I feel Unpaid carers play a vital role in supporting loved ones experiencing mental health challenges. Much of this caring happens quietly in homes, during sleepless nights, through appointments, advocacy, and everyday acts of protection and support.
For many carers from minority communities, this experiences also includes navigating the cultural understanding, language differences, and systems that sometimes do not always recognise or reflect communities. Despite the knowledge carers hold, I feel our voices can sometimes feel overlooked in those decisions about care.
I recently wrote and recorded a short spoken word poem titled “Nothing About Us Without Us.” This poem reflects a simple and important message: carers bring lived experience that should be included in conversations about mental health services.
The poem is taken from the book I am developing called “Unpaid, Unseen and Yet Unbroken”
Carers are not just supporters in the background. Carers can carry knowledge shaped by lived reality by caring, advocating, and supporting our families through complex systems.
The poem also speaks to the importance of co-production. When carers, communities, and professionals work together, services can become more understanding and culturally responsive, and equitable.
I think this message is especially relevant to ongoing work around the Patient and Carer Race Equality Framework (PCREF), which encourages meaningful involvement of people with lived experience in shaping mental health services.
The poem is a small creative contribution to that conversation. It invites us to reflect on a few simple questions:
Are carers from different backgrounds being listened to?
Are those lived experiences shaping services?
Are decisions being made with carers, not about them?
Listening to carers is not just a gesture of inclusion it can lead to better understanding, stronger partnerships, and better care.
If you would like to watch the poem, you can find the video here:
I hope my poem encourages reflection and conversation about how we can continue building services with communities, and not just for them.
On 25th February 2026, I had the privilege of speaking at the Carers’ Forum hosted by Involve Kent.
Involve is a voluntary sector infrastructure organisation in Kent that supports unpaid carers by providing information, advice and practical help to make caring more manageable.
They organise regular carers’ forums and events where carers can meet each other, access specialist support services, hear from guest speakers on issues like benefits, legal rights and wellbeing, and contribute their lived experience to local planning and decision-making. Involve also connects carers with tailored resources, signposts to relevant services across health, social care and community sectors, and advocates for carers’ voices to be heard by policymakers and service providers
The forum ran from 10:30am to 1:30pm and brought together unpaid carers from across Kent to connect, learn and have their voices heard.
It was my second time speaking at this forum, and once again I was struck by something powerful: the room was full. That might sound simple, but in the world of unpaid caring which can often feel isolating and invisible a full room means solidarity. It means people are choosing, despite exhaustion and competing demands, to show up for themselves and each other.
Arriving and the atmosphere
From the moment I walked in, there was a real sense of warmth. Information stands lined the hall Involve, Citizens Advice, mental health services, energy advice, leisure services and more. Tables were covered in leaflets, conversations were already flowing, and carers were reconnecting with familiar faces.
The purpose of the forum was clear:
To enable those caring unpaid for an adult family member, partner or friend to meet, gain information about services in their community and have their voices heard .
That last part to have their voices heard is what resonated most with me.
It was also good to see Carer leads from Cygnet Maidstone engaging with carers in the community of Kent.
My talk: Caring for someone with a mental health diagnosis
I spoke about caring for someone with a mental health diagnosis and the Patient and Carer Race Equality Framework .
As many know, I cared for my mother who lived with schizophrenia, and I now support a close friend who lives with personality disorder and addiction challenges. I don’t speak as a clinician. I spoke as someone who has sat in GP waiting rooms, on inpatient wards, in crisis meetings, and at home during those “screaming silences” that carers know too well.
I shared:
The confusion I felt when I didn’t even realise I was a “carer”
The frustration of confidentiality barriers
The loneliness of not being listened to
The emotional exhaustion that comes from constantly firefighting crises
I then shared a poem to promote carers rights
But I also shared something equally important: growth, advocacy and solidarity.
I encouraged carers to:
Educate themselves about the condition they are supporting
Learn the difference between symptoms and personality
Understand triggers
Forgive themselves for mistakes
And most importantly, look after their own wellbeing
One message I always return to was – You cannot pour from an empty cup.
I also spoke about The Patient Carer Race Equality Framework
It exists because there is clear evidence of:
Disproportionate detentions under the Mental Health Act
Poorer outcomes for Black and minority ethnic patients
Higher levels of distrust between communities and services
Carers feeling unheard or excluded
I spoke about how minority carers can face:
Cultural misunderstandings
Language barriers
Stigma around mental health within communities
Fear of services due to past discrimination
A lack of culturally appropriate support
Discussion tables: Carers influencing change
After my talk, Clara from Involve led discussions feeding into Kent’s Health Needs Assessment for carers. Carers were asked:
How do you recognise when it’s time to ask for help?
What causes burnout?
What would a carer-friendly community look like?
These wete not token questions. Staff took notes (without identifying details) so carers’ lived experiences could directly inform local planning .
I moved around the room speaking with carers. Some were open and vocal. Others were quieter, but their listening was just as powerful. Not everyone wants to speak publicly and that’s okay. Being present is also participation too.
Power of Attorney – protecting your voice
Later in the morning, Glen Miles spoke about the Mental Capacity Act and Lasting Power of Attorney .
As carers, we often assume we will automatically be consulted in crises. The reality is different. Without legal authority, our ability to advocate can be limited.
One key takeaway:
Don’t delay in arranging Lasting Powers of Attorney.
If you want your voice – or your loved one’s voice – to be heard, formalise it.
For carers who have experienced being excluded from decisions, this was a particularly important session.
Citizens Advice & practical support
Ian from Citizens Advice spoke before lunch about benefits, debt, housing and confidential support .
With the cost of living crisis, carers are under immense financial pressure. Many reduce employment hours or leave work entirely. The session was a reminder that:
Advice is free
It is confidential
You can attend anonymously
You are not judged
Lunch followed – catered by Fusion – and honestly, some of the most meaningful conversations happen over sandwiches. Carers swapping stories. Sharing phone numbers. Recommending services. That peer-to-peer support is priceless.
What stayed with me
What stayed with me most wasn’t just the agenda or the presentations.
It was:
The older carer quietly nodding as I spoke about emotional exhaustion.
The new carer asking, “Is it normal to feel this angry sometimes?”
The male carers who stayed behind to speak to me privately.
The carers from minority backgrounds who spoke about cultural barriers and stigma.
These forums matter because carers matter.
Unpaid carers save the system billions. But beyond economics, we hold families together. We absorb crises. We advocate in rooms where we’re not always welcomed.
The Patient and Carer Race Equality Framework (PCREF) is a landmark policy designed to improve racial equity in NHS mental health care. But if it’s going to deliver meaningful change, one key voice must be placed at its centre: the carer.
Watch the video
Putting the “C” (Carer) into PCREF
In this vlog, I explore why unpaid ethnic minority carers — who are often the backbone of support for people with mental health needs — are still too often excluded from decision-making, planning, and implementation in services designed to support both them and their loved ones
A Shared Movement
Integrating PCREF and Triangle of Care is a commitment to transforming relationships in mental health care.
Carers are not just an add-on. They are central to safe, equitable, and culturally competent services.
Watch the video above, share your thoughts, and join the conversation.
By Matthew McKenzie, facilitator of National ethnic mental health carers forum
Welcome to my first blog for 2026.
I am working on a new poetry project linked to my forum and poetry groups. This poem turned into song is written from the perspective of an unpaid ethnic mental health carer, and explores identity, pride, self-worth, and refusing shame in systems that don’t always listen or recognise lived experience.
The poem is taken from my forthcoming poetry book in development, Unpaid, Unseen and Yet Unbroken (due 2026), which centres the voices of ethnic mental health carers and aligns closely with the aims of PCREF (Patient and Carer Race Equality Framework), particularly around listening, inclusion, and lived experience shaping systems.
I’m using poetry and creative formats as another way to:
amplify carer voices
explore race and care with honesty
support conversations about equity, culture, and confidence in mental health services
If this resonates with your work, community, or organisation, please feel free to share. Listening is an act of care.
Matthew McKenzie FRSA BEM, poet and advocate for unpaid ethnic mental health carers, is inviting carers involved in NHS Trusts, PCREF (Patient and Carer Race Equality Framework), and Trust involvement registers to submit their poems for an upcoming 2026 poetry collection. This collection will spotlight minority carers’ voices and explore themes of race, culture, and lived experience in mental health care.
About the Poetry Collection
The collection will focus on amplifying minority carers’ experiences through poetry. It will be part of the paperback version of Matthew’s upcoming poetry book Unpaid, Unseen and Yet Unbroken and will include poems from carers all over the country. This is a unique opportunity for minority ethnic carers to have their voices heard and their stories shared on a national platform, contributing to the ongoing conversation about race equality, care, and mental health.
Why Should You Submit a Poem?
If you’re a minority carer or carers from underrepresented community, your voice matters. PCREF is committed to creating systemic change, and this collection will work alongside it to ensure that carers from minority communities are not left unheard. Submitting your poem gives you the chance to:
Raise awareness of the emotional, cultural, and psychological realities of being a carer.
Inspire others by sharing your lived experience.
Amplify minority voices within NHS Trusts, PCREF spaces, and mental health care systems.
Who Can Submit?
We welcome submissions from unpaid ethnic mental health carers who are:
Involved in NHS Trusts, PCREF, or trust involvement registers.
Attending ethnic mental health carer peer groups at carer centres
Interested in sharing their personal experiences and reflections through poetry.
How to Submit Your Poem:
Submit an original poem that reflects the emotional, cultural, and psychological realities of being an unpaid mental health carer.
Poems can focus on themes such as:
Emotional challenges of care
The hidden burden of caring
Resilience and survival
Navigating mental health services
Coping with racial and cultural barriers in care
Family dynamics in caregiving
Deadline for submissions is late April 2026.
Submission Guidelines:
Format: Poems can be submitted in Word, PDF, or plain text format.
Length: There is no strict length, but we recommend that submissions be no longer than 1 page.
Multiple submissions: You can submit more than one poem if desired.
Contact Information: Please include your full name, contact details along with your poem, so i can credit you. Unless you wish to be anonymous.
You can also reach out to Matthew directly if you have any questions about the submission process or the collection.
What Happens After You Submit?
Once submissions are received, I will review all entries and select poems that align with the themes of the collection. All selected poets will be notified and credited in the final publication.
Need Inspiration or Support?
If you’re unsure where to start or need some encouragement, consider reflecting on your personal journey as a carer. Think about moments where language failed to express your experience or times when your strength surprised you. Your story is valuable, and this collection is about lifting up voices that have often been overlooked.
Contact Information:
For any questions or additional information, please contact Matthew McKenzie:
This is your chance to raise awareness and inspire others by sharing your lived experiences through poetry. Help shape a future where minority carers are valued, heard, and recognized for the essential work they do. We look forward to reading your stories!
By Matthew Mckenzie – facilitator of national ethnic mental health carers forum
I’m pleased to share “Unpaid, Unseen and Yet Unbroken”, a spoken word poetry video that marks the first poem released from my forthcoming poetry collection of the same name.
This first poem speaks from within the lived reality of unpaid mental health carers, particularly those from ethnic and marginalised communities whose labour is often overlooked, misunderstood, or taken for granted. It reflects moments many carers will recognise: waiting rooms, misrecognition, quiet endurance, and the strength it takes to keep showing up without acknowledgement.
🎥 Watch the spoken word video here:
The wider collection I am currently working on brings together poems shaped by care, fatigue, love, resilience, and survival. It is a body of work rooted in lived experience and community voices, offering poetry not only as expression, but as witness and affirmation.
This first poem sets the tone for what is to come, promoting honest, reflective, and unapologetic in its call for carers to be seen, heard, and respected.
This work is part of my ongoing commitment through my A Caring Mind youtube channel to use creativity as a way to challenge stigma, amplify unheard voices, and centre care as a vital social contribution.
More poems from this collection will be shared in the coming months.
Our final Triangle of Care (ToC) Community Group meeting of the year brought together carers, professionals, and ToC members from across the UK to share updates, raise concerns, and discuss priorities for 2026 and beyond. Although Microsoft Teams provided some surprises, we made it work, thanks to teamwork and patience. The conversation was rich, heartfelt, and often very moving.
1. Opening & Agenda
As chair of the meeting, I acknowledged technical teething problems as the group used Teams for the first time in this format. Mary (ToC Programme Lead) welcomed attendees and explained the privacy-driven decision to hide email addresses, which also unfortunately hid attendees’ names. A fix will be implemented before the January meeting.
The agenda included:
Triangle of Care national updates (Mary)
Carer co-production and lived experience input (Matthew)
Surrey & Borders’ co-production example (postponed)
Research priority-setting presentation (Richard, University of Manchester)
Carer questions and discussion
2. Triangle of Care National Update (Mary)
Mary provided a comprehensive end-of-year update structured around ToC’s three priority areas for 2024–25.
2.1 Embedding the Relaunched Triangle of Care Framework
Growth & progress
16 new members have joined the scheme since April, bringing ToC membership to over 80.
The first Welsh hospital achieved a ToC Star Award, prompting the creation of a new Welsh-language logo and Welsh materials.
A social care pilot is underway with Livewell South West, with West Hertfordshire Teaching Hospital reviewing ToC criteria for an acute setting.
Nine Star Awards have been achieved this year, with a further 12 annual reviews approved. Many more annual reports are pending review before year-end.
Standardising data Mary emphasised the push for consistent reporting across Trusts, including:
numbers of carers identified
uptake of carer awareness training
numbers of carer champions
This will help build a national picture of impact.
Webinars ToC’s Lunch & Learn series continues, with the recent Carers Rights Day webinar (in partnership with University of Bristol) focusing on the Nearest Relative role under the Mental Health Act (MHA). Resources are available via Carers Trust’s YouTube channel.
2.2 Young Carers: Identification & Support
A major update was the successful national policy win relating to young carers and the Mental Health Act.
Mental Health Act Reform – Safety Net for Young Carers
Following campaigning by Carers Trust, the Young Carers Alliance, and ToC members who wrote to MPs:
Government has agreed to update the MHA Code of Practice to require:
identification of children when an adult is detained
sharing of information about available support
referrals for young carer needs assessments
Updates to advance choice documents will require practitioners to ask about dependent children.
Expected implementation: Summer 2026.
This win was warmly welcomed by the group.
2.3 Racially Minoritised Carers & PCREF
Mary updated members on ToC’s work to ensure carers are fully represented in the Patient & Carer Race Equality Framework (PCREF).
Key updates
A national Task & Finish Group has now completed its review of the first four ToC standards; the final standard is underway.
Piloting of new culturally sensitive criteria is planned with 10 NHS Trusts beginning April 2026.
Example of early good practice: Livewell South West is implementing a new “essential data template” that includes carers, enabling services to better identify and support racially minoritised carers.
Carers Trust is calling for a statutory duty for NHS mental health providers to implement PCREF in full, including community governance.
2.4 Changing the Narrative on Care – New Research
Mary introduced new research (supported by the Health Foundation and Oxfam GB) titled Changing the Narrative on Care, highlighting:
Although 80% of the public value unpaid care, this does not translate into policy action or investment.
Three recommended reframes:
Care is a universal experience, not a niche issue.
No care without support, make support visible and tangible.
Care is a partnership between families, communities and systems—not something families must do alone.
The full report is available on Carers Trust’s website.
I then presented an in-depth reflection on the value of authentic carer involvement, drawing on his lived experience and his role working with multiple NHS organisations.
Key points included:
Carers are not passive observers, they hold critical lived knowledge that improves services.
Real co-production goes beyond consultation; carers must be equal partners in shaping policy, documentation, training, and strategic decisions.
Examples Matthew gave from his own involvement:
redesigning welcome packs and leaflets
addressing confidentiality misapplication
involvement in recruitment panels
delivering training to staff at induction
reviewing complaints and compliments themes
advising on discharge processes and family-inclusive safety protocols
participating in research steering groups
Carers’ insight is especially essential in safeguarding, quality boards, and identifying service gaps often invisible to professionals.
4. Surrey & Borders Co-Production Example
A planned presentation from Surrey & Borders was postponed, as the relevant colleague could not attend with materials. They hope to present at a future meeting.
5. Research Priority Setting in Secure & Forensic Mental Health (Richard Kears)
Richard introduced a national project with the James Lind Alliance (JLA) aiming to identify the top 10 research priorities for secure and forensic mental health services across England, Scotland and Wales.
Who is the survey for?
Carers
People with lived experience of secure/forensic services
Staff working in these services
Anyone indirectly connected (victims, families)
Purpose
To ensure future mental health research is led by the real concerns of those most affected, not only by academics or pharmaceutical interests.
Process
National survey gathering research questions.
Analysis to identify common themes.
Second, more focused survey to refine priorities.
National workshops with carers, staff and people with lived experience to finalise the top 10.
A QR code and flyer were shared for distribution. The group expressed strong support.
6. Attendee Discussion & Questions
This was the richest section of the meeting, with many heartfelt contributions. The themes below reflect the key concerns raised.
6.1 Scotland & UK-wide ToC Alignment
A carer asked why Scotland’s ToC framework is separate and not integrated into the UK ToC accreditation model. Mary explained:
Scotland currently uses ToC only as a free policy framework.
Implementing the accreditation model in Scotland would require groundwork to assess willingness and ability of providers to fund membership.
Integration is being discussed but is not imminent.
6.2 Clarity on Co-Production
Several carers voiced concerns that:
“Co-production” is often used as a buzzword.
Some NHS Trusts label work as co-produced after completing it.
Carers need clarity on what ToC means when using the term.
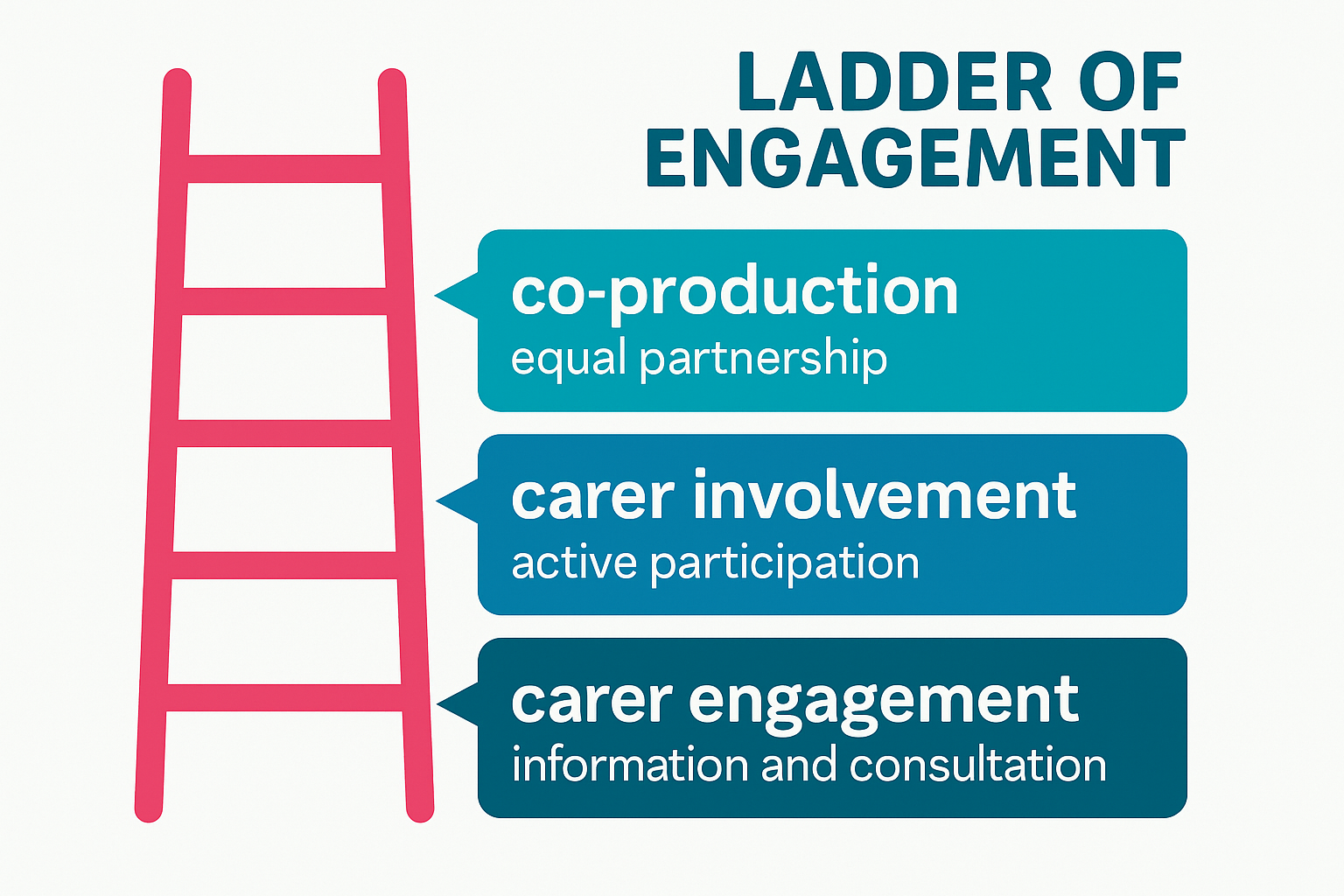
Mary responded that ToC uses a ladder of engagement, distinguishing:
carer engagement
carer involvement
full co-production
Carers Trust is developing a formal principles-based statement on involvement for future meetings.
6.3 Older Carers: Visibility, Support & Inequalities
The majority of carer questions focused on the unmet needs of older adult carers, many of whom are supporting people with severe mental illness—not dementia—and often have been caring 20–40 years.
Attendees reported:
Feeling “invisible” within both policy and services.
Being incorrectly grouped under “older carers = dementia”.
Their own poor health affecting their caring ability.
Increasing struggle to get responses from professionals.
Serious concerns about who will care for their loved ones when they die.
Feeling less heard as they age, compared with younger carers or newer voices.
One carer (age 78) shared:
“I can’t retire from caring. Benefits stop at 65, but the caring doesn’t.”
Another said:
“We have to shout louder as older women to be heard—and still we aren’t.”
Mary acknowledged the seriousness of these issues and committed to:
bringing older carers’ concerns into ongoing ToC work
exploring dedicated guidance and better mainstreaming within the ToC standards
sharing good practice on carer contingency planning in upcoming meetings
I also reiterated the group’s role in surfacing policy gaps and influencing future national lobbying.
6.4 Carer Registration & Meeting Access
Several carers raised issues with:
The length of the ToC sign-up form
Not receiving meeting links despite signing up
Verification barriers when joining Teams
Mary agreed to:
review and shorten the form
clarify which fields are optional
address email deliverability issues
adjust MS Teams settings to reduce joining friction while maintaining security
6.5 Concerns About Confidentiality Misuse
One carer reported that in a CQC meeting at an NHS Trust, raising questions about communication was dismissed as “confidentiality”, preventing meaningful dialogue. I then encouraged carers to bring such examples into:
ToC Star peer reviews
Carer involvement forums
Local advocacy routes
He noted that misuse of confidentiality is a common and unacceptable barrier and must be challenged.
6.6 Petition on Antipsychotic Medication Research
Carers highlighted concerns about:
long-term prescribing of antipsychotics
lack of regular medication review
inadequate research into long-term effects
A carer shared a petition calling for investigation of psychiatric medications. Richard noted that he had signed and shared it previously.
7. Closing Remarks
Matthew thanked all attendees for their honesty, passion and persistence:
“Carers’ voices shape policies and improve care. That is exactly what this group is here to do.”
Mary acknowledged:
the importance of every concern raised
the need to better support older carers
improvements to ToC communications and meeting accessibility
that the next meeting will be in January (provisionally 19th)
The meeting closed with gratitude from carers who said they felt heard, supported, and connected.
Chaired by Matthew McKenzie, Lived-Experience Carer
The latest meeting of the National Ethnic Mental Health Carer Forum brought together unpaid minority carers, community partners and four NHS mental Trusts (Avon & Whiltshire were kind enough to be included to update) to explore progress toward the Patient & Carer Race Equality Framework (PCREF), share challenges, and elevate lived-experience voices. As always, I ensured the space remained honest, fast-paced and rooted in what truly matters to ethnic minority carers: being heard, understood and included.
My latest blog for the November forum captures key highlights from each Trust, along with questions raised by attendees, reflecting the critical concerns and lived realities that continue to shape PCREF work across the country.
1. Avon & Wiltshire Mental Health Partnership Trust (AWP)
Focus: Triangle of Care, PCREF oversight, carer champion roles.
Avon & Wiltshire outlined how their PCREF programme is being driven through a clear governance structure, including a central Oversight Group and locality-based meetings. These layers ensure that learning from communities and staff filters upward and influences whole-trust priorities. Their collaboration with Nilaari (I think that is what their called), a long-standing community organisation supporting racially marginalised groups, has been key in grounding their PCREF work in authentic community voice.
A central pillar of their presentation was the strengthening of the Triangle of Care and carer-related PCREF oversight. They recognised that carer involvement cannot rely on goodwill or isolated champions; it requires structurally defined roles, written responsibilities, and consistent organisational expectations. The Trust is working on ensuring that every team and ward embeds a carer champion, whose purpose is not to “do everything for carers”, but to support cultural change within the workforce so that carers are recognised as equal partners.
They emphasised the importance of building staff capacity in cultural humility and safe conversations about race. AWP acknowledged that staff often feel unprepared to discuss ethnicity, discrimination or identity with carers. To address this, the Trust has created psychologically safe internal spaces, particularly for racially marginalised staff—to process experiences and explore how structural and interpersonal inequalities impact both staff wellbeing and patient care. This cultural environment is foundational to PCREF implementation because it shapes how confidently staff engage with diverse carers.
Key Points:
Carer champions must support, not replace, teams in working with carers.
Emphasis on psychological safety for racially marginalised staff and carers.
Encouraging honest conversations around race, trauma, and culture across staff teams.
Questions raised by attendees:
How do you embed cultural awareness within staff teams, not just for carers? – Concern that staff dynamics and cultural differences must be addressed to create consistent culturally responsive care.
How do staff and leaders hold ‘difficult conversations’ about race and safety? – Attendees wanted clarity on how psychological safety is practiced and how managers are supported.
🌟 2. Birmingham & Solihull Mental Health NHS FT
(Children & Young People’s Division – “Co-STARS” programme)
Birmingham & Solihull (CYP) presented one of the most detailed and emotionally grounded PCREF programmes, shaped heavily by lived-experience research with Black diaspora families. Their PCREF priorities, knowing our communities, transforming with communities, and delivering care that works reflect a commitment to embedding cultural responsiveness at every step. Their partnership with the University of Birmingham and Forward Thinking Birmingham has produced the Co-STARS project, a blend of lived-experience-led community work and staff training modules.
A major part of their PCREF advancement comes from working intensively with families to capture how racialised parents feel when using services. The Trust shared powerful testimonies from Black carers who described needing to “emotionally self-regulate” in meetings to avoid being labelled angry, unstable or cold. Parents also highlighted the emotional labour of protecting their children from stereotypes such as the “angry Black boy”, as well as fears of being adultified or dismissed. These insights have directly reshaped responses from clinical teams and informed the development of carers’ passports and safe spaces.
Birmingham & Solihull also emphasised building structures to ensure that their care pathways become culturally competent and adaptive. They are embedding PCREF champions across all clinical pathways, from eating disorders to psychosis and autism, ensuring diversity and inclusion principles shape every aspect of assessment, treatment and review. The Trust is also developing e-learning on culturally responsive practice, and expanding identity-specific support spaces (e.g., Black Carers Groups and new plans for Asian carers’ spaces). This multi-layered approach reflects a commitment to PCREF that is both structural and deeply relational.
Key Points:
Embedding culturally competent conversations within CYP teams.
Developing a Black Carers Group and safe spaces for racialised parent groups.
New e-learning on culturally responsive practice (from Co-STARS package).
Use of carer passports to ensure carers feel like equal partners.
Strong focus on how ethnic minority parents feel judged or misread by services (e.g., “angry Black woman,” “cold mother”) – themes drawn directly from carer focus groups.
Recognising adultification, stereotyping, and the emotional labour families perform.
Questions raised by attendees:
What about older adult Black communities? – Carers questioned how older Black adults, shaped by decades of racism, would be included in PCREF work.
Are you working with the police on cultural awareness? – Concerns around disproportionate use of Section 136 and stereotypes (e.g., assuming someone is “aggressive” because they speak loudly or gesture).
How will parent–carer voices shape service pathways and outcomes across all diagnoses (e.g., autism, psychosis)?
3. Sussex Partnership NHS Foundation Trust
Sussex Partnership presented PCREF as a three-pillared programme: data, co-production & engagement, and workforce development. Their first priority is improving ethnicity and protected characteristics data, which they acknowledged has historically been inconsistent. Sussex is launching a behavioural-change campaign that involves interviewing service users from minority backgrounds about why they may decline to share ethnicity, alongside staff interviews to understand documentation issues. Their goal is a transparent baseline from which meaningful PCREF action can be driven.
The Trust also described significant investment in a new data infrastructure via Power BI dashboards. These tools will pull together real-time information on areas such as restraint, Section 132 rights, and involuntary detention by ethnicity. The Trust stressed that PCREF cannot function without high-quality data because inequalities must be clearly visible and accessible to teams at every level—from ward managers to executive boards. Their future ambition is to enable quicker identification of disparities and faster interventions that prevent harm.
Sussex’s strongest focus was on building genuine co-production through their Expert Delivery Group (EDG). Unlike past approaches where community partners were only consulted, the EDG is designed as a collaborative decision-making space. Sussex acknowledged up front that phase 1 of PCREF planning did not fully embody equal partnership, and committed to ensuring that phase 2 will be co-produced from the ground up. The EDG will define what co-production means, co-design PCREF implementation plans, and shape updates that reflect community priorities, trust recovery, and anti-racist aspirations.
Key Points:
A behavioural-change campaign to improve ethnicity data recording (currently 65% compliance).
Development of Power BI dashboards for rapid inequality analysis.
Defining anti-racist and cultural competency skills for staff, tied to new EDI training.
Creation of the Expert Delivery Group (EDG) as a collaborative community–trust space.
Questions raised by attendees:
Is this “real” co-production or consultation? – Attendees challenged Sussex on whether the initial plan was created with the community or presented to them.
How will service users and carers hold equal power within co-production?
How will your anti-racism ambitions be demonstrated externally to communities? – Attendees expressed concerns that staff training alone does not reassure communities.
How will carers’ needs be embedded in PCREF (Triangle of Care)?
🌟 4. Kent & Medway Mental Health NHS Trust
Presenter:Kamellia (with contribution from Harriet – Lived Experience)
Kent & Medway showcased a comprehensive and governance-driven PCREF structure supported by their Equity for All Assurance Group. The Trust has embedded health inequalities into its broader strategy and is working to ensure that PCREF, protected characteristics data and health equity are woven into everyday practice. With the Trust’s newly updated name and identity, PCREF sits at the centre of a renewed commitment to equitable access, outcomes and patient experience across Kent and Medway.
Their PCREF progress includes delivering cultural competence training to 259 senior leaders, a significant investment in shifting leadership behaviour and expectations. They have also identified major data disparities in areas such as complaints, where ethnicity recording is only around 30%. To address this, they are rolling out the About Me form across their clinical system (Rio), which streamlines demographic and protected characteristics documentation for both carers and patients. This step is being supported by staff training designed to build confidence in discussing sensitive identity-related topics.
Kent & Medway also highlighted the expansion of their new Involvement & Engagement Team, which links directly with communities across East, West and North Kent. They are testing a Health Inequalities Toolkit, improving carer experience data collection, and creating new Family, Friends & Carers forms that capture protected characteristics, communication needs, and whether a carers pack was offered. The Trust’s approach is detailed, structural and long-term, aiming to embed PCREF as part of “business as usual” rather than a separate initiative.
Key Points:
259 senior leaders trained in cultural competence.
New About Me demographic/protected characteristics form launching trust-wide.
Major data gaps identified (e.g., only 30% ethnicity data for complaints).
New Involvement & Engagement Team connecting with community groups.
Testing the Health Inequalities Toolkit .
New Family, Friends & Carers Information Form including carer-pack tracking.
Questions raised by attendees:
Do you provide information in languages other than English? – Carers stressed that if translations don’t exist, PCREF is inaccessible from the start.
How will carers be supported to attend meetings given their unpredictable caring responsibilities?
How will you gather demographic data for carers when many do not have Rio records?
How will minority groups be reached in areas where the Trust’s population is overwhelmingly White British?
5. Carer Support Organisation (Kent & Medway Carers Support)
Presenter:Donna Green (involve Kent)
Key Points:
They run trust-wide carer experience groups and targeted workshops.
Emphasised difficulty for carers to attend meetings due to constant demands.
Highlighted the need for multiple approaches, including creative well-being sessions.
Closing Reflections from the Forum
I wrapped up the session acknowledging:
The strong desire across Trusts to improve PCREF delivery.
The pressure to progress quickly without losing sight of lived experience leadership.
The need to bring CQC into future meetings for transparency around expectations.
The importance of ethnic minority carers having a forum that values honesty over polished presentations.
Final Thoughts
This month’s forum demonstrated that while progress continues nationally, there remain shared challenges across NHS Mental HealthTrusts:
Recording ethnicity and protected characteristics meaningfully
Embedding anti-racism beyond training modules
Meeting the needs of Black, Asian and other racialised carers
Co-production that is real, not rhetorical
Involving carers whose time and emotional capacity are already stretched
Ensuring safety, trust and humanity in every interaction.
Above all, the session showed that ethnic minority carers are not passive observers they’re leading, questioning, shaping and insisting on accountability at every step.
By Matthew McKenzie, Facilitator, National Ethnic Mental Health Carer Forum
Introduction: A Forum that Connects and Challenges
As the facilitator of the National Ethnic Mental Health Carer Forum, I never take for granted how special these sessions are. Each month, carers, professionals, and researchers from all over the UK log in to share knowledge, raise awareness, and push for change in how mental health services understand and support ethnic minority communities.
Our October 2025 session was a powerful one. Falling on the last day of Black History Month, it brought together crucial themes on race equality, co-production, research, and carer visibility.
We heard from two key areas shaping mental health equity right now:
The OSMOSIS Project, led by Dr. Jacqueline Sin and Sharon Galliford, focusing on developing social care-based support for carers of people with psychosis.
The Patient and Carer Race Equality Framework (PCREF), presented by Aboobaker Bhana, Equality and Involvement Manager for South West Yorkshire Partnership NHS Foundation Trust.
by Matthew McKenzie – National Ethnic Mental Health Carer Forum Chair
In August, the online National Ethnic Mental Health Carer Forum came together once again to confront difficult but necessary conversations about systemic racism, discrimination, and the experiences of ethnic minority carers within health and social care. The forum, hosted by Matthew McKenzie, provided a platform for carers, professionals, and researchers to share insights, frustrations, and plans for change.
Focus on Racism and Discrimination
This month’s forum was unflinching in its focus: racism in health and mental health systems. Attendees shared powerful testimonies of racial abuse and discrimination, highlighting how these experiences undermine trust in services and affect both carers and those they support. There was a clear call for honesty – participants stressed the importance of naming racism directly, rather than disguising it behind euphemisms.
The group also discussed the overrepresentation of Black and brown people in prisons, the lack of tailored initiatives for older Black carers, and the persistent inequalities faced by ethnic minority families trying to navigate mental health and social care support.
Research and Evidence from Carers Trust
A key presentation came from Andrew of Carers Trust, who shared research into the barriers faced by Black, Asian, and minoritised ethnic carers. The findings highlighted widespread issues: discrimination, language barriers, lack of cultural competence, and difficulties in accessing benefits. Andrew emphasised the need for culturally inclusive services and stronger outreach strategies, while acknowledging feedback from the forum that research and advocacy must be explicit about racism rather than avoiding the term.
Andrew expanded on the importance of equity in benefit advice, pointing out that many carers miss out on their entitlements because information is inaccessible, overly complex, or not communicated in culturally relevant ways. He called for dedicated advice services that are not only multilingual but also sensitive to carers who may not self-identify as such.
He also spoke about the impact of social isolation on carers from ethnic minority backgrounds, who often have fewer support networks and face stigma within their own communities. Addressing this requires building trust with local organisations and ensuring carer support is visible in spaces where communities already gather, such as faith centres or community hubs.
Finally, Andrew outlined the Carers Trust’s national strategy, which involves working more closely with local carer organisations, producing research that amplifies marginalised voices, and lobbying for systemic reforms. He highlighted how this forum’s feedback directly shapes their advocacy, showing a real commitment to partnership.
Questions raised during Carers Trust’s presentation:
How can Carers Trust ensure its research explicitly names racism rather than using softer language?
What specific support can be offered to carers who do not self-identify as carers and miss out on benefits?
How can Carers Trust improve its complaints handling processes, particularly for carers facing racism and discrimination?
What role can MPs and lobbying groups play in supporting Carers Trust’s advocacy for ethnic minority carers?
How will Carers Trust ensure its multilingual materials are distributed widely enough to reach isolated communities?
Hampshire & Isle of Wight NHS Anti-Racism Initiatives
Usually NHS Mental Health trust representatives update on anti-racism initiatives at the forum. This time Hampshire and Isle of Wight engaged with minority carers.
Elton who is the Diversity and Inclusion Partner from Hampshire and Isle of Wight NHS Trust provided an update on their anti-racist programmes, including the rollout of the Patient and Carer Race Equality Framework (PCREF). The trust has begun implementing cultural competence training, engaging with local communities, and embedding anti-racism into its wider mental health services. While early in its journey, the trust is already seeing changes in communication and engagement across different wards and services.
Elton shared that the trust is actively developing training modules on implicit bias, with the aim of reaching every staff member across its services. This training is intended not as a one-off exercise but as part of a sustained culture change programme. Early feedback from staff has been encouraging, with more frontline workers recognising how unconscious bias can influence treatment decisions.
He also described the trust’s efforts to engage directly with service users and carers, ensuring that their lived experiences feed into decision-making. Listening events, surveys, and advisory panels are being used to capture diverse perspectives, with a particular focus on groups who historically felt excluded from consultation.
In addition, Elton emphasised the need for transparency and accountability. The trust will publish regular updates on its PCREF action plan, allowing communities and stakeholders to scrutinise progress. He acknowledged that this is just the beginning, but stressed that embedding anti-racism into healthcare systems requires openness, humility, and sustained commitment.
Participants raised questions about how these initiatives address specific groups, such as older Black carers and prisoners’ families, as well as concerns about public misconceptions of anti-racism work. Elton acknowledged these challenges and committed to following up with colleagues on gaps raised during the discussion.
Questions raised during NHS Trust’s presentation:
How will PCREF specifically address the needs of older Black adults who often feel invisible in services?
What is being done to support the mental health of prisoners (e.g. Albany and Parkhurst prisons) and their families within this anti-racist framework?
How will the trust prevent the public misconception that PCREF “excludes” white people?
What mechanisms are in place to ensure transparency and accountability in publishing progress updates?
How will the trust measure the long-term impact of cultural competence and implicit bias training?
Academic Research Contributions
The forum also heard from Shylet, a PhD researcher from University of Glasgow, who is focusing on learning disabilities. She presented her work on the lived experiences of Black African families caring for adults with learning disabilities, and invited participants to take part in interviews. Their contributions highlighted the importance of academic research in documenting and amplifying carers’ lived realities.
Another important theme was the financial challenges facing carers. The group discussed the complexity of benefits like Carer’s Allowance and how misinformation or fear of losing other entitlements often deters carers from claiming support. A carer expressed reluctance to claim due to concerns about how it might affect their relative’s benefits, while another highlighted the importance of valuing one’s own contribution and recognising caring work. There was frustration with bureaucratic systems that seem designed to exclude, particularly when layered with the additional barriers of language, culture, and discrimination.
Carers also highlighted the immense value of unpaid care, with estimates placing its worth at over £180 billion per year if it were to be paid for by the NHS. This figure underscored the urgent need for better recognition and support of carers’ contributions.
Strengthening Complaints and Accountability
There was a debate around how carers can raise complaints when faced with racism or poor treatment. Many participants expressed a lack of trust in formal systems like the CQC or Ombudsman, feeling that complaints disappear into bureaucracy without change. Suggestions included working with MPs, lobbying groups, or the media to ensure voices are heard.
Final Reflections
The August forum showed once again how necessary it is to hold these difficult conversations. Carers spoke bravely about racism and exclusion, professionals shared updates on anti-racist strategies, and researchers sought to bring lived experience into policy. Yet the message was clear: systemic change requires more than frameworks and research reports. It requires honesty, collaboration, and persistence.
As host, I was encouraged by the passion and determination in the room. The forum continues to grow as a national voice for ethnic minority carers, and our commitment to addressing racism head-on remains at the heart of this work.