services will continue to address as transformation plans progress.
Croydon and Lewisham carer information
Members also heard that new information resources for carers are being developed in Croydon and Lewisham. Rather than relying on lengthy booklets, services are creating a series of practical information sheets covering different aspects of mental health care. This approach should allow information to be updated more regularly and provided when carers need it most.
Carers welcomed this change, noting that people often need specific information at different stages of their caring journey rather than receiving a large handbook all at once.
The important role of GP practices
An interesting discussion focused on the role of GP practices in supporting unpaid carers.
Members recognised that experiences vary considerably between surgeries. Some GP practices have developed strong support for carers, while others still have some way to go.
One positive example shared was Wells Park Practice, where carers have become actively involved in developing support, including helping to establish a regular carers’ coffee morning. This demonstrates what can be achieved when GP practices actively engage with carers and recognise the valuable role they play.
The meeting reinforced several practical messages for carers:
Make sure your GP practice knows that you are an unpaid carer and ask to be recorded on their carers register.
Ask what support your surgery offers to carers, including health checks, referrals or local support groups.
If your current practice offers limited support for carers, it may be worth exploring what neighbouring GP practices provide, particularly if they have developed a stronger carers programme.
As community mental health services increasingly work alongside primary care, ensuring that GP practices recognise and support unpaid carers is becoming more important than ever.
Learning from each other
Perhaps the most valuable part of the local updates was hearing how carers are finding solutions in different boroughs. Good practice in one area can often inspire improvements elsewhere.
Whether discussing carers’ information, community transformation, GP engagement or involvement opportunities, the message was clear: carers’ experiences are a vital source of learning, and sharing those experiences helps improve services across South London as a whole.
Looking ahead
One of the biggest messages from the meeting was that carers have valuable lived experience that services need to hear. Whether through local carers’ centres, involvement registers, Trust committees or community groups, every contribution helps shape future services.
If you are interested in becoming more involved but can only contribute occasionally, don’t let that put you off. Many opportunities allow carers to participate as much or as little as their circumstances allow.
Thank you to everyone who attended and contributed so openly. Your experiences continue to help improve understanding and influence services across South London.
We look forward to welcoming both new and returning carers to our next meeting.
Blog by Ethnic Mental Health Carer forum Chair – Matthew McKenzie
The May 2026 Ethnic Mental Health Carers Forum brought together carers, researchers, clinicians, community leaders, and representatives from mental health organisations across England. Although attendance was smaller than usual, the discussion was rich, honest, and highly informative, covering Mental Health Act reform, carers’ experiences, service inequalities, innovative approaches to care, and new research opportunities.
For those who were unable to attend, this blog provides a comprehensive overview of the meeting, including key presentations, audience questions, responses from speakers, and useful resources shared during the session.
Opening Remarks
As the chair, I welcomed attendees and outlined the agenda. The meeting focused on following:
Mental Health Act research and reform
Carers’ experiences supporting loved ones through detention
Findings from a major East Sussex carers research project
Resources for carers under the Mental Health Act
Electronic Health Records and future developments
Wider discussions on racial trauma, inequalities, and service improvement
The meeting also provided opportunities for networking, sharing lived experiences, and highlighting innovative projects happening across the country.
Research Study: Supporting a Loved One Through Mental Health Detention
Dr Maeve Conneely from University College London opened the meeting with a presentation on a new research study exploring the experiences of people who have been assessed or detained under the Mental Health Act, as well as the experiences of family members and carers who supported them through that process. The study has been commissioned as part of the wider programme of Mental Health Act reform and aims to understand how the current “Nearest Relative” provisions operate in practice before changes are introduced under the new legislation.
Dr Conneely explained that researchers are particularly interested in hearing from carers who were involved in supporting a loved one but who were not formally recognised as the “Nearest Relative” under the existing legal framework. She highlighted that these experiences are especially important because they can reveal where carers have been excluded from decision-making, denied access to information, or prevented from contributing to assessments despite playing a significant role in supporting the individual concerned. The study is open to anyone aged 16 or over who has direct experience of Mental Health Act assessments, detentions, Community Treatment Orders, holding powers, or related interventions, whether as a patient or as a supporter.
The research is linked to ongoing reforms of the Mental Health Act and seeks to understand how the “Nearest Relative” provisions currently operate before changes are implemented.
Who Can Take Part?
The study is looking for:
People who have been detained under the Mental Health Act
Family members and carers who supported someone during detention or assessment
Individuals who should have been involved as a nearest relative but were not
Anyone aged 16 or over with relevant experience
Interviews are conducted online and participants receive a £30 shopping voucher as a thank-you for their time.
Key Question from Participants
Q: Does the study include situations where someone should have been involved but wasn’t?
Response: Yes. Researchers are particularly interested in understanding experiences where carers or family members were excluded from decision-making processes despite playing a significant caring role.
Another Important Question
Q: Do carers need permission from the person who was detained before participating?
Response: No. Carers are sharing their own experiences and therefore only need to provide their own consent.
Discussion Themes
Participants highlighted:
Long-standing inequalities affecting Black communities under the Mental Health Act.
The overuse of psychiatric labels without sufficient exploration of trauma.
The need to understand why some individuals receive significantly different experiences of care, including access to private mental health facilities.
Concerns about trust in mental health services and the lasting impact of poor experiences across generations.
Several carers committed to taking part in the study to ensure lived experience informs future policy.
East Sussex Carers Research Project: What Carers Told Us
Age Angiolini presented findings from a year-long carers-led research project examining the experiences of family carers supporting people with serious mental illness across East Sussex. The study was developed in response to repeated concerns raised by carers at local support meetings and sought to capture their experiences of interacting with mental health services provided by the Sussex Partnership Foundation Trust (SPFT).
Although the research received 71 responses, representing only a proportion of the carers population in the region, the findings revealed a striking consistency in the challenges carers face. The survey explored themes including carers’ involvement in care planning, communication with services, consent and confidentiality, quality of care, crisis support, and priorities for improvement. Among the most significant findings were that 72% of carers reported being only sometimes involved or not involved at all in their loved one’s care, 73% felt services relied too heavily on carers, and 72% said they regularly had to advocate to secure appropriate support. The research concluded that many carers feel undervalued, excluded from decision-making, and left carrying significant responsibilities without adequate recognition or support.
The study gathered responses from carers supporting people with:
Schizophrenia
Bipolar disorder
ADHD
Autism
Complex neurodiverse conditions
Although the sample size was relatively modest, the findings revealed significant and consistent concerns.
Key Findings from the report
Carers Feel Excluded
72% reported being only sometimes involved or not involved at all.
73% felt services relied too heavily on carers.
72% said they had to advocate strongly to secure appropriate care.
Communication Failures
Participants reported poor communication between:
Mental health services
Assessment teams
Social services
Mental health liaison teams
Many carers described communications as inconsistent, unclear, and difficult to navigate.
Consent and Confidentiality
A recurring concern was that confidentiality procedures are often applied rigidly, preventing carers from sharing vital information during crises.
Carers argued that this can actively undermine effective care.
Quality of Care Concerns
The research found:
90% reported insufficient care.
Significant concerns around continuity of care.
A strong desire for dedicated care coordinators.
Widespread frustration with crisis services.
Crisis Support is Not Working
Many carers reported that:
NHS 111 is often inadequate for mental health crises.
A&E is frequently unsuitable for people experiencing mental distress.
Services remain reactive rather than preventative.
Calls for Change
Recommendations included:
Better crisis pathways
Improved coordination between services
More trauma-informed approaches
Greater therapeutic support
Increased family involvement
Better support for neurodiverse individuals
The presentation sparked considerable discussion, with many attendees noting that the findings reflected experiences they had encountered for years.
Carers Speak Out: Frustration, Trauma and the Need for Change
One of the most powerful aspects of the meeting was hearing directly from carers.
Several participants reflected on decades of involvement with mental health services and expressed concern that despite repeated reviews, consultations, and reforms, many of the same issues continue to persist.
Common themes included:
Institutional racism
Poor communication
Exclusion of carers
Over-medicalisation
Lack of trauma-informed care
Inadequate support during crises
A number of attendees emphasised that families often become de facto care coordinators, managing appointments, services, medications, and crises while receiving little support themselves.
One participant observed:
“They plan, medicate and treat. We care. Our worlds don’t meet.”
Others highlighted the impact of racial trauma and the way mental health services can fail to recognise the cultural context of distress.
Open Dialogue: A Different Way Forward?
Ren Reins introduced the concept of Open Dialogue, an internationally recognised approach to mental health care that focuses on relationships, networks, and collaborative conversations.
Open Dialogue aims to:
Bring families and professionals together
Reduce fragmentation between services
Focus on lived experience
Build trust
Improve recovery outcomes
Ren explained that major NHS-funded trials are underway and encouraged carers to learn more about the approach.
The discussion generated significant interest, particularly from attendees looking for alternatives to traditional medical models of care.
Nearest Relative Resources Project
Professor Judy Laing from the University of Bristol provided an update on an innovative project designed to support family members and carers who hold, or may hold, responsibilities under the Mental Health Act’s “Nearest Relative” provisions. Drawing on previous research with carers and mental health professionals, Professor Laing explained that many family members who find themselves in the Nearest Relative role often receive little information, guidance, or emotional support despite carrying significant legal responsibilities. In response, her team secured funding to develop a free, co-produced online resource that helps carers understand their rights, responsibilities, and options when supporting a loved one through mental health assessment, detention, and treatment.
Developed in partnership with carers, family members, mental health professionals, and organisations including Mind, Rethink Mental Illness, and Carers Trust, the website provides practical information, downloadable tools, guidance for conversations with professionals, and resources to help carers look after their own wellbeing. Professor Laing stressed that the project has been shaped directly by the experiences of those who have undertaken the role themselves, ensuring that the guidance reflects the realities and challenges carers face in practice rather than simply explaining legal processes.
The project emerged from research identifying significant gaps in information and support for people carrying out the “Nearest Relative” role.
What Has Been Developed?
The project has created a free online resource containing:
Information about legal rights
Guidance on conversations with professionals
Practical tools for meetings
Support for carers’ wellbeing
Resources explaining upcoming legal changes
The materials have been co-produced with carers and family members.
Questions Raised
How are diverse communities included?
Participants asked how the project ensures equity and accessibility.
Professor Laing explained that:
People from ethnic minority backgrounds have contributed to development.
Resources are being improved to increase accessibility.
Additional funding is supporting work around inclusion and accessibility.
Translation and alternative formats are being explored.
How is the project promoted?
Discussion focused on ensuring communities are aware of available support rather than resources existing only online.
Professor Laing outlined efforts involving:
Mind
Carers Trust
Mental health services
Local media
Carer forums
How will the new Nominated Person role protect carers who have traditionally been involved in supporting a loved one?
Several participants expressed concern that replacing the Nearest Relative role could unintentionally weaken the involvement of family members who have historically provided substantial support during periods of mental ill-health. Questions were raised about situations where a person may choose someone other than their primary carer to act as their Nominated Person, potentially reducing carers’ ability to access information or participate in key decisions. Professor Laing acknowledged that these concerns have been raised by many carers and explained that the practical details of how the new system will operate are still being developed. She stressed the importance of carers contributing their experiences to ensure that future guidance recognises the valuable role families often play in supporting recovery and maintaining continuity of care.
What support is available when professionals fail to recognise or understand carers’ legal rights?
Attendees also discussed the reality that many mental health professionals are not always familiar with the legal powers and rights associated with the Nearest Relative role. Participants described situations where carers were excluded from discussions, not informed of important decisions, or felt unable to challenge professional opinions because they lacked confidence in their understanding of the law. In response, Professor Laing highlighted that one of the main objectives of the Bristol resources project is to bridge this knowledge gap by providing practical tools, suggested questions, and clear explanations of carers’ rights. She noted that the project is also developing resources aimed at professionals themselves, with the goal of increasing awareness and ensuring that carers’ legal rights are better understood and respected across mental health services.
Attendees welcomed the commitment to increasing visibility.
Electronic Health Records and Future Developments
Dr Anna De Simoni, an Academic GP and Associate Professor of Primary Care at Queen Mary University of London, presented an early-stage research proposal focused on how electronic health records could be used to better understand and map the social support networks surrounding people living with multiple long-term health conditions.
Dr De Simoni sought direct feedback from carers to help shape the project before a formal funding application is submitted. She explained that while healthcare professionals can usually identify a patient’s next of kin and household members through existing GP records, they often have very limited understanding of the wider support networks that play a vital role in a person’s wellbeing.
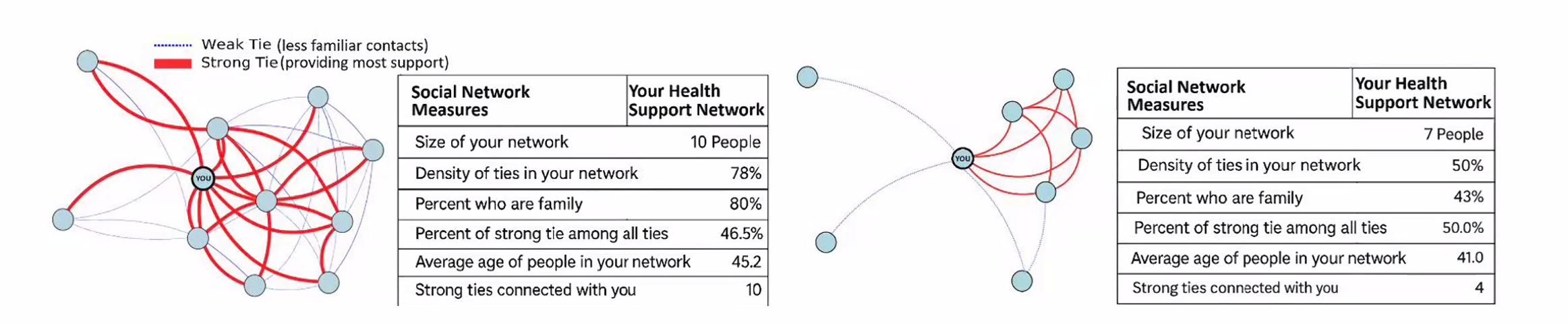
These networks may include family members, neighbours, friends, faith groups, community organisations, carers, and others who provide practical and emotional support. The research aims to explore whether technology and electronic health records can help healthcare professionals better recognise these support systems and use that information to improve care planning, reduce unnecessary hospital admissions, and enhance quality of life for people living with complex health conditions.
The discussion generated considerable interest, particularly regarding:
Information sharing
Integration across services
Support for carers
Data protection concerns
Improving continuity of care
Several participants expressed enthusiasm about the potential benefits while also raising questions regarding privacy and access to NHS information.
Questions and Answers from Dr Anna De Simoni’s Presentation
Q: What problem is this research trying to solve? A: Dr De Simoni explained that healthcare professionals often know very little about the wider support network surrounding a patient. While medical records may identify a next of kin or people living in the same household, they rarely capture the full picture of who is actually providing practical, emotional, or day-to-day support. The project aims to better understand these social networks and use that information to improve care planning and patient outcomes.
Q: Who is the research aimed at? A: The initial focus is on people living with multiple long-term health conditions, including illnesses such as COPD and other complex health needs e.g mental health. The project seeks to understand how stronger recognition of support networks could improve quality of life, reduce hospital admissions, and support people to remain independent for longer.
Q: How would patients contribute information about their support network? A: The proposal includes the use of a Universal Care Plan through the NHS App. Patients would be able to enter information themselves about what matters to them, who supports them, how they prefer to be treated, and what should happen if their health deteriorates. This information could then be viewed and updated by relevant healthcare professionals.
Q: What role could carers play within the proposed system? A: Participants highlighted that carers often provide the majority of practical support but are frequently invisible within healthcare systems. The proposed approach could make carers more visible by helping professionals understand who is involved in supporting a patient and what role they play in maintaining wellbeing and independence.
Q: How will patient confidentiality and data protection be managed? A: Concerns were raised about privacy and the security of NHS data. Dr De Simoni explained that information governance, GDPR compliance, and data protection would be central to the project. Specialists in privacy and information governance would be involved to ensure that any information collected is handled safely, appropriately, and with proper consent.
Key Discussion: Why Are Carers Still Fighting the Same Battles?
A recurring theme throughout the meeting was the sense that many challenges identified today are the same challenges carers raised ten or twenty years ago.
Questions included:
Why are services still fragmented?
Why do carers continue to feel excluded?
Why are communication problems so persistent?
Why is trauma often overlooked?
Why do inequalities remain entrenched?
Participants reflected on whether the issue is primarily one of resources, leadership, service design, or culture.
Many agreed that meaningful change requires carers to remain actively involved in shaping policy and service delivery.
A carers support group recommended during discussion as a source of peer support and shared experience.
Final Reflections
The May 2026 Ethnic Mental Health Carers Forum highlighted both the challenges carers continue to face and the determination across the sector to improve outcomes.
From Mental Health Act reform and carers’ rights to innovative approaches such as Open Dialogue, the meeting demonstrated the importance of bringing together lived experience, research, policy, and practice.
Several speakers reminded attendees that change often begins with carers sharing their stories, participating in research, challenging poor practice, and helping shape future services.
The forum remains an important space where those voices can be heard.
By Matthew McKenzie – Triangle of Care Community Chair.
The meeting opened with a welcome to carers, professionals, and partner organisations, reinforcing the importance of the Community Group as a collaborative and inclusive space. The Chair highlighted the ongoing commitment to co-production, ensuring that lived experience remains central to all Triangle of Care development and decision-making.
The purpose of the meeting was outlined, with emphasis on shared learning, constructive challenge, and influencing national work. Members were reminded that discussions within the group directly inform improvements to Triangle of Care standards, guidance, and implementation across services.
2. Triangle of Care Update (with Q&A)
Mary Patel – Carers Trust
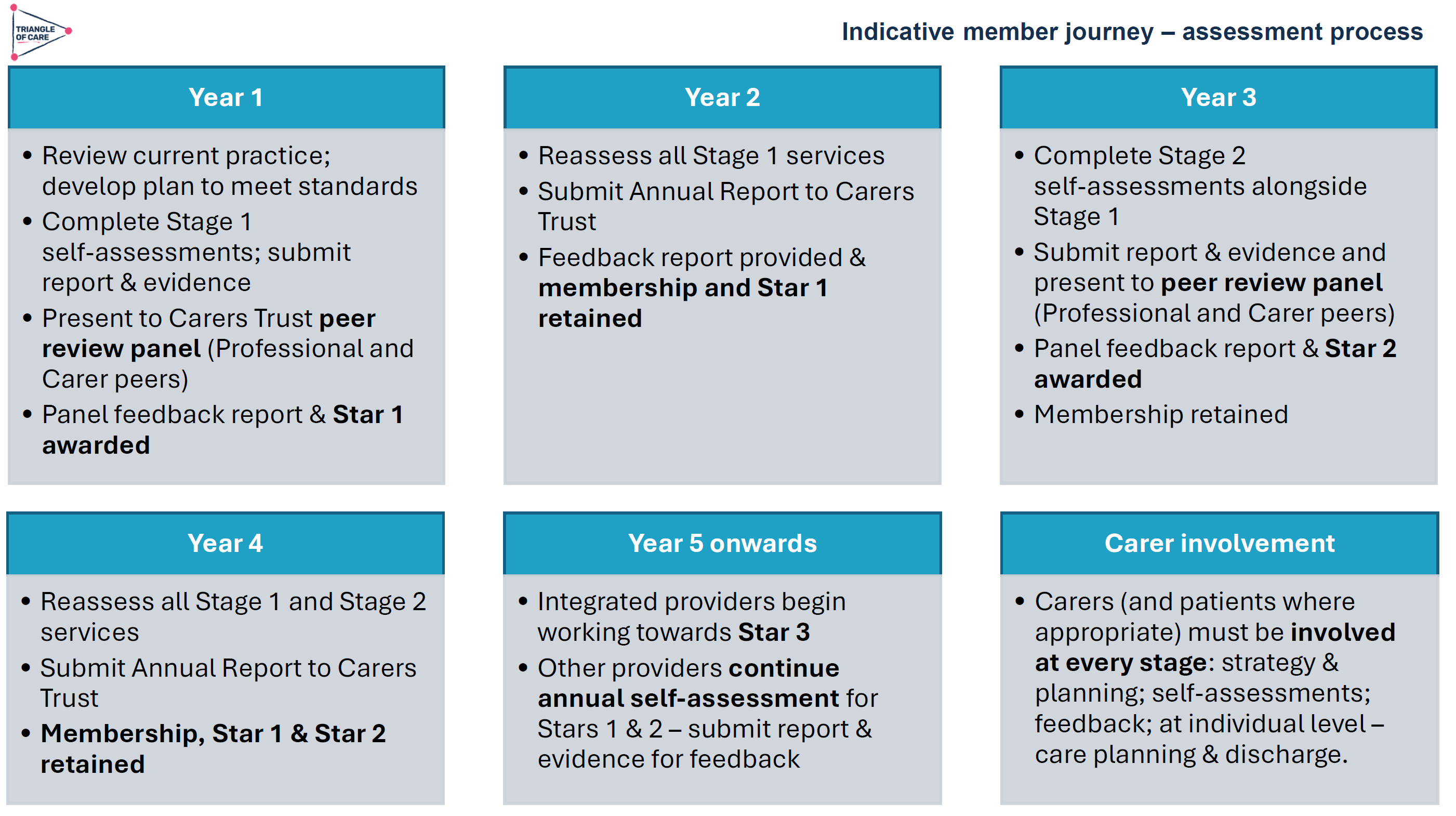
The Triangle of Care update focused on how the programme continues to evolve as a learning-led, improvement-focused framework rather than a compliance or inspection tool. Members were reminded that the Triangle of Care is designed to support services to reflect honestly on how well carers are recognised, involved, and supported, and to identify practical actions for improvement.
The update highlighted the growing maturity of the self-assessment and peer review process. Increasingly, organisations are using the framework not only to evidence good practice but to challenge themselves, learn from others, and embed carer partnership more consistently across teams and pathways.
Self-Assessment and Peer Review: What’s Working Well
The self-assessment process continues to be a key entry point for organisations engaging with the Triangle of Care. Where we were updated on how self-assessment encourages teams to pause and reflect on everyday practice, policies, and culture, rather than relying solely on written procedures. When combined with peer review, this reflection is strengthened by external challenge and lived-experience insight.
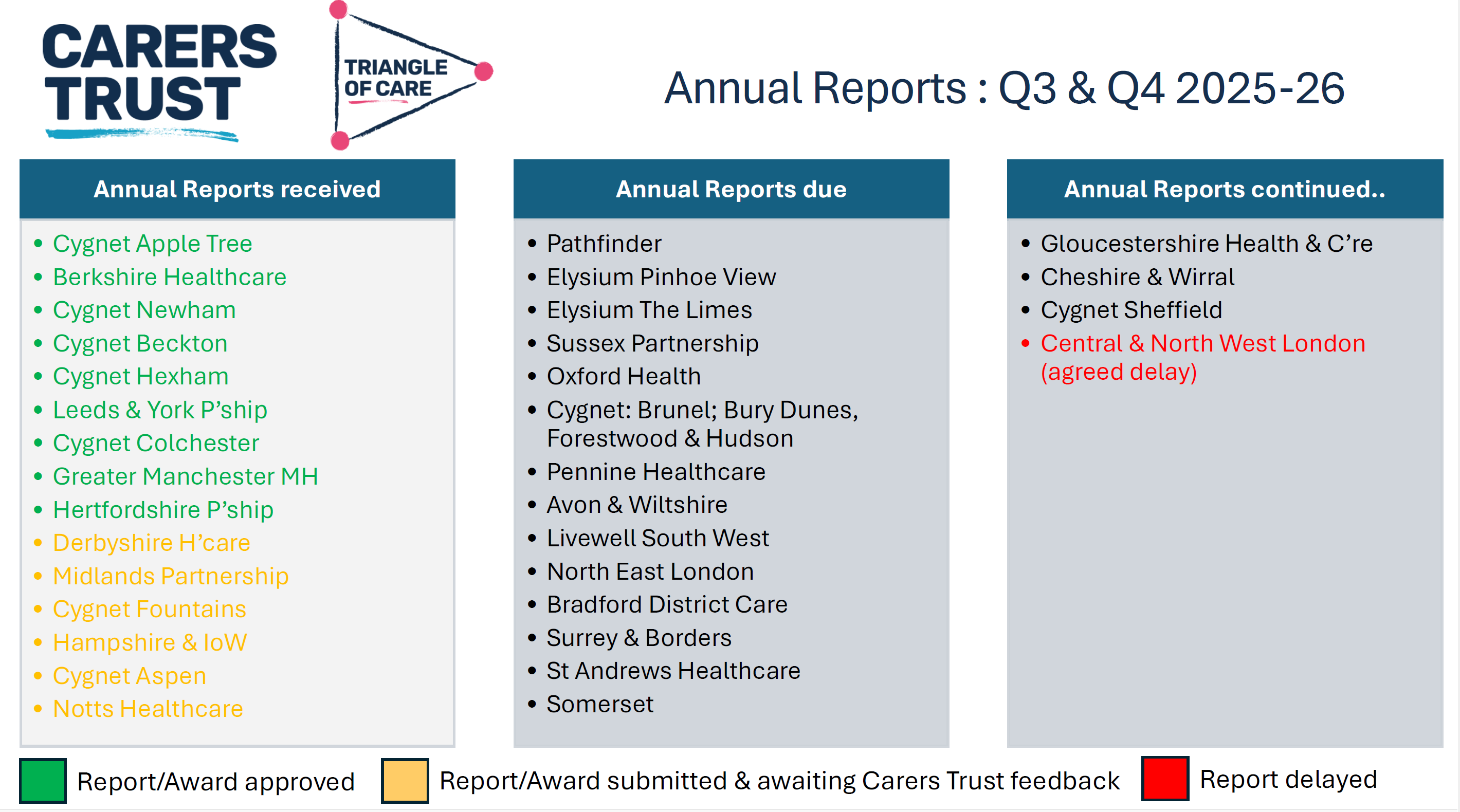
As part of the update, members were updated on emerging learning from Triangle of Care reports, including self-assessment submissions and peer review feedback. These reports were described as an important source of insight into how carer involvement is experienced on the ground, highlighting both areas of strong practice and recurring challenges across services
NOTE: These include reports going back 6 months, so not all NHS trusts listed
Peer review was described as most effective when organisations approach it with openness and curiosity. Lived-experience peer reviewers play a crucial role in asking different questions, highlighting blind spots, and grounding discussions in real-world carer experience.
A key discussion point was how to balance national consistency with local flexibility. Members acknowledged that while the Triangle of Care provides a shared framework and standards, services operate within different contexts, populations, and resource constraints.
Triangle of care and Patient Carer Race Equality Framework updates
The Triangle of Care and PCREF Phase 2 pilot will be launched in April 2026, to test co-produced specialist guidance to support integration of carers from racially marginalised communities into the Triangle of Care.
Alignment with Wider System Priorities
Members discussed how Triangle of Care activity aligns with broader system developments, including Mental Health Act reform, integrated care, and equality frameworks. There was strong agreement that Triangle of Care should not sit in isolation but be embedded within wider quality improvement, safeguarding, and workforce development agendas.
The need to visibly align Triangle of Care with the Patient and Carer Race Equality Framework was reiterated. Members emphasised that carers must be able to see how equality commitments translate into tangible actions within standards, training, and evidence.
Key points
Aligning Triangle of Care with Mental Health Act reform
Embedding within wider system and quality frameworks
Stronger visibility of equality and race equity
Carer Voice and Evidence of Impact
A recurring theme was the importance of demonstrating impact. Members discussed how services can better evidence carer involvement and experience beyond policies and training records. This includes qualitative feedback, lived-experience insight, and examples of how carer input has influenced service design and delivery.
Emerging Challenges and Areas for Development
The update also acknowledged ongoing challenges, including workforce pressures, digital transformation, and uneven awareness of the Triangle of Care across organisations. Members noted that carer involvement can become fragile during periods of change unless it is firmly embedded in systems and culture.
Summary: Where the Programme Is Heading
The Triangle of Care update concluded with a shared understanding that the programme is well-established but still evolving. The focus for the next phase is on deepening impact, strengthening alignment with equality and legislative change, and supporting services to move from intention to consistent, inclusive practice.
Key discussion points
Peer review as a developmental, learning-focused process
Balancing national consistency with local flexibility
Alignment with Mental Health Act reform and equality frameworks
Keeping carer voices central to assessment and review
3. Sharing Experiences as a Peer Reviewer
Carer involved with Avon & whitlshire
A carer presented from her involvement at Avon and Wiltshire Mental Health Partnership NHS Trust, where she is involved as a lived-experience peer reviewer contributing to Triangle of Care.
She shared reflections from her role as a lived-experience peer reviewer. She spoke about the importance of authenticity, trust, and transparency in the peer review process, and how lived experience strengthens both credibility and impact. Her contribution reinforced the value of co-production and highlighted how peer review can challenge assumptions, surface good practice, and promote more carer-inclusive cultures within organisations.
The discussion reinforced that organisational openness and leadership engagement are critical to turning peer review feedback into real change. Members reflected on how hearing directly from peer reviewers deepens understanding of the practical impact of policies on carers.
Q&A / Discussion
Members asked how organisations typically respond to lived-experience feedback.
The involved carer noted that openness and leadership support were key factors in whether reviews led to meaningful change.
Discussion reinforced the importance of preparing services for peer review so that carers feel genuinely welcomed and listened to.
4. Carer Contingency Planning – Presentation and Local Practice
Mary Patel Local example: Carly Driscoll – Bradford District Care
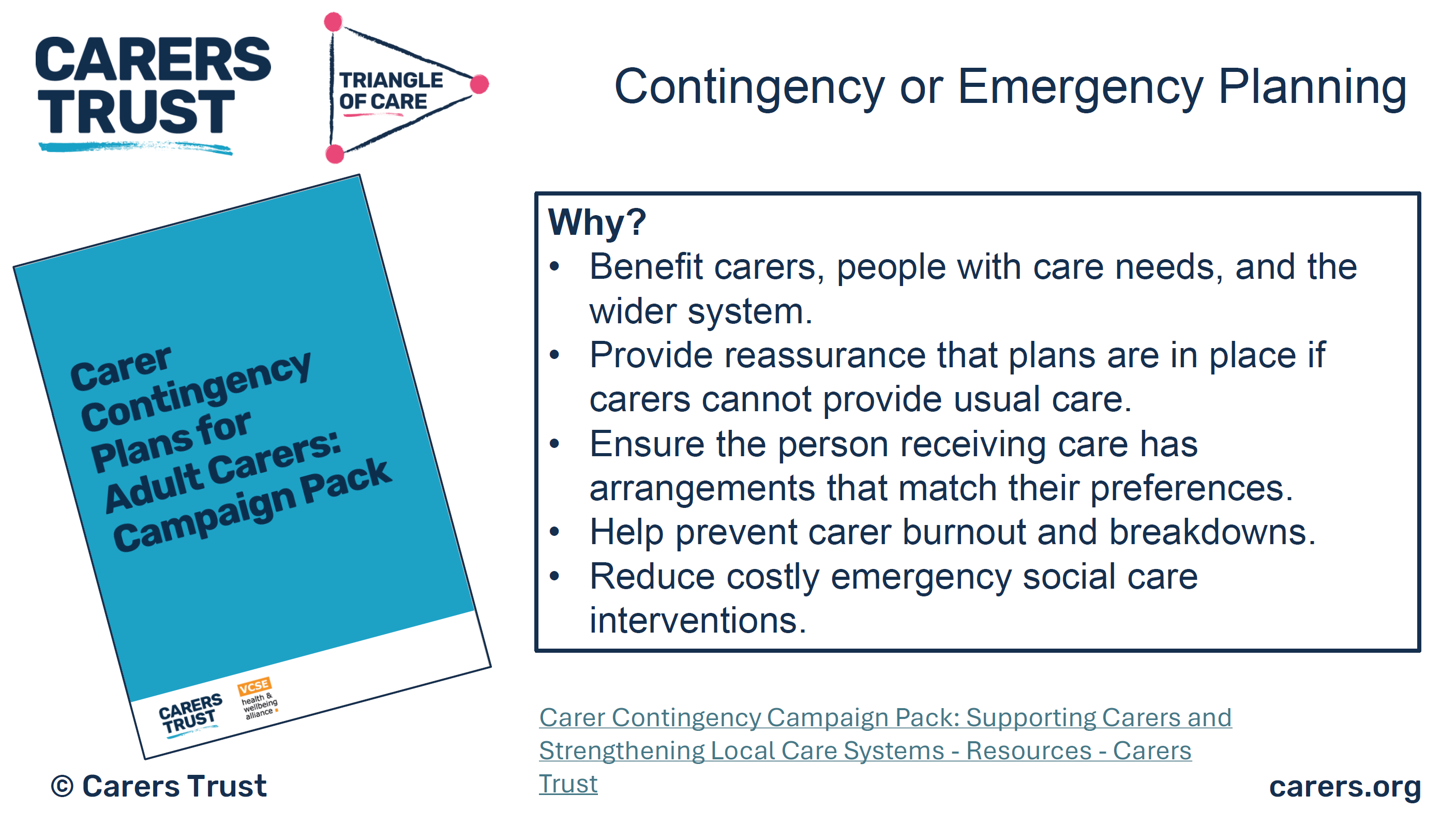
This session focused on carer contingency planning as a key element of carer support and crisis prevention. The presentation outlined why contingency planning is critical in reducing carer anxiety, preventing emergency admissions, and ensuring continuity of care when carers are unable to continue their role.
Carer Contingency Planning (CCP), as championed by Carers Trust, is designed to support carers by planning ahead for times when they might suddenly be unable to continue caring. This might include illness, emergencies, hospitalisation, or other crises. CCP shifts the focus from reactive support during crisis moments to proactive planning that reduces anxiety and prevents avoidable breakdowns in care.
Carers Trust emphasises that CCP is a conversational, personalised process where the carer’s expertise is central. Carers know the routines, preferences, and cues that matter for the person they care for; the goal of CCP is to capture that knowledge in a way that can be shared quickly and effectively with services, families, and emergency responders when needed.
A local practice example from Bradford District Care demonstrated how contingency planning can work in practice, highlighting practical tools, partnership working, and engagement with carers. Discussion explored the benefits of clear, accessible plans, while also acknowledging challenges around awareness, consistency, and uptake
The local practice example demonstrated how contingency planning can be embedded into routine work through partnership approaches and proactive engagement with carers. Members discussed the importance of introducing plans early and reviewing them regularly.
Key features of the Bradford approach
Routine integration: CCP discussions happen early, not just in crisis moments
Partnership working: Health, social care, and voluntary sector staff work in concert
Accessible documentation: Plans are shared in forms that carers can use and update
Support for carers: Carers are supported to lead the planning, not be passive recipients
Ongoing review: Plans are revisited as needs and circumstances evolve
Benefits seen locally
Carers report feeling more confident and less anxious
Greater clarity across professionals when carers are unavailable
Fewer last-minute, unplanned crises or service escalations
Better use of local support networks when official services are stretched
Q&A / Discussion
Questions focused on how contingency plans are introduced to carers and reviewed over time.
Members raised concerns about low awareness of contingency planning among carers not already engaged with services.
Discussion highlighted the need for flexibility, recognising that carers’ circumstances can change rapidly.
5. Carer Contingency Planning – System Perspective
Sara Lewis – SW London ICB
Sara Lewis’s session focused on Carer Contingency Planning (CCP) as a core, preventative element of carer support rather than a reactive or optional add-on. CCP is a structured way of planning for what should happen if a carer is suddenly unable to continue caring due to illness, crisis, exhaustion, or an emergency. At its heart, CCP is about reducing uncertainty and anxiety for carers while ensuring continuity and safety for the person they support.
Sara emphasised that effective CCP recognises carers as partners with expert knowledge of the person they care for. The process supports carers to articulate what matters most, what routines and support are essential, and who needs to be contacted in an emergency. When done well, CCP helps prevent avoidable crises, emergency admissions, and breakdowns in care by making plans visible, accessible, and shared across relevant services.
Accessibility was a major theme, particularly the risks of digital exclusion. While digital tools can be effective, members stressed the need for non-digital options, language support, and culturally appropriate approaches to ensure equity.
Key Takeaways from Sara Lewis’s Session
Carer Contingency Planning is preventative, not reactive
CCP is built on early, ongoing conversations with carers
Plans should reflect what matters to carers and the cared-for person
CCP must be accessible, inclusive, and culturally appropriate
Digital tools can help, but must not increase exclusion
Successful CCP requires shared ownership across services
When embedded well, CCP reduces crisis, anxiety, and system pressure
Q&A / Discussion
Members questioned how to balance digital innovation with the risk of digital exclusion.
Language barriers and accessibility for carers with different communication needs were highlighted.
Discussion emphasised that contingency planning must be embedded into standard care planning processes, not treated as optional or additional.
6. Looking Ahead: Priorities for the Community Group
The “Looking Ahead” discussion focused on how the Triangle of Care Community Group can continue to influence meaningful change for carers in an evolving policy and practice landscape. Members reflected on the increasing complexity of health and care systems and the importance of ensuring that carers are not left behind as reforms, digital transformation, and workforce pressures accelerate.
A strong theme throughout the discussion was visibility, making carer involvement, equality, and partnership explicit in practice, evidence, and outcomes. Participants emphasised that carers must not only be recognised in principle but experience consistent involvement and support in real-world settings. The group agreed that the next phase of work should strengthen both strategic influence and practical implementation.
Mental Health Act Reform and Carer Involvement
Members discussed the implications of upcoming Mental Health Act reform, particularly around carers’ rights, information-sharing, and involvement in decision-making. There was recognition that Triangle of Care principles provide a strong foundation for supporting services to meet new expectations, but that further work will be needed to translate legislation into everyday practice.
The group highlighted the risk that carers could be inconsistently involved if workforce understanding is weak or if systems focus narrowly on legal compliance. Proactive guidance, training, and examples of good practice were seen as essential to ensure carers are meaningfully included rather than consulted as an afterthought.
Equality, Race Equity, and Inclusion
A central priority looking ahead is ensuring that Triangle of Care activity visibly aligns with the Patient and Carer Race Equality Framework (PCREF). Members stressed that carers from racialised and marginalised communities often face additional barriers to involvement, including mistrust, cultural misunderstandings, and unequal access to support.
The group agreed that equality must be embedded into standards, peer review evidence, and training—not treated as a parallel or optional agenda. This includes capturing meaningful data, listening to diverse carer voices, and ensuring culturally responsive practice is clearly demonstrated.
Workforce Training and Education
Workforce development was identified as a critical lever for long-term change. Members highlighted the need to strengthen carer awareness training across all roles, particularly for staff new to mental health and social care settings. Without this foundation, carer involvement remains inconsistent and dependent on individual attitudes rather than organisational culture.
There was strong support for influencing pre-registration education, including universities and training providers, to embed carer awareness earlier. This was seen as an opportunity to normalise partnership with carers from the start of professional careers rather than trying to retrofit it later.
Key points
Strengthening carer awareness across the workforce
Embedding Triangle of Care principles early in training
Influencing universities and pre-registration pathways
Moving from individual goodwill to system-wide culture change
Digital, Data, and Accessibility
Digital transformation featured prominently in the discussion, with members acknowledging both its potential and its risks. While improved data systems and digital tools can support information-sharing and coordination, there was concern that carers without digital access or confidence may be excluded.
Participants emphasised that digital solutions must be designed inclusively, with non-digital alternatives always available. Data collection should support understanding of carer experience and inequality, not become a barrier to support.
Key points
Digital tools should support, not replace, relationships
Risk of digital exclusion for some carers
Importance of non-digital alternatives
Using data to improve equity, not reinforce gaps
Young Carers and Marginalised Groups
Supporting young carers and carers from marginalised communities was highlighted as a continuing priority. Members noted that these groups are often under-identified and less likely to be involved in care planning or decision-making, despite carrying significant caring responsibilities.
The group agreed that future work should focus on visibility, early identification, and tailored approaches that recognise the specific needs and challenges faced by these carers. Partnership with education, community, and voluntary sector organisations was seen as essential.
Key points
Improving identification of young carers
Addressing barriers faced by marginalised carers
Tailored, age-appropriate and culturally sensitive support
Stronger partnership working beyond health services
Collective Commitment Moving Forward
The discussion concluded with a shared commitment to using the Community Group as a platform for influence, learning, and accountability. Members recognised the value of continuing to share practical examples alongside strategic discussion, ensuring that Triangle of Care principles are translated into everyday practice.
Looking ahead, the group aims to remain proactive, inclusive, and responsive—supporting services to recognise carers as equal partners and ensuring that no carer is left unseen or unsupported as systems evolve.
Key discussion points
Preparing for Mental Health Act reform
Embedding the Patient and Carer Race Equality Framework
Improving workforce training and education pathways
Supporting young carers and marginalised communities
Improving data and digital systems without exclusion
As Chair I thanked contributors and reaffirmed the importance of continued collaboration to ensure carers are recognised as equal partners in care, with Triangle of Care principles translated into meaningful practice across services.
For those interested to hear more about triangle of care, see details below