If you weren’t able to join our June South London Mental Health Carers Group meeting, here’s a summary of the main discussions and updates. As always, the meeting brought together unpaid carers from across Lambeth, Lewisham, Southwark and Croydon to share experiences, raise concerns and keep each other informed about developments affecting mental health carers.
Why these meetings matter
One of the strongest themes throughout the meeting was the importance of carers staying connected. Many carers cannot attend every committee or involvement meeting due to their caring responsibilities, work or other commitments. By sharing updates, we can help ensure everyone remains informed about changes that may affect them and the people they support.
Several carers commented that services sometimes feel like they are “reinventing the wheel”, with the same issues being raised repeatedly. While progress can be slow, continuing to speak up and share experiences remains essential.
Updates from the Maudsley Family and Carers Committee
Carers who attended the latest South London and Maudsley (SLAM) Family and Carers Committee shared several important developments.
Review of the Involvement Register
SLAM is reviewing its Involvement Register over the coming months. Working groups will look at areas including:
Outcomes
How involvement is delivered
Governance and policy
Carers interested in influencing how services engage with families are encouraged to consider joining the register. Participation is flexible, allowing carers to contribute when they are able.
Triangle of Care
The Triangle of Care continues to be a significant focus, particularly around how carers are identified, involved and supported during someone’s mental health care.
Discussions also covered how Trusts monitor their progress and how carers’ details are recorded to ensure families receive appropriate information and support.
Information for carers
Work is continuing to improve the information provided to carers. Rather than relying on a single handbook that can quickly become outdated, there are plans to develop more flexible information resources that can be updated more easily and provided when carers actually need them.
Mental Health Act reforms
A significant part of the meeting focused on the recent changes to the Mental Health Act and what they could mean for unpaid carers.
Key topics included:
Greater emphasis on patient choice and involvement.
The introduction of the Nominated Person, replacing the traditional “Nearest Relative” in many situations.
The importance of Advance Choice Documents, allowing people to record their wishes while they are well.
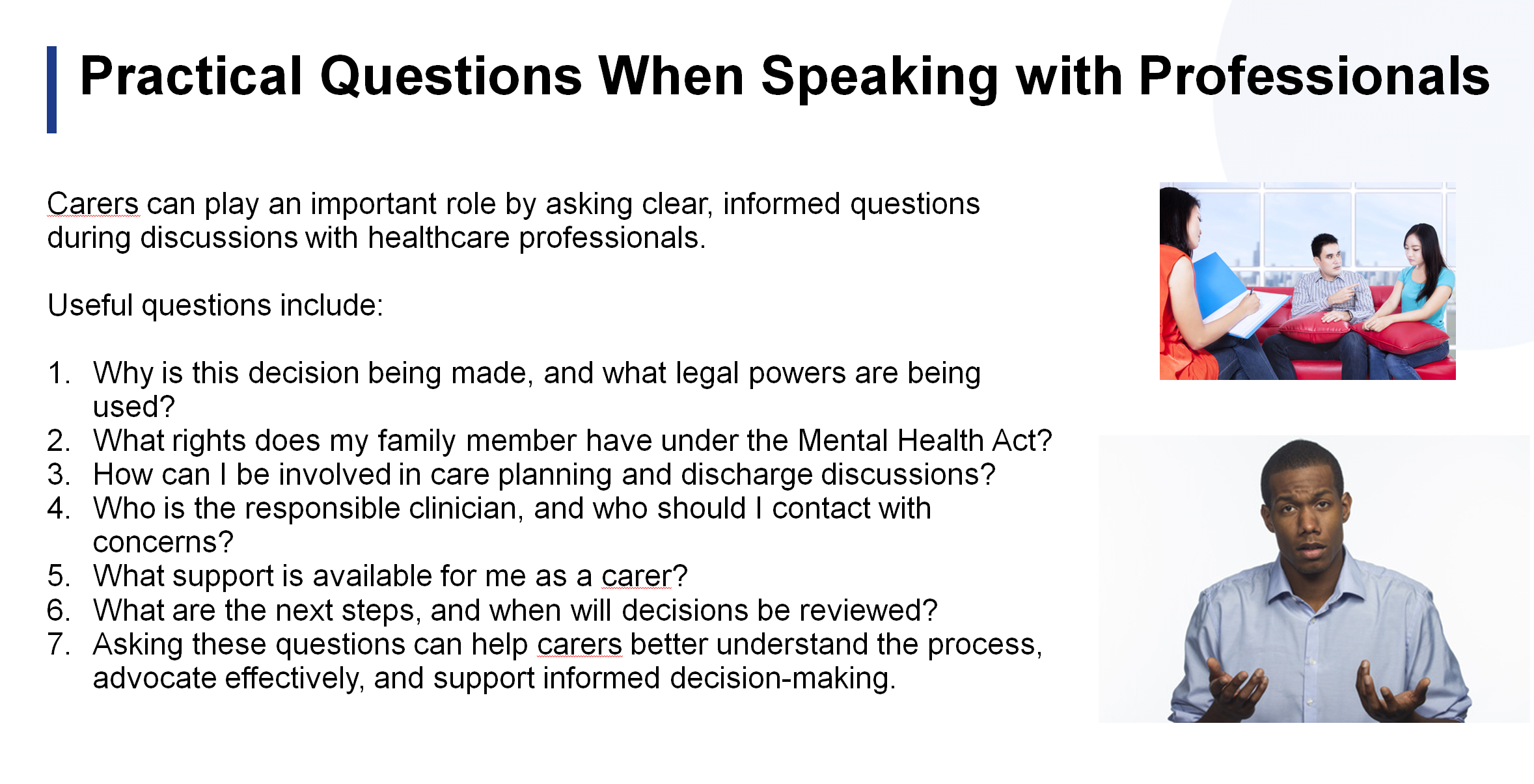
The need for carers to understand their legal rights and ask questions during admissions, treatment planning and discharge.
Carers discussed both the opportunities and concerns arising from these changes, particularly where someone may lose insight during periods of illness. There was broad agreement that carers need clear information about how the reforms will be implemented locally and how families will continue to be involved.
Advocacy and complaints
Members shared experiences of trying to access advocacy services and navigate complaints processes.
Concerns included:
Limited access to independent mental health advocacy in some boroughs.
Unclear complaints pathways.
The need for carers to be listened to, even when confidential information cannot be shared with them.
The importance of raising concerns through appropriate safeguarding and governance routes where necessary.
Several carers also shared positive experiences where persistence had led to improvements in care.
Local updates from across South London
One of the strengths of the South London Mental Health Carers Group is the opportunity for carers from different boroughs to share what is happening locally. While each area faces its own challenges, many of the issues raised were common across South London.
Lambeth
Carers discussed the continuing work of the Lambeth Living Well Collaborative, which brings together carers, service users, voluntary organisations and professionals to improve local mental health services. Members were reminded that carers are welcome to attend collaborative meetings and contribute to discussions about service improvements.
The conversation also recognised the wider pressures affecting carers beyond mental health services. Rising living costs, reductions in council tax support for many working-age residents receiving benefits, and the increasing financial pressures on families continue to affect carers’ wellbeing. These wider social issues inevitably have an impact on people’s ability to sustain their caring role.
Lewisham
Carers provided an update on Lewisham’s Community Mental Health Transformation programme. While work continues to redesign community services, concerns remain about what happens when someone is discharged from specialist mental health services back to primary care.
Several carers highlighted unanswered questions around:
How GPs will be supported to manage people with ongoing severe mental health needs.
What support carers can expect once specialist services are no longer involved.
Whether communication between secondary mental health services and GP practices is sufficiently robust.
These are important questions that carers hope local services will continue to address as transformation plans progress.
Croydon and Lewisham carer information
Members also heard that new information resources for carers are being developed in Croydon and Lewisham. Rather than relying on lengthy booklets, services are creating a series of practical information sheets covering different aspects of mental health care. This approach should allow information to be updated more regularly and provided when carers need it most.
Carers welcomed this change, noting that people often need specific information at different stages of their caring journey rather than receiving a large handbook all at once.
The important role of GP practices
An interesting discussion focused on the role of GP practices in supporting unpaid carers.
Members recognised that experiences vary considerably between surgeries. Some GP practices have developed strong support for carers, while others still have some way to go.
One positive example shared was Wells Park Practice, where carers have become actively involved in developing support, including helping to establish a regular carers’ coffee morning. This demonstrates what can be achieved when GP practices actively engage with carers and recognise the valuable role they play.
The meeting reinforced several practical messages for carers:
Make sure your GP practice knows that you are an unpaid carer and ask to be recorded on their carers register.
Ask what support your surgery offers to carers, including health checks, referrals or local support groups.
If your current practice offers limited support for carers, it may be worth exploring what neighbouring GP practices provide, particularly if they have developed a stronger carers programme.
As community mental health services increasingly work alongside primary care, ensuring that GP practices recognise and support unpaid carers is becoming more important than ever.
Learning from each other
Perhaps the most valuable part of the local updates was hearing how carers are finding solutions in different boroughs. Good practice in one area can often inspire improvements elsewhere.
Whether discussing carers’ information, community transformation, GP engagement or involvement opportunities, the message was clear: carers’ experiences are a vital source of learning, and sharing those experiences helps improve services across South London as a whole.
Looking ahead
One of the biggest messages from the meeting was that carers have valuable lived experience that services need to hear. Whether through local carers’ centres, involvement registers, Trust committees or community groups, every contribution helps shape future services.
If you are interested in becoming more involved but can only contribute occasionally, don’t let that put you off. Many opportunities allow carers to participate as much or as little as their circumstances allow.
Thank you to everyone who attended and contributed so openly. Your experiences continue to help improve understanding and influence services across South London.
We look forward to welcoming both new and returning carers to our next meeting.
Written by Matthew McKenzie, Speaker, Carer, Campaigner and Poet
As part of Carers Week 2026, I had the privilege of travelling to East Dean in East Sussex to speak at the East Sussex Carers Voices – Celebrating Carers Week Event, organised by Care for the Carers. The event brought together unpaid carers, carers’ organisations, NHS representatives, local authority leaders, health professionals, community groups and carers from across East Sussex to discuss the realities of caring and identify ways to improve support for unpaid carers.
The event was hosted by Dr Neil Churchill, Chair of Care for the Carers, who guided the day’s discussions and emphasised the vital role carers play in society. Throughout the day, carers shared their personal stories, experiences and recommendations directly with decision-makers and service providers.
This blog post provides an overview of the key themes, speakers and discussions for those who were unable to attend.
Opening Remarks – Dr Neil Churchill
Dr Neil Churchill opened the event by welcoming attendees and recognising the significant contribution unpaid carers make to families, communities and public services.
He highlighted several key challenges currently facing carers:
• Rising financial pressures and cost-of-living concerns. • The growing number of carers leaving employment due to caring responsibilities. • Increased risks of poor physical and mental health among carers. • Social isolation and loneliness experienced by many carers. • Growing concerns around carer burnout.
Dr Churchill stressed that the country depends heavily on unpaid carers and that health and social care systems would struggle to function without them. He also spoke about the importance of moving towards a model where carers are treated as equal partners in care rather than simply being expected to cope alone.
A key message from his introduction was that carers should not be left to navigate fragmented services by themselves. Instead, health, social care and voluntary sector organisations must work together more effectively to recognise, support and value carers.
Carer Stories and Lived Experience
One of the most powerful aspects of the event was hearing directly from carers themselves.
Miles Bing – Caring Through Dementia
The first speaker was Miles Bing, author of “Deadheaded: An Alzheimer’s Memoir by Mother and Son”.
Miles shared his family’s experience of supporting both of his parents through Alzheimer’s disease. His presentation explored the emotional impact of caring at a distance, the guilt often experienced by family members who live far away, and the difficulties of coordinating support across multiple services.
He spoke about:
• The long-term impact of dementia on families. • The challenges of accessing services in rural areas. • The lack of coordination between health and social care systems. • The practical and emotional burden placed on carers.
Many attendees identified strongly with his comments regarding the need for carers to act as coordinators between multiple organisations that often fail to communicate effectively with one another.
Young Carers – Julia and Elsie
The audience then heard from young carers Julia and Elsie, whose presentations left a lasting impression on everyone in the room.
Both spoke honestly about growing up while caring for family members with complex needs. They described responsibilities that included supporting parents during health crises, helping siblings with disabilities and managing situations involving emergency services.
Their stories demonstrated:
• The hidden nature of young caring responsibilities. • The emotional impact caring can have on children and young people. • The importance of early intervention and support. • The value of dedicated young carers services.
Perhaps most importantly, they highlighted that while caring can build resilience, no child should have to face these responsibilities without support.
The standing ovation they received reflected the courage and honesty with which they shared their experiences.
Round Table Discussions
Following the morning speakers, attendees participated in facilitated round table discussions.
These conversations focused on:
• The biggest issues facing carers over the next six months. • Practical actions that could help carers in their caring role. • Barriers to accessing support. • Positive examples of support that should be expanded.
Several common themes emerged from these discussions:
Earlier Identification
Many carers reported not being recognised as carers until they had reached crisis point. Participants called for earlier identification within GP surgeries, hospitals and community services.
Access to Information
Attendees highlighted how difficult it can be to find accurate and timely information about available support.
Financial Pressures
Many carers discussed the financial impact of caring, including reduced employment opportunities and increasing household costs.
Mental Health and Wellbeing
Carers spoke about the emotional strain of caring and the importance of counselling, respite and peer support services.
Speaker sessions resumes
Diverse Communities and Caring
A particularly thought-provoking presentation was delivered by Manal Ahmed, who supports carers from ethnically diverse and refugee communities.
She discussed additional challenges experienced by carers from minority communities, including:
• Language barriers. • Cultural differences. • Social isolation. • Displacement trauma. • Immigration-related issues. • Financial and emotional dependency.
Manal explained that many carers experience multiple layers of disadvantage and that support services must be culturally aware and accessible to everyone.
She also highlighted positive examples of community-building activities that help carers connect with one another and reduce isolation.
Her presentation reinforced the importance of ensuring that no carer is excluded from support because of their background, language or circumstances.
My Presentation – A Carer’s Journey
I was invited to speak about my own experiences as a young carer and later as an adult carer supporting family members with autism and serious mental illness.
One of the key messages I shared was that many carers do not initially recognise themselves as carers. Like many people, I simply viewed what I was doing as helping my family.
However, over time I found myself:
• Coordinating care. • Supporting hospital admissions and discharges. • Managing appointments. • Advocating with professionals. • Navigating complex systems. • Supporting multiple family members simultaneously.
I spoke about how difficult it can be when carers are not listened to or involved in important decisions.
I also highlighted the importance of recognising carers as equal partners in care and ensuring that professionals understand the expertise carers develop through lived experience.
One of the central themes of my presentation was carers’ rights.
I encouraged carers to:
• Identify themselves as carers. • Seek support from local carers organisations. • Request carers assessments. • Learn about their rights. • Participate in co-production and service improvement. • Share their experiences to help reduce stigma.
To conclude, I performed my poem “It’s My Right”, which focuses on the rights every carer should expect to receive, including recognition, respect, involvement, information and support.
Afternoon Reflections and Future Priorities
The afternoon session included reflections from senior leaders from Care for the Carers, East Sussex County Council and NHS Sussex.
Discussions focused on:
• Improving identification of carers. • Supporting carers before crises occur. • Encouraging carers to access support services. • Learning from positive experiences of care. • Strengthening partnerships between carers and professionals.
Representatives acknowledged the crucial role carers play and listened to feedback gathered throughout the day.
Many carers expressed concerns about navigating systems that can often feel complicated and difficult to access. There was broad agreement that services should be simpler, more joined-up and more responsive to carers’ needs.
Key Messages from the Day
Several important messages emerged consistently throughout the event:
Carers Need Recognition
Many carers remain hidden and unidentified. Earlier recognition can lead to earlier support.
Carers Need Practical Support
Information, respite, emotional support and financial advice remain essential.
Carers Must Be Involved
Carers are experts in the lives of the people they support and should be treated as partners in care.
Young Carers Need Protection
Children and young people with caring responsibilities require dedicated support and opportunities to thrive.
Communities Matter
Strong local networks can help reduce isolation and improve wellbeing.
Prevention Is Better Than Crisis Management
Supporting carers early can prevent breakdowns in caring arrangements and reduce pressure on services.
Conclusion
The East Sussex Carers Voices Event was an excellent example of what can happen when carers, professionals and decision-makers come together to listen, learn and work collaboratively.
Throughout the day, carers shared powerful stories of resilience, commitment and compassion. They also spoke honestly about the challenges they face and the changes they want to see. I also recognised Agi who does lots of work raising carer awareness in Sussex, she recently spoke at my national ethnic mental health carers forum. So it was great to see her there.
Dr Neil Churchill’s leadership as host helped create an environment where carers felt able to speak openly and where decision-makers could hear directly from those with lived experience.
As Carers Week 2026 comes to a close, the challenge now is to turn these conversations into meaningful action. Carers should not have to struggle to be recognised, supported or heard.
The event demonstrated that when carers’ voices are placed at the centre of discussions, better solutions can emerge for everyone.
Thank you to Care for the Carers, all speakers, volunteers, professionals and carers who contributed to such a valuable and inspiring day.
For Carers Week 2026, it takes place from 8–14 June and shines a spotlight on the millions of unpaid carers who provide essential care and support to family members, friends and loved ones throughout the UK.
This year’s theme, Building Carer Friendly Communities, highlights the need for workplaces, healthcare services, schools, local authorities and communities to better recognise and support unpaid carers.
Despite contributing billions of pounds worth of care each year, many unpaid carers continue to face challenges including financial hardship, social isolation, poor mental health and difficulties accessing support. So Carers Week aims to raise awareness of these issues while encouraging practical action to create a society where carers are valued, respected and included.
As a carer activist and founder of my site A Caring Mind, I am sure that creating carer-friendly communities starts with understanding the realities of caring. Whether you are caring for an ageing parent, a disabled child, a partner with a long-term condition or someone experiencing mental ill health, carers play a vital role in keeping families and communities together.
However, there are still many people do not identify themselves as carers and therefore miss out on important support, benefits and services. Carers Week 2026 provides an opportunity for individuals, organisations and policymakers to listen to carers’ experiences, champion carers’ rights and improve access to support for unpaid carers across the UK.
Watch my Carers Week 2026 video below to learn more about the campaign, this year’s theme and how you can get involved in supporting unpaid carers. Please share the video to help raise awareness and encourage more people to recognise the invaluable contribution that carers make every single day.
Together, we can build stronger, more inclusive and more carer-friendly communities
Blog by Ethnic Mental Health Carer forum Chair – Matthew McKenzie
The May 2026 Ethnic Mental Health Carers Forum brought together carers, researchers, clinicians, community leaders, and representatives from mental health organisations across England. Although attendance was smaller than usual, the discussion was rich, honest, and highly informative, covering Mental Health Act reform, carers’ experiences, service inequalities, innovative approaches to care, and new research opportunities.
For those who were unable to attend, this blog provides a comprehensive overview of the meeting, including key presentations, audience questions, responses from speakers, and useful resources shared during the session.
Opening Remarks
As the chair, I welcomed attendees and outlined the agenda. The meeting focused on following:
Mental Health Act research and reform
Carers’ experiences supporting loved ones through detention
Findings from a major East Sussex carers research project
Resources for carers under the Mental Health Act
Electronic Health Records and future developments
Wider discussions on racial trauma, inequalities, and service improvement
The meeting also provided opportunities for networking, sharing lived experiences, and highlighting innovative projects happening across the country.
Research Study: Supporting a Loved One Through Mental Health Detention
Dr Maeve Conneely from University College London opened the meeting with a presentation on a new research study exploring the experiences of people who have been assessed or detained under the Mental Health Act, as well as the experiences of family members and carers who supported them through that process. The study has been commissioned as part of the wider programme of Mental Health Act reform and aims to understand how the current “Nearest Relative” provisions operate in practice before changes are introduced under the new legislation.
Dr Conneely explained that researchers are particularly interested in hearing from carers who were involved in supporting a loved one but who were not formally recognised as the “Nearest Relative” under the existing legal framework. She highlighted that these experiences are especially important because they can reveal where carers have been excluded from decision-making, denied access to information, or prevented from contributing to assessments despite playing a significant role in supporting the individual concerned. The study is open to anyone aged 16 or over who has direct experience of Mental Health Act assessments, detentions, Community Treatment Orders, holding powers, or related interventions, whether as a patient or as a supporter.
The research is linked to ongoing reforms of the Mental Health Act and seeks to understand how the “Nearest Relative” provisions currently operate before changes are implemented.
Who Can Take Part?
The study is looking for:
People who have been detained under the Mental Health Act
Family members and carers who supported someone during detention or assessment
Individuals who should have been involved as a nearest relative but were not
Anyone aged 16 or over with relevant experience
Interviews are conducted online and participants receive a £30 shopping voucher as a thank-you for their time.
Key Question from Participants
Q: Does the study include situations where someone should have been involved but wasn’t?
Response: Yes. Researchers are particularly interested in understanding experiences where carers or family members were excluded from decision-making processes despite playing a significant caring role.
Another Important Question
Q: Do carers need permission from the person who was detained before participating?
Response: No. Carers are sharing their own experiences and therefore only need to provide their own consent.
Discussion Themes
Participants highlighted:
Long-standing inequalities affecting Black communities under the Mental Health Act.
The overuse of psychiatric labels without sufficient exploration of trauma.
The need to understand why some individuals receive significantly different experiences of care, including access to private mental health facilities.
Concerns about trust in mental health services and the lasting impact of poor experiences across generations.
Several carers committed to taking part in the study to ensure lived experience informs future policy.
East Sussex Carers Research Project: What Carers Told Us
Age Angiolini presented findings from a year-long carers-led research project examining the experiences of family carers supporting people with serious mental illness across East Sussex. The study was developed in response to repeated concerns raised by carers at local support meetings and sought to capture their experiences of interacting with mental health services provided by the Sussex Partnership Foundation Trust (SPFT).
Although the research received 71 responses, representing only a proportion of the carers population in the region, the findings revealed a striking consistency in the challenges carers face. The survey explored themes including carers’ involvement in care planning, communication with services, consent and confidentiality, quality of care, crisis support, and priorities for improvement. Among the most significant findings were that 72% of carers reported being only sometimes involved or not involved at all in their loved one’s care, 73% felt services relied too heavily on carers, and 72% said they regularly had to advocate to secure appropriate support. The research concluded that many carers feel undervalued, excluded from decision-making, and left carrying significant responsibilities without adequate recognition or support.
The study gathered responses from carers supporting people with:
Schizophrenia
Bipolar disorder
ADHD
Autism
Complex neurodiverse conditions
Although the sample size was relatively modest, the findings revealed significant and consistent concerns.
Key Findings from the report
Carers Feel Excluded
72% reported being only sometimes involved or not involved at all.
73% felt services relied too heavily on carers.
72% said they had to advocate strongly to secure appropriate care.
Communication Failures
Participants reported poor communication between:
Mental health services
Assessment teams
Social services
Mental health liaison teams
Many carers described communications as inconsistent, unclear, and difficult to navigate.
Consent and Confidentiality
A recurring concern was that confidentiality procedures are often applied rigidly, preventing carers from sharing vital information during crises.
Carers argued that this can actively undermine effective care.
Quality of Care Concerns
The research found:
90% reported insufficient care.
Significant concerns around continuity of care.
A strong desire for dedicated care coordinators.
Widespread frustration with crisis services.
Crisis Support is Not Working
Many carers reported that:
NHS 111 is often inadequate for mental health crises.
A&E is frequently unsuitable for people experiencing mental distress.
Services remain reactive rather than preventative.
Calls for Change
Recommendations included:
Better crisis pathways
Improved coordination between services
More trauma-informed approaches
Greater therapeutic support
Increased family involvement
Better support for neurodiverse individuals
The presentation sparked considerable discussion, with many attendees noting that the findings reflected experiences they had encountered for years.
Carers Speak Out: Frustration, Trauma and the Need for Change
One of the most powerful aspects of the meeting was hearing directly from carers.
Several participants reflected on decades of involvement with mental health services and expressed concern that despite repeated reviews, consultations, and reforms, many of the same issues continue to persist.
Common themes included:
Institutional racism
Poor communication
Exclusion of carers
Over-medicalisation
Lack of trauma-informed care
Inadequate support during crises
A number of attendees emphasised that families often become de facto care coordinators, managing appointments, services, medications, and crises while receiving little support themselves.
One participant observed:
“They plan, medicate and treat. We care. Our worlds don’t meet.”
Others highlighted the impact of racial trauma and the way mental health services can fail to recognise the cultural context of distress.
Open Dialogue: A Different Way Forward?
Ren Reins introduced the concept of Open Dialogue, an internationally recognised approach to mental health care that focuses on relationships, networks, and collaborative conversations.
Open Dialogue aims to:
Bring families and professionals together
Reduce fragmentation between services
Focus on lived experience
Build trust
Improve recovery outcomes
Ren explained that major NHS-funded trials are underway and encouraged carers to learn more about the approach.
The discussion generated significant interest, particularly from attendees looking for alternatives to traditional medical models of care.
Nearest Relative Resources Project
Professor Judy Laing from the University of Bristol provided an update on an innovative project designed to support family members and carers who hold, or may hold, responsibilities under the Mental Health Act’s “Nearest Relative” provisions. Drawing on previous research with carers and mental health professionals, Professor Laing explained that many family members who find themselves in the Nearest Relative role often receive little information, guidance, or emotional support despite carrying significant legal responsibilities. In response, her team secured funding to develop a free, co-produced online resource that helps carers understand their rights, responsibilities, and options when supporting a loved one through mental health assessment, detention, and treatment.
Developed in partnership with carers, family members, mental health professionals, and organisations including Mind, Rethink Mental Illness, and Carers Trust, the website provides practical information, downloadable tools, guidance for conversations with professionals, and resources to help carers look after their own wellbeing. Professor Laing stressed that the project has been shaped directly by the experiences of those who have undertaken the role themselves, ensuring that the guidance reflects the realities and challenges carers face in practice rather than simply explaining legal processes.
The project emerged from research identifying significant gaps in information and support for people carrying out the “Nearest Relative” role.
What Has Been Developed?
The project has created a free online resource containing:
Information about legal rights
Guidance on conversations with professionals
Practical tools for meetings
Support for carers’ wellbeing
Resources explaining upcoming legal changes
The materials have been co-produced with carers and family members.
Questions Raised
How are diverse communities included?
Participants asked how the project ensures equity and accessibility.
Professor Laing explained that:
People from ethnic minority backgrounds have contributed to development.
Resources are being improved to increase accessibility.
Additional funding is supporting work around inclusion and accessibility.
Translation and alternative formats are being explored.
How is the project promoted?
Discussion focused on ensuring communities are aware of available support rather than resources existing only online.
Professor Laing outlined efforts involving:
Mind
Carers Trust
Mental health services
Local media
Carer forums
How will the new Nominated Person role protect carers who have traditionally been involved in supporting a loved one?
Several participants expressed concern that replacing the Nearest Relative role could unintentionally weaken the involvement of family members who have historically provided substantial support during periods of mental ill-health. Questions were raised about situations where a person may choose someone other than their primary carer to act as their Nominated Person, potentially reducing carers’ ability to access information or participate in key decisions. Professor Laing acknowledged that these concerns have been raised by many carers and explained that the practical details of how the new system will operate are still being developed. She stressed the importance of carers contributing their experiences to ensure that future guidance recognises the valuable role families often play in supporting recovery and maintaining continuity of care.
What support is available when professionals fail to recognise or understand carers’ legal rights?
Attendees also discussed the reality that many mental health professionals are not always familiar with the legal powers and rights associated with the Nearest Relative role. Participants described situations where carers were excluded from discussions, not informed of important decisions, or felt unable to challenge professional opinions because they lacked confidence in their understanding of the law. In response, Professor Laing highlighted that one of the main objectives of the Bristol resources project is to bridge this knowledge gap by providing practical tools, suggested questions, and clear explanations of carers’ rights. She noted that the project is also developing resources aimed at professionals themselves, with the goal of increasing awareness and ensuring that carers’ legal rights are better understood and respected across mental health services.
Attendees welcomed the commitment to increasing visibility.
Electronic Health Records and Future Developments
Dr Anna De Simoni, an Academic GP and Associate Professor of Primary Care at Queen Mary University of London, presented an early-stage research proposal focused on how electronic health records could be used to better understand and map the social support networks surrounding people living with multiple long-term health conditions.
Dr De Simoni sought direct feedback from carers to help shape the project before a formal funding application is submitted. She explained that while healthcare professionals can usually identify a patient’s next of kin and household members through existing GP records, they often have very limited understanding of the wider support networks that play a vital role in a person’s wellbeing.
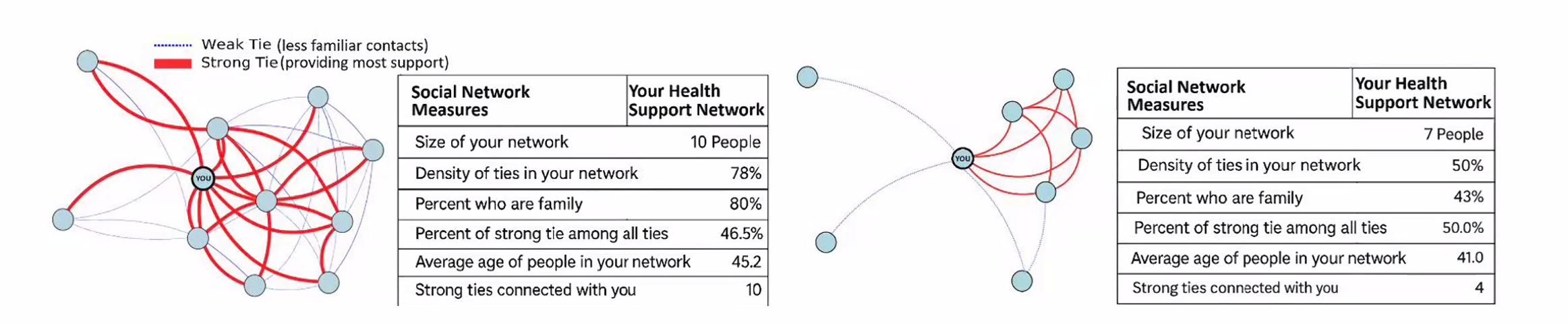
These networks may include family members, neighbours, friends, faith groups, community organisations, carers, and others who provide practical and emotional support. The research aims to explore whether technology and electronic health records can help healthcare professionals better recognise these support systems and use that information to improve care planning, reduce unnecessary hospital admissions, and enhance quality of life for people living with complex health conditions.
The discussion generated considerable interest, particularly regarding:
Information sharing
Integration across services
Support for carers
Data protection concerns
Improving continuity of care
Several participants expressed enthusiasm about the potential benefits while also raising questions regarding privacy and access to NHS information.
Questions and Answers from Dr Anna De Simoni’s Presentation
Q: What problem is this research trying to solve? A: Dr De Simoni explained that healthcare professionals often know very little about the wider support network surrounding a patient. While medical records may identify a next of kin or people living in the same household, they rarely capture the full picture of who is actually providing practical, emotional, or day-to-day support. The project aims to better understand these social networks and use that information to improve care planning and patient outcomes.
Q: Who is the research aimed at? A: The initial focus is on people living with multiple long-term health conditions, including illnesses such as COPD and other complex health needs e.g mental health. The project seeks to understand how stronger recognition of support networks could improve quality of life, reduce hospital admissions, and support people to remain independent for longer.
Q: How would patients contribute information about their support network? A: The proposal includes the use of a Universal Care Plan through the NHS App. Patients would be able to enter information themselves about what matters to them, who supports them, how they prefer to be treated, and what should happen if their health deteriorates. This information could then be viewed and updated by relevant healthcare professionals.
Q: What role could carers play within the proposed system? A: Participants highlighted that carers often provide the majority of practical support but are frequently invisible within healthcare systems. The proposed approach could make carers more visible by helping professionals understand who is involved in supporting a patient and what role they play in maintaining wellbeing and independence.
Q: How will patient confidentiality and data protection be managed? A: Concerns were raised about privacy and the security of NHS data. Dr De Simoni explained that information governance, GDPR compliance, and data protection would be central to the project. Specialists in privacy and information governance would be involved to ensure that any information collected is handled safely, appropriately, and with proper consent.
Key Discussion: Why Are Carers Still Fighting the Same Battles?
A recurring theme throughout the meeting was the sense that many challenges identified today are the same challenges carers raised ten or twenty years ago.
Questions included:
Why are services still fragmented?
Why do carers continue to feel excluded?
Why are communication problems so persistent?
Why is trauma often overlooked?
Why do inequalities remain entrenched?
Participants reflected on whether the issue is primarily one of resources, leadership, service design, or culture.
Many agreed that meaningful change requires carers to remain actively involved in shaping policy and service delivery.
A carers support group recommended during discussion as a source of peer support and shared experience.
Final Reflections
The May 2026 Ethnic Mental Health Carers Forum highlighted both the challenges carers continue to face and the determination across the sector to improve outcomes.
From Mental Health Act reform and carers’ rights to innovative approaches such as Open Dialogue, the meeting demonstrated the importance of bringing together lived experience, research, policy, and practice.
Several speakers reminded attendees that change often begins with carers sharing their stories, participating in research, challenging poor practice, and helping shape future services.
The forum remains an important space where those voices can be heard.
On Tuesday 28th April 2026, from 2:00pm to 4:00pm, we came together at Cygnet Churchill in Lambeth for what was described as a carers poetry event, but in truth, it became something much deeper.
It became a space where carers could speak, reflect, and be heard.
I hosted the session not just as a PCREF Carer Lead, but as someone with lived experience. That shaped everything the tone, the structure, and the intention behind every part of the agenda.
I made it clear: this was a safe, inclusive, and optional space. No pressure to perform. No expectation to share. Just an invitation.
We began with a simple check-in: “What’s one word you’re arriving with?”
Opening Readings: Creating a Shared Starting Point
I started with a couple of my own poems, drawn from my work around carers, stigma, and racial inequality in mental health.
As shown above, one piece explored the question of who is listened to and who is overlooked within systems. Another focused on stigma and shame, particularly how cultural expectations and institutional barriers can compound the experience of caring.
These weren’t just readings—they were a way of opening the room. An invitation for others to see themselves reflected.
Featured Performer: Karen Ibrahim
We then heard from Karen Ibrahim, whose poetry captured something deeply familiar to many carers the quiet, often invisible emotional labour of caring.
Her piece reflected the silence between carer and loved one, the fear of saying the wrong thing, and the reality of sitting with someone in distress without always knowing how to help. It spoke to that fragile balance carers hold every day.
Karen also shared a series of haiku-style reflections, drawn from carer experiences—short, powerful snapshots of emotion, nature, and coping. They reminded us that even the smallest expressions can carry deep meaning.
Guided Writing Exercise #1: Bringing PCREF to Life
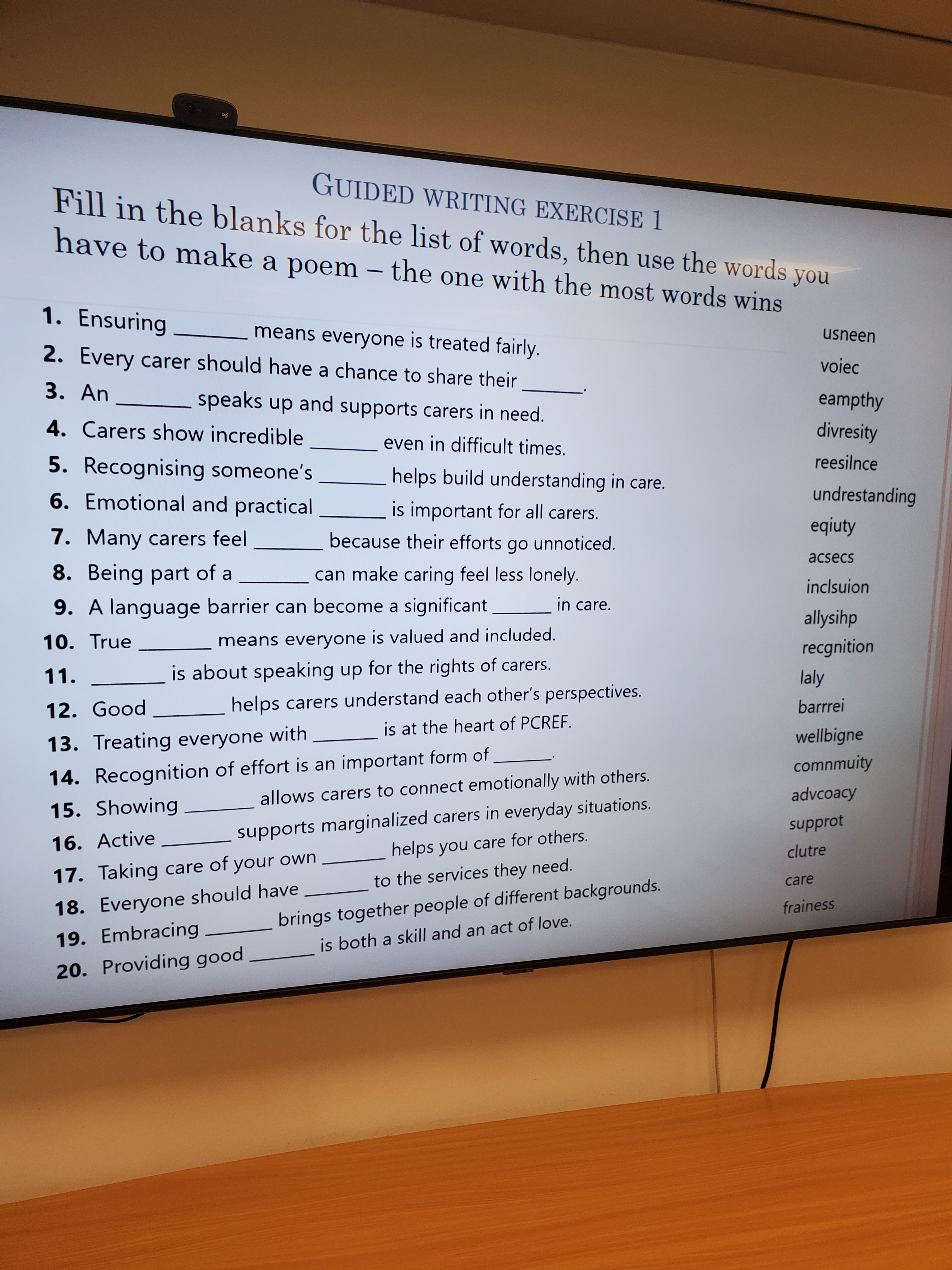
We then moved into the first guided writing exercise.
I paired participants and asked them to:
Match PCREF-related concepts (like equity, advocacy, inclusion, resilience) to their meanings
Use those words to create a short poem or reflection
It was about translating PCREF from policy into lived language.
The results were powerful. Carers wrote about 4 poems altogether, below were the themes, which will be included in the new PCREF poetry book I am working on.
Feeling unseen and unheard
Wanting their voice recognised
Breaking down barriers in care
Finding strength through community
One group asked: “Is my voice not loud enough to be heard?”
I felt that line stayed with me, because it captures exactly what PCREF is trying to address.
Performer & Open Mic (Round 1)
We then moved into our first round of performances, where carers shared both prepared and newly written work.
I felt Brenda brought something unique, blending cultural storytelling and poetry rooted in Jamaican heritage. She reflected on traditional knowledge, community wisdom, and the use of language and folklore as a way of preserving identity and healing. Her use of dialect and storytelling highlighted how culture shapes how we express and understand care.
Next was Annette Davis shared a piece centred on the identity of being a carer, capturing the emotional strain, lack of recognition, and inner strength that comes with the role. Her poem questioned what it means to be labelled a “carer” while navigating burnout, resilience, and the need for self-care.
Next up was Faith Smith and Nadine sharing a powerful reflection on system inequality, exploring the daily pressures of navigating services, the lack of accessible support, and the feeling of being caught in processes that don’t always respond to real-life needs.
Each piece added another layer to the conversation, with different perspectives, but shared truths.
Break & Connection
We paused for a short break and refreshments provided by the kind and wonderful staff at cygnet, but for the poetry event the conversations didn’t stop.
Carers continued to connect. Share stories. and reflected on what they had heard.
This is something I always emphasise, community doesn’t just happen in structured sessions. It happens in those in-between moments.
Creative Exercise session #2: Exploring PCREF Language
After the break, I introduced a second exercise, which was more interactive and reflective.
Participants worked with a word-search style challenge, identifying key PCREF-related terms such as:
Voice
Inclusion
Equity
Community
Trust
Advocacy
Listening
Stereotyping
Rather than writing full poems, we focused on discussion: Which word stands out and why?
The responses were honest and grounded:
“Listening builds trust.”
“Community is where we belong.”
“Inclusion is what drives change.”
“Stereotyping still shapes how we’re treated.”
This is where PCREF becomes real, when people recognise themselves within it.
Performer & Open Mic (Round 2)
We continued with a second round of performances.
Carers shared reflections shaped by:
Cultural identity
Personal caring journeys
The emotional impact of systems
Hope, resilience, and change
Then ended with cultural carer songs by Brenda, see the video of part of the PCREF poetry session below.
In the end PCREF is about improving outcomes for racialised communities—but it cannot succeed if it remains purely clinical.
We:
Translated PCREF into lived experience
Used creativity to engage carers meaningfully
Created a culturally responsive space
Positioned carers as equal voices not passive participants
If you are caring for someone using Cygnet services, contact Family&Friends@cygnethealth.co.uk to join our Voices & Verses poetry group
Recently, I had the privilege of attending and speaking at the West Kent Paddock Wood Group, and I wanted to take a moment to reflect on the experience, not just as a speaker, but as a mental health carer among peers who truly understand the journey.
The session took place at Unit 1 Eastlands, Maidstone Road in Paddock Wood, a welcoming and accessible venue that immediately set the tone for openness and support. From the moment I arrived, it was clear that this was a safe space. The event was hosted by Naomi Muigua who is the Social Care Involvement Officer.
The structure of the morning was thoughtfully organised, with time for introductions, discussion, and shared learning, all underpinned by respect, confidentiality, and equality among attendees .
A Community that works to understand carers
What stood out to me most was the diversity of lived experience in the room. Carers supporting loved ones with dementia, autism, and complex health needs came together, each bringing their own story, challenges, and resilience. It reinforced something I’ve long believed: carers often feel invisible in wider society, but in spaces like this, they are seen, heard, and valued.
The group is supported by organisations and professionals who are genuinely committed to reducing isolation and improving access to services. From digital inclusion to transport and community support, there’s a real effort to make sure carers are not left navigating the system alone
Sharing My Journey as a Mental Health Carer
As the invited speaker, I spoke from my own lived experience as a mental health carer. My journey began as a young carer supporting my mother, who developed schizophrenia, while also helping care for my brothers with non-verbal autism. Over the years, that experience has shaped not only my life, but my purpose.
During my talk, I shared:
The emotional reality of becoming a carer—often suddenly, without preparation
The confusion and isolation that can come with navigating mental health systems
The importance of recognising carers as partners in care, not just bystanders
The long-term impact on mental health, identity, and wellbeing
I also spoke about the concept of “lived experience”—something I feel strongly should be embedded in health and social care systems. If professionals are to truly understand and support carers, they need to hear directly from those who live it every day.
One of the key messages I left with the group was this: Carers are the hidden link that holds everything together. Without them, the system simply could not function.
This was taken from my poem off my book.
The Conversations of the group
What made the session particularly powerful wasn’t just the presentation, it was the discussion that followed. Carers openly spoke about:
Not knowing where to go for help
The complexity of accessing services
Feeling that outcomes often depend on how well you can advocate
The emotional toll of long-term caring
These are not small issues, they are systemic challenges. But spaces like this group allow those conversations to happen honestly, and more importantly, collectively.
Why Groups Like This Matter
The West Kent Paddock Wood Group is actually a lifeline to carers as it provides:
A supportive peer network
Access to information and local services
A platform for carers’ voices to be heard
A sense of belonging that many carers lack
For anyone who is caring for a loved one, especially in mental health, I cannot stress enough how important it is to connect with others who understand. You don’t have to do this alone.
Final Thoughts
Leaving the session, I felt both humbled and encouraged. Humbled by the strength of the carers in the room, and encouraged by the existence of a group that is actively working to support them.
If you are a carer in Kent, or even just exploring what support is available, I would strongly recommend attending the West Kent Paddock Wood Group. It is a space where your voice matters, your experience is valid, and your wellbeing is recognised.
For me, it was not just an opportunity to speak, it was an opportunity to connect, learn, and continue advocating for carers everywhere.
If you want to find out more about Kent County Council support for unpaid carers, see link below.
I feel Unpaid carers play a vital role in supporting loved ones experiencing mental health challenges. Much of this caring happens quietly in homes, during sleepless nights, through appointments, advocacy, and everyday acts of protection and support.
For many carers from minority communities, this experiences also includes navigating the cultural understanding, language differences, and systems that sometimes do not always recognise or reflect communities. Despite the knowledge carers hold, I feel our voices can sometimes feel overlooked in those decisions about care.
I recently wrote and recorded a short spoken word poem titled “Nothing About Us Without Us.” This poem reflects a simple and important message: carers bring lived experience that should be included in conversations about mental health services.
The poem is taken from the book I am developing called “Unpaid, Unseen and Yet Unbroken”
Carers are not just supporters in the background. Carers can carry knowledge shaped by lived reality by caring, advocating, and supporting our families through complex systems.
The poem also speaks to the importance of co-production. When carers, communities, and professionals work together, services can become more understanding and culturally responsive, and equitable.
I think this message is especially relevant to ongoing work around the Patient and Carer Race Equality Framework (PCREF), which encourages meaningful involvement of people with lived experience in shaping mental health services.
The poem is a small creative contribution to that conversation. It invites us to reflect on a few simple questions:
Are carers from different backgrounds being listened to?
Are those lived experiences shaping services?
Are decisions being made with carers, not about them?
Listening to carers is not just a gesture of inclusion it can lead to better understanding, stronger partnerships, and better care.
If you would like to watch the poem, you can find the video here:
I hope my poem encourages reflection and conversation about how we can continue building services with communities, and not just for them.
On 25th February 2026, I had the privilege of speaking at the Carers’ Forum hosted by Involve Kent.
Involve is a voluntary sector infrastructure organisation in Kent that supports unpaid carers by providing information, advice and practical help to make caring more manageable.
They organise regular carers’ forums and events where carers can meet each other, access specialist support services, hear from guest speakers on issues like benefits, legal rights and wellbeing, and contribute their lived experience to local planning and decision-making. Involve also connects carers with tailored resources, signposts to relevant services across health, social care and community sectors, and advocates for carers’ voices to be heard by policymakers and service providers
The forum ran from 10:30am to 1:30pm and brought together unpaid carers from across Kent to connect, learn and have their voices heard.
It was my second time speaking at this forum, and once again I was struck by something powerful: the room was full. That might sound simple, but in the world of unpaid caring which can often feel isolating and invisible a full room means solidarity. It means people are choosing, despite exhaustion and competing demands, to show up for themselves and each other.
Arriving and the atmosphere
From the moment I walked in, there was a real sense of warmth. Information stands lined the hall Involve, Citizens Advice, mental health services, energy advice, leisure services and more. Tables were covered in leaflets, conversations were already flowing, and carers were reconnecting with familiar faces.
The purpose of the forum was clear:
To enable those caring unpaid for an adult family member, partner or friend to meet, gain information about services in their community and have their voices heard .
That last part to have their voices heard is what resonated most with me.
It was also good to see Carer leads from Cygnet Maidstone engaging with carers in the community of Kent.
My talk: Caring for someone with a mental health diagnosis
I spoke about caring for someone with a mental health diagnosis and the Patient and Carer Race Equality Framework .
As many know, I cared for my mother who lived with schizophrenia, and I now support a close friend who lives with personality disorder and addiction challenges. I don’t speak as a clinician. I spoke as someone who has sat in GP waiting rooms, on inpatient wards, in crisis meetings, and at home during those “screaming silences” that carers know too well.
I shared:
The confusion I felt when I didn’t even realise I was a “carer”
The frustration of confidentiality barriers
The loneliness of not being listened to
The emotional exhaustion that comes from constantly firefighting crises
I then shared a poem to promote carers rights
But I also shared something equally important: growth, advocacy and solidarity.
I encouraged carers to:
Educate themselves about the condition they are supporting
Learn the difference between symptoms and personality
Understand triggers
Forgive themselves for mistakes
And most importantly, look after their own wellbeing
One message I always return to was – You cannot pour from an empty cup.
I also spoke about The Patient Carer Race Equality Framework
It exists because there is clear evidence of:
Disproportionate detentions under the Mental Health Act
Poorer outcomes for Black and minority ethnic patients
Higher levels of distrust between communities and services
Carers feeling unheard or excluded
I spoke about how minority carers can face:
Cultural misunderstandings
Language barriers
Stigma around mental health within communities
Fear of services due to past discrimination
A lack of culturally appropriate support
Discussion tables: Carers influencing change
After my talk, Clara from Involve led discussions feeding into Kent’s Health Needs Assessment for carers. Carers were asked:
How do you recognise when it’s time to ask for help?
What causes burnout?
What would a carer-friendly community look like?
These wete not token questions. Staff took notes (without identifying details) so carers’ lived experiences could directly inform local planning .
I moved around the room speaking with carers. Some were open and vocal. Others were quieter, but their listening was just as powerful. Not everyone wants to speak publicly and that’s okay. Being present is also participation too.
Power of Attorney – protecting your voice
Later in the morning, Glen Miles spoke about the Mental Capacity Act and Lasting Power of Attorney .
As carers, we often assume we will automatically be consulted in crises. The reality is different. Without legal authority, our ability to advocate can be limited.
One key takeaway:
Don’t delay in arranging Lasting Powers of Attorney.
If you want your voice – or your loved one’s voice – to be heard, formalise it.
For carers who have experienced being excluded from decisions, this was a particularly important session.
Citizens Advice & practical support
Ian from Citizens Advice spoke before lunch about benefits, debt, housing and confidential support .
With the cost of living crisis, carers are under immense financial pressure. Many reduce employment hours or leave work entirely. The session was a reminder that:
Advice is free
It is confidential
You can attend anonymously
You are not judged
Lunch followed – catered by Fusion – and honestly, some of the most meaningful conversations happen over sandwiches. Carers swapping stories. Sharing phone numbers. Recommending services. That peer-to-peer support is priceless.
What stayed with me
What stayed with me most wasn’t just the agenda or the presentations.
It was:
The older carer quietly nodding as I spoke about emotional exhaustion.
The new carer asking, “Is it normal to feel this angry sometimes?”
The male carers who stayed behind to speak to me privately.
The carers from minority backgrounds who spoke about cultural barriers and stigma.
These forums matter because carers matter.
Unpaid carers save the system billions. But beyond economics, we hold families together. We absorb crises. We advocate in rooms where we’re not always welcomed.
If you’re an unpaid carer in Southwark, chances are you’re used to putting everyone else first. You support a loved one day in, day out, emotionally, practically, often invisibly. And too often, decisions about “support” for carers are made without carers truly being heard.
Southwark Council is developing its Unpaid Carers Strategy, and they are inviting unpaid carers to take part in upcoming focus groups to share real experiences, which are your lived reality.
As an unpaid carer myself, I know how rare and valuable this opportunity is.
Why having your say is important because
Policies and strategies shape:
What support is available
How easy (or hard) it is to access help
Whether carers feel recognised, supported, and understood
When carers don’t speak up, systems are built around us, not with us. When we do speak up, its a chance to make change becomes possible.
This isn’t about complaining. It’s about being honest: what works, what doesn’t, and what would genuinely make life easier for carers in Southwark.
Your voice could help shape:
Better access to information and services
More flexible, carer-friendly support
A strategy that reflects the real pressures carers face
A safe, non-judgemental space
One of the most important things about these focus groups is that they are designed to be:
Non-judgemental
Inclusive
Open to carers with any level of responsibility
You don’t need to have all the answers. You don’t need to be an “expert”. You just need your experience.
Whether you care full-time, part-time, occasionally, or don’t even label yourself as a “carer” your perspective still counts.
Focus group dates and details
In-person focus groups 📅 24th February ⏰ 11am – 1pmand2pm – 4pm 📍 Harriet Hardy Community Centre Harriet-Hardy Building, Aylesbury Estate, Albany Road, Walworth SE5 0AH
Online focus group 📅 25th February ⏰ 7pm 💻 Virtual session via Microsoft Teams
How to get involved
You can:
Scan the QR code on the flyer shown above my blog to register your interest
Our final Triangle of Care (ToC) Community Group meeting of the year brought together carers, professionals, and ToC members from across the UK to share updates, raise concerns, and discuss priorities for 2026 and beyond. Although Microsoft Teams provided some surprises, we made it work, thanks to teamwork and patience. The conversation was rich, heartfelt, and often very moving.
1. Opening & Agenda
As chair of the meeting, I acknowledged technical teething problems as the group used Teams for the first time in this format. Mary (ToC Programme Lead) welcomed attendees and explained the privacy-driven decision to hide email addresses, which also unfortunately hid attendees’ names. A fix will be implemented before the January meeting.
The agenda included:
Triangle of Care national updates (Mary)
Carer co-production and lived experience input (Matthew)
Surrey & Borders’ co-production example (postponed)
Research priority-setting presentation (Richard, University of Manchester)
Carer questions and discussion
2. Triangle of Care National Update (Mary)
Mary provided a comprehensive end-of-year update structured around ToC’s three priority areas for 2024–25.
2.1 Embedding the Relaunched Triangle of Care Framework
Growth & progress
16 new members have joined the scheme since April, bringing ToC membership to over 80.
The first Welsh hospital achieved a ToC Star Award, prompting the creation of a new Welsh-language logo and Welsh materials.
A social care pilot is underway with Livewell South West, with West Hertfordshire Teaching Hospital reviewing ToC criteria for an acute setting.
Nine Star Awards have been achieved this year, with a further 12 annual reviews approved. Many more annual reports are pending review before year-end.
Standardising data Mary emphasised the push for consistent reporting across Trusts, including:
numbers of carers identified
uptake of carer awareness training
numbers of carer champions
This will help build a national picture of impact.
Webinars ToC’s Lunch & Learn series continues, with the recent Carers Rights Day webinar (in partnership with University of Bristol) focusing on the Nearest Relative role under the Mental Health Act (MHA). Resources are available via Carers Trust’s YouTube channel.
2.2 Young Carers: Identification & Support
A major update was the successful national policy win relating to young carers and the Mental Health Act.
Mental Health Act Reform – Safety Net for Young Carers
Following campaigning by Carers Trust, the Young Carers Alliance, and ToC members who wrote to MPs:
Government has agreed to update the MHA Code of Practice to require:
identification of children when an adult is detained
sharing of information about available support
referrals for young carer needs assessments
Updates to advance choice documents will require practitioners to ask about dependent children.
Expected implementation: Summer 2026.
This win was warmly welcomed by the group.
2.3 Racially Minoritised Carers & PCREF
Mary updated members on ToC’s work to ensure carers are fully represented in the Patient & Carer Race Equality Framework (PCREF).
Key updates
A national Task & Finish Group has now completed its review of the first four ToC standards; the final standard is underway.
Piloting of new culturally sensitive criteria is planned with 10 NHS Trusts beginning April 2026.
Example of early good practice: Livewell South West is implementing a new “essential data template” that includes carers, enabling services to better identify and support racially minoritised carers.
Carers Trust is calling for a statutory duty for NHS mental health providers to implement PCREF in full, including community governance.
2.4 Changing the Narrative on Care – New Research
Mary introduced new research (supported by the Health Foundation and Oxfam GB) titled Changing the Narrative on Care, highlighting:
Although 80% of the public value unpaid care, this does not translate into policy action or investment.
Three recommended reframes:
Care is a universal experience, not a niche issue.
No care without support, make support visible and tangible.
Care is a partnership between families, communities and systems—not something families must do alone.
The full report is available on Carers Trust’s website.
I then presented an in-depth reflection on the value of authentic carer involvement, drawing on his lived experience and his role working with multiple NHS organisations.
Key points included:
Carers are not passive observers, they hold critical lived knowledge that improves services.
Real co-production goes beyond consultation; carers must be equal partners in shaping policy, documentation, training, and strategic decisions.
Examples Matthew gave from his own involvement:
redesigning welcome packs and leaflets
addressing confidentiality misapplication
involvement in recruitment panels
delivering training to staff at induction
reviewing complaints and compliments themes
advising on discharge processes and family-inclusive safety protocols
participating in research steering groups
Carers’ insight is especially essential in safeguarding, quality boards, and identifying service gaps often invisible to professionals.
4. Surrey & Borders Co-Production Example
A planned presentation from Surrey & Borders was postponed, as the relevant colleague could not attend with materials. They hope to present at a future meeting.
5. Research Priority Setting in Secure & Forensic Mental Health (Richard Kears)
Richard introduced a national project with the James Lind Alliance (JLA) aiming to identify the top 10 research priorities for secure and forensic mental health services across England, Scotland and Wales.
Who is the survey for?
Carers
People with lived experience of secure/forensic services
Staff working in these services
Anyone indirectly connected (victims, families)
Purpose
To ensure future mental health research is led by the real concerns of those most affected, not only by academics or pharmaceutical interests.
Process
National survey gathering research questions.
Analysis to identify common themes.
Second, more focused survey to refine priorities.
National workshops with carers, staff and people with lived experience to finalise the top 10.
A QR code and flyer were shared for distribution. The group expressed strong support.
6. Attendee Discussion & Questions
This was the richest section of the meeting, with many heartfelt contributions. The themes below reflect the key concerns raised.
6.1 Scotland & UK-wide ToC Alignment
A carer asked why Scotland’s ToC framework is separate and not integrated into the UK ToC accreditation model. Mary explained:
Scotland currently uses ToC only as a free policy framework.
Implementing the accreditation model in Scotland would require groundwork to assess willingness and ability of providers to fund membership.
Integration is being discussed but is not imminent.
6.2 Clarity on Co-Production
Several carers voiced concerns that:
“Co-production” is often used as a buzzword.
Some NHS Trusts label work as co-produced after completing it.
Carers need clarity on what ToC means when using the term.
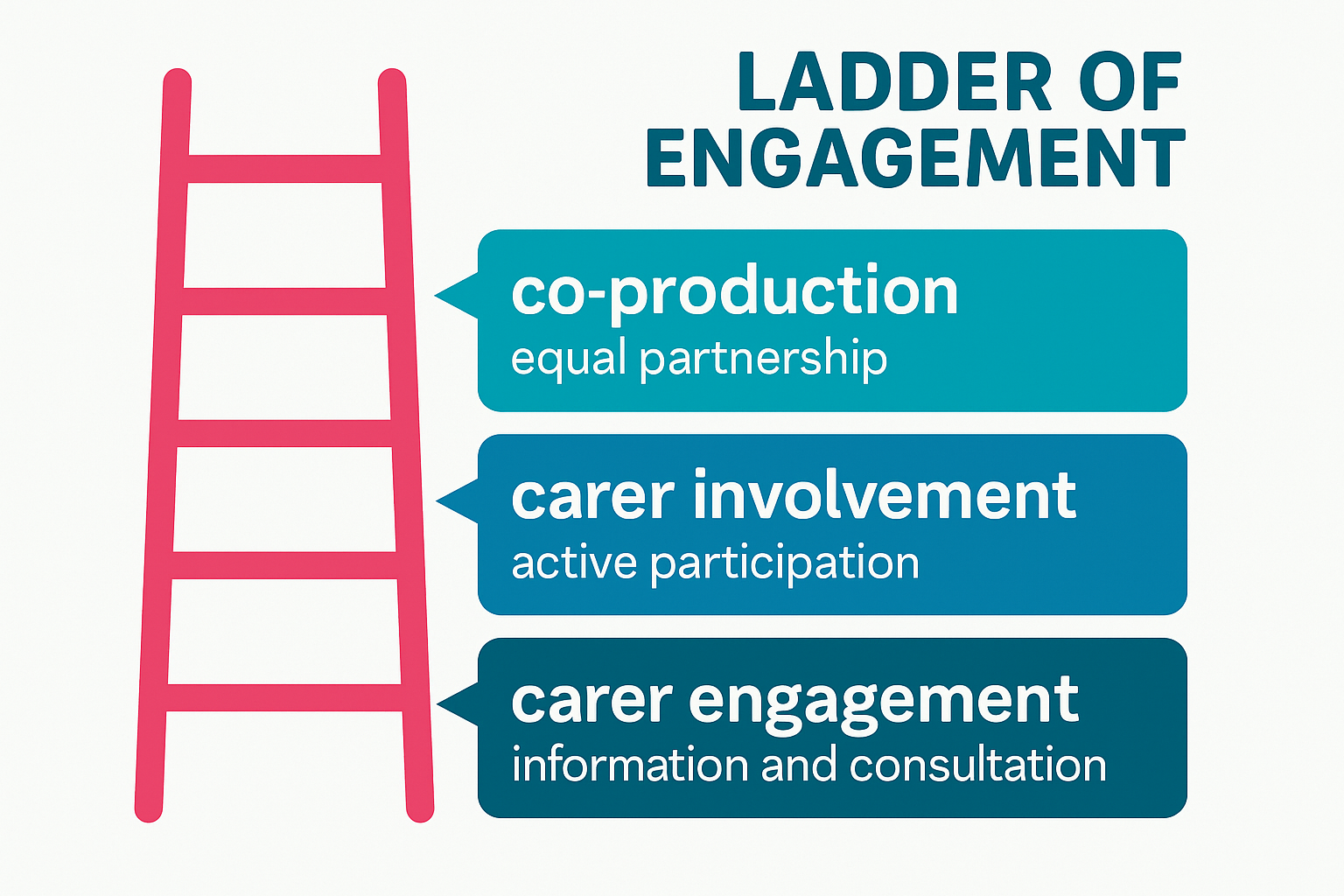
Mary responded that ToC uses a ladder of engagement, distinguishing:
carer engagement
carer involvement
full co-production
Carers Trust is developing a formal principles-based statement on involvement for future meetings.
6.3 Older Carers: Visibility, Support & Inequalities
The majority of carer questions focused on the unmet needs of older adult carers, many of whom are supporting people with severe mental illness—not dementia—and often have been caring 20–40 years.
Attendees reported:
Feeling “invisible” within both policy and services.
Being incorrectly grouped under “older carers = dementia”.
Their own poor health affecting their caring ability.
Increasing struggle to get responses from professionals.
Serious concerns about who will care for their loved ones when they die.
Feeling less heard as they age, compared with younger carers or newer voices.
One carer (age 78) shared:
“I can’t retire from caring. Benefits stop at 65, but the caring doesn’t.”
Another said:
“We have to shout louder as older women to be heard—and still we aren’t.”
Mary acknowledged the seriousness of these issues and committed to:
bringing older carers’ concerns into ongoing ToC work
exploring dedicated guidance and better mainstreaming within the ToC standards
sharing good practice on carer contingency planning in upcoming meetings
I also reiterated the group’s role in surfacing policy gaps and influencing future national lobbying.
6.4 Carer Registration & Meeting Access
Several carers raised issues with:
The length of the ToC sign-up form
Not receiving meeting links despite signing up
Verification barriers when joining Teams
Mary agreed to:
review and shorten the form
clarify which fields are optional
address email deliverability issues
adjust MS Teams settings to reduce joining friction while maintaining security
6.5 Concerns About Confidentiality Misuse
One carer reported that in a CQC meeting at an NHS Trust, raising questions about communication was dismissed as “confidentiality”, preventing meaningful dialogue. I then encouraged carers to bring such examples into:
ToC Star peer reviews
Carer involvement forums
Local advocacy routes
He noted that misuse of confidentiality is a common and unacceptable barrier and must be challenged.
6.6 Petition on Antipsychotic Medication Research
Carers highlighted concerns about:
long-term prescribing of antipsychotics
lack of regular medication review
inadequate research into long-term effects
A carer shared a petition calling for investigation of psychiatric medications. Richard noted that he had signed and shared it previously.
7. Closing Remarks
Matthew thanked all attendees for their honesty, passion and persistence:
“Carers’ voices shape policies and improve care. That is exactly what this group is here to do.”
Mary acknowledged:
the importance of every concern raised
the need to better support older carers
improvements to ToC communications and meeting accessibility
that the next meeting will be in January (provisionally 19th)
The meeting closed with gratitude from carers who said they felt heard, supported, and connected.