The poem is a spoken word piece from my upcoming poetry collection Unpaid, Unseen and Yet Unbroken (launching 2026).
This poem centres the lived experiences of ethnic and minority mental health carers, where they continue to show up, often without recognition, navigating systems that can feel complex and unresponsive.
The poem focuses on the quiet strength, shared knowledge, and collective care that exist within our communities.
In the spirit of PCREF, this work highlights the importance of listening to lived experience, valuing cultural understanding, and recognising community as a source of resilience and healing
I chaired our March hospital discharge network meeting with a real sense of momentum building across the system. What continues to strike me is the mix of voices in the room, commissioners, carers centres, hospital representatives, and grassroots advocates all trying to tackle the same persistent issue: how we properly involve and support unpaid carers during and after hospital discharge.
As someone with lived experience, particularly in mental health and complex care, I always come back to one key question: Are carers being treated as partners, or are they still being treated as visitors?
This meeting gave us a very honest answer progress is happening, but there is still a long way to go.
Key Presentation: Derbyshire HConnect Project
Emma’s presentation was, for me, an important part of the meeting not because it introduced something completely new, but because it clearly articulated what many carers have been saying for years, and then actually did something about it.
What stood out immediately was that this wasn’t a project designed in isolation. It was built directly from carer voice and lived experience. The starting point wasn’t “how do we improve discharge?” it was “what are carers actually experiencing right now?”
And what carers described was difficult to hear, but not surprising.
Carers spoke about not being recognised at all. Some said no one had even asked if they were a carer. Others described situations where their knowledge of the person they care for was ignored, even when it was critical. One example that stayed with me was a carer describing their loved one being discharged in the middle of winter, late at night, without proper clothing or preparation.
There was a consistent feeling that once someone enters hospital, the carer’s role is almost paused or worse, dismissed entirely.
What the HConnect project does differently is acknowledge that this isn’t just a communication issue it’s a system and culture issue.
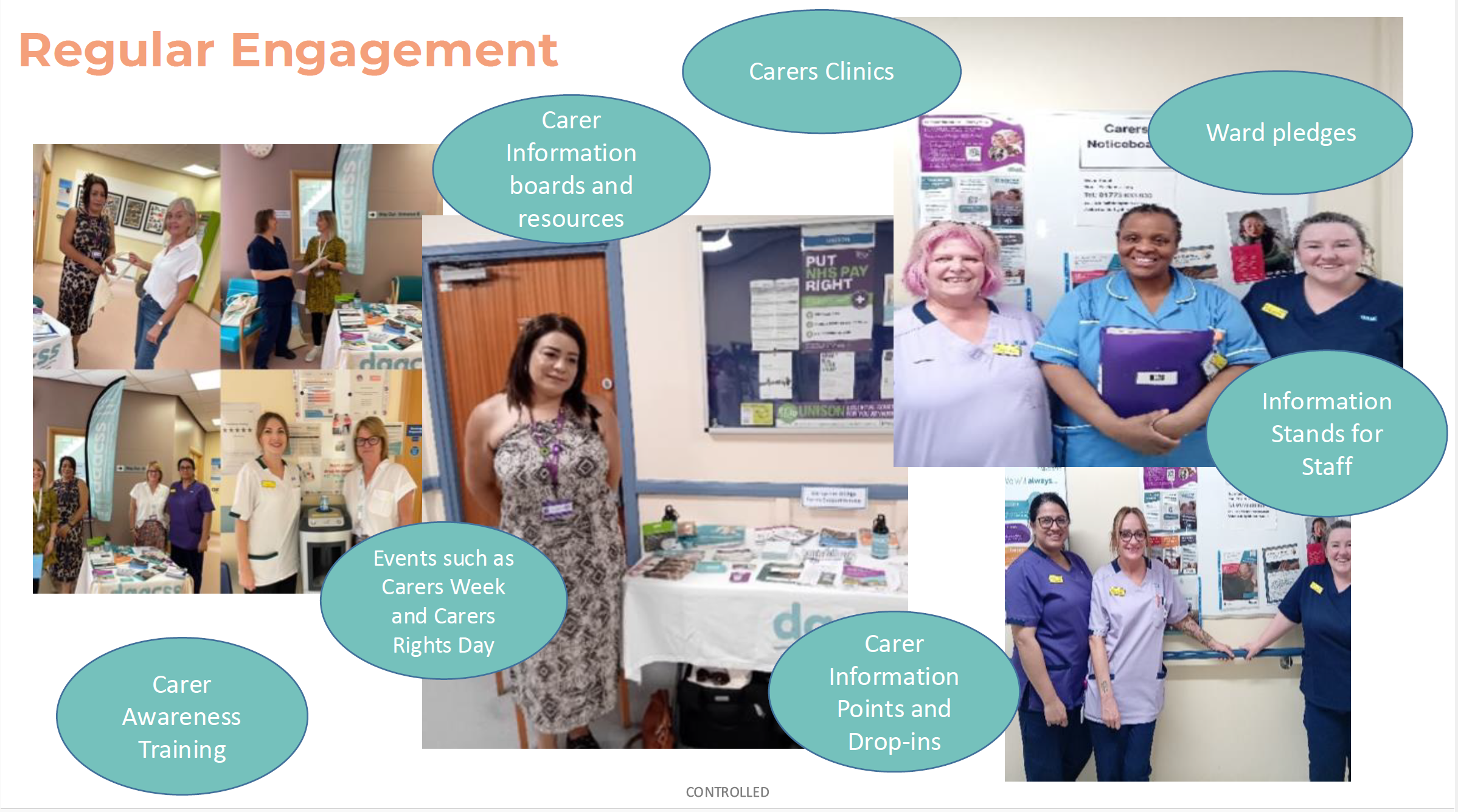
Instead of relying on one intervention, the model works across multiple layers of the hospital system. It introduces dedicated hospital liaison workers who build relationships with wards, while also ensuring carers themselves are visible and supported directly on-site. At the same time, it invests in staff through training, guidance, and practical tools so that engaging carers becomes part of everyday practice rather than an optional extra.
What I found particularly important is that the project doesn’t assume staff are unwilling—it recognises that many staff simply lack the confidence, knowledge, or structure to engage carers properly. In fact, the findings showed that many hospital teams had never received any formal carer awareness training and were often unaware that carers even have a legal right to be involved in discharge planning.
The research element of the project adds another layer of depth. Through interviews with carers, several consistent themes emerged.
Carers described feeling invisible—treated as visitors rather than partners in care. They talked about their expertise being dismissed, even when they knew the patient best. Communication was often unclear or inconsistent, and discharge frequently felt rushed, with little notice or preparation. In many cases, carers ended up acting as the safety net catching mistakes, coordinating care, and managing complex needs on their own once the person returned home.
What struck me most is that these issues aren’t just isolated incidents they are patterns.
But importantly, the presentation didn’t just focus on what’s going wrong. It also highlighted what good looks like. In situations where carers were listened to, involved early, and treated as equal partners, the entire experience changed for both the carer and the patient. The challenge now is making that level of practice consistent, not exceptional.
The project is already showing tangible impact. There has been a noticeable increase in carers being identified within hospital settings, more referrals coming directly from health professionals, and hundreds of carers receiving support through the programme.
For me, the biggest takeaway from this presentation is this:
This isn’t about adding more services it’s about changing behaviour across the system.
The HConnect model recognises that for carers to be properly involved, three things need to be in place: staff need the capability to identify carers, the opportunity within the system to engage them, and the motivation to see this as a core part of care. Without all three, change simply won’t stick.
And that’s why this work matters. Because until carers are consistently seen, heard, and included, we will continue to see the same issues repeating no matter how many initiatives we introduce.
Lewisham Commissioner Update
From Lewisham’s commissioning side, there were some strong practical developments.
A key initiative is the rollout of a carer welcome pack, designed to be:
Clearly visible in hospital settings
Easily accessible to carers at the point of need
This is being strengthened through:
Increased collaboration with hospital staff
Plans to expand distribution across wards
From Lewisham, we also received a really significant update around system-level change, particularly the development of a Standard Operating Procedure (SOP) for engaging unpaid carers in hospital settings.
This work has been led across South East London ICB, with an external partner supporting the design. The aim of the SOP is to provide:
Clear guidance to hospital wards
Practical prompts and questions for staff
A consistent approach to identifying and engaging carers during hospital stays
What stood out to me is that this isn’t just a document, it’s designed to change behaviour on the ground. It focuses on something simple but powerful: how staff start conversations with carers and recognise the people already supporting patients.
In Lewisham, University Hospital Lewisham was selected as one of the pilot sites, with two wards testing the approach. The next stage is particularly important:
The SOP is being embedded into Trust templates
It is due to be presented to the Trust board for formal approval
There are plans to roll this out across Lewisham and Greenwich NHS Trust, including Queen Elizabeth Hospital (Woolwich)
What I found especially encouraging is that carers have been involved throughout:
Input gathered through workshops
Further feedback taken to the Lewisham Council’s Open Carers Forum
Ongoing opportunity for boroughs to adapt the SOP to local needs
Alongside this, Lewisham is continuing practical work on the ground:
Strengthening links between commissioned carers services and hospital staff
Expanding visibility through carer welcome packs and information points within the hospital
For me, this is one of the most important developments discussed in the meeting. If implemented properly, a shared SOP like this has the potential to:
Reduce inconsistency across wards
Embed carer identification into everyday practice
Move us closer to a system where carers are routinely recognised—not accidentally discovered
Hospital Update: Lewisham & Greenwich NHS Trust
A really important contribution came from the patient experience perspective at Lewisham and Greenwich NHS Trust, which covers University Hospital Lewisham and Queen Elizabeth Hospital (Woolwich).
From the Trust side, there was clear recognition that:
The work carers are doing is valuable and essential to patient outcomes
There is a need to improve physical visibility of carer support within hospital settings
Space and infrastructure need to better support engagement (for example, identifying a permanent location for carer engagement and resources)
There was also a willingness to:
Explore how carer-led engagement (including my own involvement) can be better embedded within the hospital environment
Strengthen links between patient experience teams and carers organisations
From my perspective, this was a positive and practical discussion. Too often we talk about engagement in theory—but here we were talking about where the table actually goes on the ward, and that level of detail matters.
Because if carers can’t see you, they can’t access you.
Greenwich (Commissioning & Mental Health)
Greenwich colleagues spoke about their broader system approach, particularly within mental health.
Their focus includes:
Identifying gaps in carer support across services
Embedding carers within commissioning priorities
Understanding what carers themselves want from local systems
They also posed an important question to the group: What should local authorities prioritise for carers?
My answer was straightforward: We need clear leadership and accountability, a named person or role responsible for carers across the system.
Without that, good work risks becoming fragmented.
Lambeth Carers Hub (King’s College Hospital & St Thomas’ Hospital)
Lambeth shared a detailed and honest update regarding their work across King’s College Hospital and Guys and St Thomas Hospital
Key points included:
Their hospital discharge project is continuing, but with reduced capacity due to funding constraints
They have secured a short-term extension, allowing work to continue until September
A major focus is now embedding carer awareness training into staff induction processes
Importantly, they raised a systemic issue:
The need to hold commissioned care agencies accountable, particularly when carers report poor-quality care after discharge
This is critical. Discharge doesn’t end at the hospital door—if the care package fails, the whole system fails.
Southwark Council Update
From Southwark, we heard about work being done at a system level, particularly linked to:
Development of discharge information resources across South East London
Collaboration across boroughs and NHS partners
The intention is for these resources to be:
Widely accessible and adaptable
Used across multiple organisations, rather than siloed locally
Given the proximity to major hospitals like King’s College Hospital and GSTT hosptal, this kind of coordinated approach is essential.
City & Hackney Carers Centre (Homerton Hospital)
A more concerning update came from City & Hackney, particularly regarding work linked to Homerton Hospital.
They reported:
The loss of a hospital discharge worker role
A significant drop in referrals to the carers centre as a result
Reduced presence within the hospital environment
This clearly demonstrates something we often say but don’t always quantify:
When you remove dedicated roles, you remove outcomes.
The worker’s presence had been directly contributing to engagement and referrals. Without that, carers are once again at risk of being missed.
Richmond Carers Centre (Kingston Hospital)
Updates from Richmond Carers Centre highlighted both strong engagement and opportunities to build further.
Positives:
Strong referral pathways coming through from Kingston Hospital, particularly linked to discharge activity
Ongoing professional awareness work, helping improve understanding of carers across services
There is a clear foundation here, with established relationships already supporting carers into services. The opportunity now is to build on that by increasing visibility and strengthening in-hospital engagement further.
Richmond Borough Mind (Springfield Hospital – SWLSTG)
From Richmond Borough Mind, the focus was more specifically on their work within South West London and St George’s Mental Health Trust (SWLSTG), particularly at Springfield Hospital.
Key challenges highlighted:
Difficulty accessing wards within Springfield Hospital, limiting direct engagement with carers
Limited contact with carers when based in general hospital areas rather than embedded on wards
Ongoing challenge in identifying where carers are most visible and reachable within mental health settings
What came through strongly is that, despite proactive efforts such as setting up stands and being present on-site, footfall from carers remains low unless services are embedded directly into ward environments.
This reinforces a key point for me:
In mental health settings especially, access is everything—if you’re not where carers are, you simply won’t reach them.
Bexley Carers (Post-Discharge & Reablement Focus)
Bexley brought an important perspective that often gets overlooked what happens after discharge.
Their work is focusing on:
Supporting carers once reablement packages end
Recognising that carers often deprioritise themselves during discharge, only to struggle later
Increasing concern around safeguarding and mental health, particularly in dementia care
This is where we need to shift thinking: Discharge is not the endpoint—it’s the start of a new phase of care.
Cross-Cutting Reflections
Across all updates, several consistent themes emerged:
Inconsistent carer identification across wards and trusts
Funding fragility, with projects often short-term
Need for embedded training, not optional sessions
Importance of visibility within hospital environments
Gaps in post-discharge support, especially after reablement
My Closing Thoughts
Chairing this meeting, I was struck by both the progress and the gaps.
There is innovation happening in Derbyshire, in Lambeth, in Lewisham, across South East London. But it’s uneven. And carers feel that inconsistency every day.
For me, the priority remains clear:
Identify carers early
Involve them properly
Support them beyond discharge
Because when we get that right, everything else improves—outcomes, safety, and experience.
And until we get that right consistently, we still have work to do.
This week as of this blog post, the London Assembly published a major new report on unpaid carers: “London’s unpaid carers: Caring for the carers.”
I had the opportunity to contribute to this work as a carer and advocate, alongside others who shared their lived experience. Seeing those voices reflected in the final report is both encouraging and a reminder of how much still needs to change for unpaid carers in London.
One of the strongest messages in the report is that many unpaid carers are still not identified.
Too often, people caring for a partner, parent, or child don’t even realise they are classed as a “carer” which means they miss out on financial support, services, and basic recognition.
From my own experience, and what was shared at the Assembly, this is especially true for:
Mental health carers
Carers from ethnic minority backgrounds
Indentification of unpaid carers
If you’re not identified, I feel you don’t exist in the system.
Financial pressure is a major issue
The report possibly confirms what many carers already know:
Nearly 1 in 3 carers in London are living in poverty
Carer’s Allowance is not enough to live on
Many carers have to reduce work or leave employment entirely
There are positive recommendations here like reviewing Carer’s Allowance and reducing travel costs, but these need to turn into real change, not just policy discussions.
Support isn’t working as it should
Another issue raised in the report and something I spoke about is that support often feels like a “tick-box exercise”.
Carers go through assessments, but:
Support is limited
Funding is inconsistent
Real help (like respite care) is hard to access, especially for mental health carers, I mean what does respite actually mean for mental health unpaid carers?
Identification alone isn’t enough. I think It has to lead to meaningful, practical support.
So what needs to happen next?
The report makes some important recommendations:
Better identification of carers across London
More funding for local carer services
Changes to Carer’s Allowance
Improved workplace support
and a lot more, but you would have to go through the report.
But the key question now is: will this actually be implemented?
Carers don’t need more recognition alone we need action.
Final thoughts
Unpaid carers are holding up the health and social care system every single day.
This report is a very important step forward. But it should be the beginning of change not the end of the conversation.
If you are a carer, or know someone who is, I’d encourage you to read the report and share your experiences. The more visible carers are, the harder it is for the system to ignore us.
On 25th February 2026, I had the privilege of speaking at the Carers’ Forum hosted by Involve Kent.
Involve is a voluntary sector infrastructure organisation in Kent that supports unpaid carers by providing information, advice and practical help to make caring more manageable.
They organise regular carers’ forums and events where carers can meet each other, access specialist support services, hear from guest speakers on issues like benefits, legal rights and wellbeing, and contribute their lived experience to local planning and decision-making. Involve also connects carers with tailored resources, signposts to relevant services across health, social care and community sectors, and advocates for carers’ voices to be heard by policymakers and service providers
The forum ran from 10:30am to 1:30pm and brought together unpaid carers from across Kent to connect, learn and have their voices heard.
It was my second time speaking at this forum, and once again I was struck by something powerful: the room was full. That might sound simple, but in the world of unpaid caring which can often feel isolating and invisible a full room means solidarity. It means people are choosing, despite exhaustion and competing demands, to show up for themselves and each other.
Arriving and the atmosphere
From the moment I walked in, there was a real sense of warmth. Information stands lined the hall Involve, Citizens Advice, mental health services, energy advice, leisure services and more. Tables were covered in leaflets, conversations were already flowing, and carers were reconnecting with familiar faces.
The purpose of the forum was clear:
To enable those caring unpaid for an adult family member, partner or friend to meet, gain information about services in their community and have their voices heard .
That last part to have their voices heard is what resonated most with me.
It was also good to see Carer leads from Cygnet Maidstone engaging with carers in the community of Kent.
My talk: Caring for someone with a mental health diagnosis
I spoke about caring for someone with a mental health diagnosis and the Patient and Carer Race Equality Framework .
As many know, I cared for my mother who lived with schizophrenia, and I now support a close friend who lives with personality disorder and addiction challenges. I don’t speak as a clinician. I spoke as someone who has sat in GP waiting rooms, on inpatient wards, in crisis meetings, and at home during those “screaming silences” that carers know too well.
I shared:
The confusion I felt when I didn’t even realise I was a “carer”
The frustration of confidentiality barriers
The loneliness of not being listened to
The emotional exhaustion that comes from constantly firefighting crises
I then shared a poem to promote carers rights
But I also shared something equally important: growth, advocacy and solidarity.
I encouraged carers to:
Educate themselves about the condition they are supporting
Learn the difference between symptoms and personality
Understand triggers
Forgive themselves for mistakes
And most importantly, look after their own wellbeing
One message I always return to was – You cannot pour from an empty cup.
I also spoke about The Patient Carer Race Equality Framework
It exists because there is clear evidence of:
Disproportionate detentions under the Mental Health Act
Poorer outcomes for Black and minority ethnic patients
Higher levels of distrust between communities and services
Carers feeling unheard or excluded
I spoke about how minority carers can face:
Cultural misunderstandings
Language barriers
Stigma around mental health within communities
Fear of services due to past discrimination
A lack of culturally appropriate support
Discussion tables: Carers influencing change
After my talk, Clara from Involve led discussions feeding into Kent’s Health Needs Assessment for carers. Carers were asked:
How do you recognise when it’s time to ask for help?
What causes burnout?
What would a carer-friendly community look like?
These wete not token questions. Staff took notes (without identifying details) so carers’ lived experiences could directly inform local planning .
I moved around the room speaking with carers. Some were open and vocal. Others were quieter, but their listening was just as powerful. Not everyone wants to speak publicly and that’s okay. Being present is also participation too.
Power of Attorney – protecting your voice
Later in the morning, Glen Miles spoke about the Mental Capacity Act and Lasting Power of Attorney .
As carers, we often assume we will automatically be consulted in crises. The reality is different. Without legal authority, our ability to advocate can be limited.
One key takeaway:
Don’t delay in arranging Lasting Powers of Attorney.
If you want your voice – or your loved one’s voice – to be heard, formalise it.
For carers who have experienced being excluded from decisions, this was a particularly important session.
Citizens Advice & practical support
Ian from Citizens Advice spoke before lunch about benefits, debt, housing and confidential support .
With the cost of living crisis, carers are under immense financial pressure. Many reduce employment hours or leave work entirely. The session was a reminder that:
Advice is free
It is confidential
You can attend anonymously
You are not judged
Lunch followed – catered by Fusion – and honestly, some of the most meaningful conversations happen over sandwiches. Carers swapping stories. Sharing phone numbers. Recommending services. That peer-to-peer support is priceless.
What stayed with me
What stayed with me most wasn’t just the agenda or the presentations.
It was:
The older carer quietly nodding as I spoke about emotional exhaustion.
The new carer asking, “Is it normal to feel this angry sometimes?”
The male carers who stayed behind to speak to me privately.
The carers from minority backgrounds who spoke about cultural barriers and stigma.
These forums matter because carers matter.
Unpaid carers save the system billions. But beyond economics, we hold families together. We absorb crises. We advocate in rooms where we’re not always welcomed.
If you’re an unpaid carer in Southwark, chances are you’re used to putting everyone else first. You support a loved one day in, day out, emotionally, practically, often invisibly. And too often, decisions about “support” for carers are made without carers truly being heard.
Southwark Council is developing its Unpaid Carers Strategy, and they are inviting unpaid carers to take part in upcoming focus groups to share real experiences, which are your lived reality.
As an unpaid carer myself, I know how rare and valuable this opportunity is.
Why having your say is important because
Policies and strategies shape:
What support is available
How easy (or hard) it is to access help
Whether carers feel recognised, supported, and understood
When carers don’t speak up, systems are built around us, not with us. When we do speak up, its a chance to make change becomes possible.
This isn’t about complaining. It’s about being honest: what works, what doesn’t, and what would genuinely make life easier for carers in Southwark.
Your voice could help shape:
Better access to information and services
More flexible, carer-friendly support
A strategy that reflects the real pressures carers face
A safe, non-judgemental space
One of the most important things about these focus groups is that they are designed to be:
Non-judgemental
Inclusive
Open to carers with any level of responsibility
You don’t need to have all the answers. You don’t need to be an “expert”. You just need your experience.
Whether you care full-time, part-time, occasionally, or don’t even label yourself as a “carer” your perspective still counts.
Focus group dates and details
In-person focus groups 📅 24th February ⏰ 11am – 1pmand2pm – 4pm 📍 Harriet Hardy Community Centre Harriet-Hardy Building, Aylesbury Estate, Albany Road, Walworth SE5 0AH
Online focus group 📅 25th February ⏰ 7pm 💻 Virtual session via Microsoft Teams
How to get involved
You can:
Scan the QR code on the flyer shown above my blog to register your interest
By Matthew McKenzie, A Caring Mind (Carers UK Ambassador)
As an unpaid mental health carer, I have spent years navigating hospital corridors, GP practices, care plans, juggling crises, and long silences where carers are too often left out. I am sure unpaid carers are expected to hold families together, while notice early warning signs, and keep loved ones safe. Still I always mention most of us receive no formal training, and our knowledge is rarely recognised as expertise.
That is why recently teaching a module for the Masters course to mental health nursing students at King’s College London felt so important. Not after they qualify. Not once they are overwhelmed in practice. But before they step out into the field. The session took place 15th of January.
Why carer-led teaching matters
Unpaid carers sit at the sharp edge of the mental health system. We see what works, what harms, and what gets missed when professionals don’t fully understand the family context. When students hear directly from carers, learning moves beyond textbooks into real life into the emotional, practical, and ethical realities of care.
Training mental health professionals without carer voices is like teaching navigation without a map.
What I taught: lived experience as learning
The session I delivered was built entirely from a carer’s perspective and centred on one core message: you cannot deliver effective mental health care without working with carers.
The module covered:
My lived experience as an unpaid mental health carer How I became a carer, the emotional impact, the daily responsibilities, and the toll caring can take on mental and physical health.
The hidden impact on carers Burnout, stigma, isolation, guilt, and the reality that many carers are supporting professionals while receiving little support themselves.
Carers as partners, not problems Exploring what happens when carers are ignored – and how outcomes improve when they are listened to, informed, and included.
The Triangle of Care A strong emphasis on the Triangle of Care framework: the partnership between service user, carer, and professional. I challenged students to see carers as a vital link in the chain, not an optional extra.
Carers UK and carer identification Highlighting the role of Carers UK in advocacy, rights, resources, and why professionals must help carers identify themselves early so they can access support.
Practical skills for future nurses Listening without defensiveness, sharing information appropriately, involving carers in care planning, and understanding when carers need support themselves.
Interactive discussion and reflection Students worked through real-life scenarios, asking: What would I do differently now that I understand the carer experience?
The shift we need in education
Most unpaid carers are not trained for their role. We learn through crisis, exhaustion, and trial and error. Mental health professionals, however, are trained, which means universities have a responsibility to ensure that training includes those of us living this reality every day.
Carer-led teaching builds empathy, improves communication, and ultimately leads to safer, more effective care. When students learn early that carers matter, they carry that mindset into practice.
A final thought
Unpaid carers are already part of the mental health workforce, it’s just the title unpaid, unsupported, and often unheard. So I feel bringing carers into universities is not a “nice extra”. It is absolutely essential.
If we want a mental health system that truly works, we must start by listening to those who never clock off.
I’ve spoken at many events over the years, but standing in a room full of carers always is a great experince differently. The room filled with lived experience, this time paid and unpaid carers carrying invisible weight of caring stories that rarely get space.
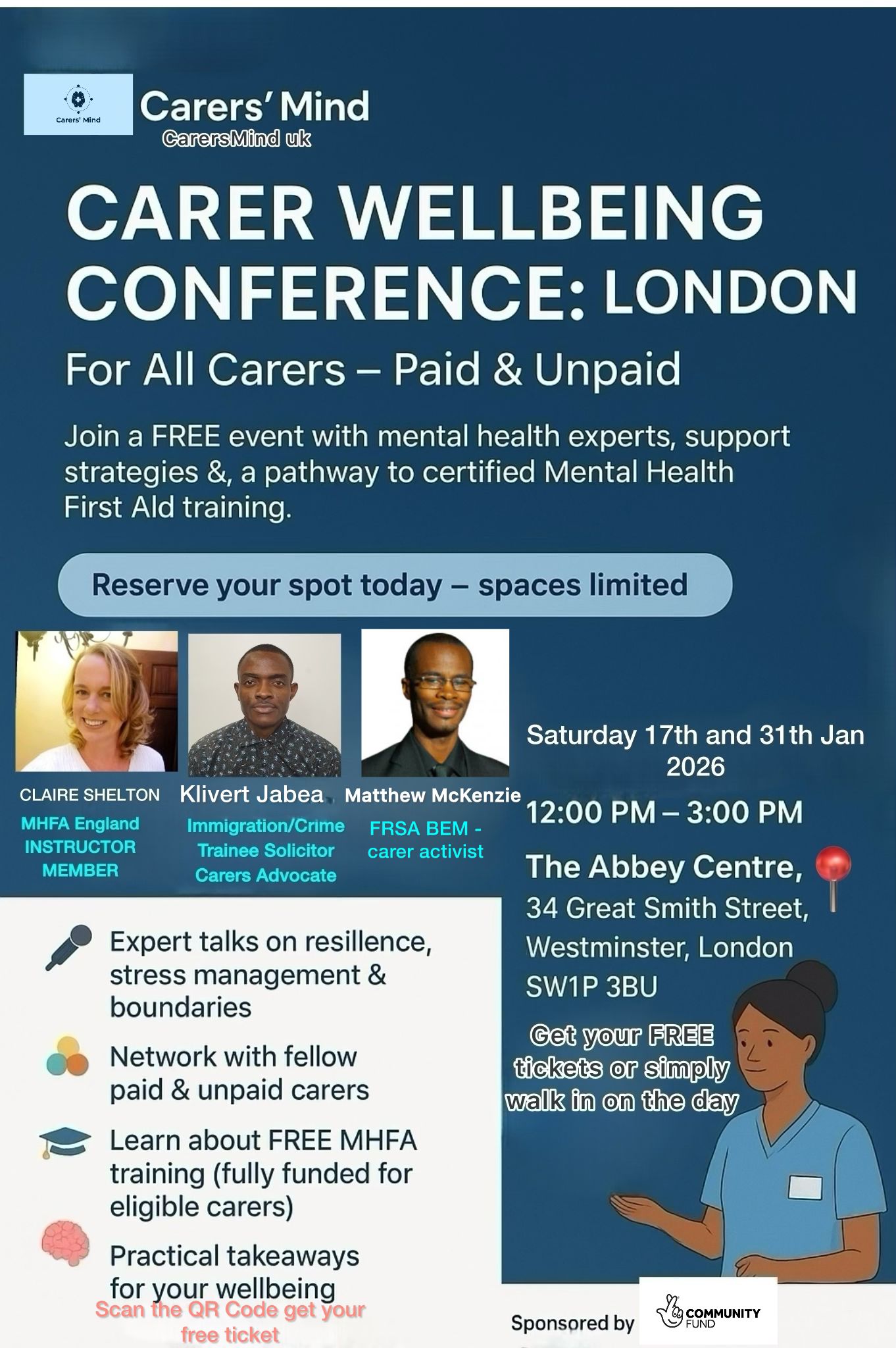
The Carers’ Wellbeing Conference in London, organised by Carers’ Mind CIC, was a moment where carers were allowed to be people first.
The event was hosted at The Abbey Centre, a welcoming community venue in Westminster that provides vital space for local groups, charities, and events focused on wellbeing, inclusion, and social support.
CarersMind CIC is a community-interest organisation dedicated to improving the wellbeing, visibility, and support of both paid and unpaid carers. Through accessible events, practical training, and open conversations about mental health, CarersMind CIC creates safe spaces where carers are recognised as individuals
The Impact of Caring on Mental Health
When I was invited to speak about “The Impact of Caring on Mental Health and What Actually Helps”, I didn’t hesitate. Caring has shaped every part of my adult life. It has taught me empathy, patience, advocacy, but it has also exposed me to burnout, trauma, guilt, and long stretches of isolation.
Too often, carers are spoken about rather than with. This conference made a conscious effort to centre carers’ voices, not as an afterthought, but as expertise.
The Room Told Its Own Story
At the conference, there was no pressure to “cope better” or “be more resilient” without acknowledging the cost. Instead, there was honesty.
Carers spoke about:
Burnout that creeps in quietly
Guilt for needing rest
The emotional toll of long-term responsibility
Feeling unseen by systems that rely on them
These were truths that deserved to be heard without judgement.
What Claire Shelton Shared at her session
Claire spoke openly about how caring impacts mental health carers over time, not just during moments of crisis. she talked about trauma that doesn’t announce itself, about stress containers that overflow slowly, and about how carers often normalise distress because “there’s no other option.”
Most importantly, she focused on what actually helps:
Being recognised as a carer both formally and emotionally
Access to peer support, not just professional services
Practical tools that reduce isolation
Boundaries that protect carers’ wellbeing without guilt
One resource Claire highlighted was the Hub of Hope, because carers need access to support that doesn’t require jumping through endless hoops. These matter not because they fix everything, but because they return a small amount of control to people who’ve lost a lot of it.
What I Shared in my session
In my session, I spoke from lived experience about the long-term impact of caring, shaped deeply by my role as a carer for my mother. I shared how caring is rarely defined by single moments of crisis, but by the gradual, cumulative pressure that builds over time. This includes the emotional labour, the constant vigilance, and the way stress and trauma often go unrecognised because caring simply becomes “what you do.”
I reflected on how caring for my mother affected my mental health, identity, and sense of self. This experience led me to speak about carers’ rights the right to be recognised as a carer, to be involved in decisions, to access support, and to protect one’s own wellbeing without guilt or fear of judgement.
Most importantly, I focused on what actually helps:
Being identified and recognised as a carer, both formally and emotionally
Understanding and exercising carers’ rights
Access to peer support grounded in shared lived experience, not only professional services
Practical tools that reduce isolation and complexity
The Power of Being in the Same Room
One of the most powerful moments wasn’t during my talk it was during the conversations that followed. Carers sharing strategies with each other. Nodding in recognition. Saying, “I thought it was just me.”
That’s the quiet power of events like this. They remind carers that their experiences are valid, shared, and worthy of space.
A Collective Effort
It was a privilege to share the day with:
Claire Shelton, who spoke with clarity and compassion about resilience, stress management, and boundaries
Klivert Jabea, who brought warmth, insight, and a strong message that self-care is not a luxury
The organisers at Carers’ Mind CIC, who created an environment that felt safe, inclusive, and genuinely carer-focused
This conference was about acknowledging reality and that’s where real wellbeing work begins.
Leaving with Hope and Responsibility
I left the Abbey Centre reminded of why this work matters. Carers are holding together families, communities, and systems often at great personal cost. Supporting carers isn’t optional. It’s essential.
Resources and Support for Carers
If you are a carer and are looking for support for your wellbeing, mental health, or caring role, the following resources were highlighted or reflected in discussions during the conference:
Hub of Hope — https://hubofhope.co.uk A free, UK-wide mental health support database that helps carers find local and national services quickly, without needing to navigate complex systems. It is particularly useful for carers who may not know where to start or who feel overwhelmed by traditional referral pathways.
CarersMind CIC — https://carersmind.co.uk/ A community interest company focused on improving carers’ mental health and wellbeing through events, training, and open conversations that centre lived experience. Their work creates spaces where carers feel recognised, heard, and supported.
Carers UK — https://www.carersuk.org/ Provides information on carers’ rights, benefits, assessments, and practical guidance for unpaid carers across the UK.
NHS Carers Support Local NHS and local authority carers services can offer carers’ assessments, signposting, and practical support. Availability varies by area, but carers have a right to request an assessment.
By Matthew McKenzie, facilitator of National ethnic mental health carers forum
Welcome to my first blog for 2026.
I am working on a new poetry project linked to my forum and poetry groups. This poem turned into song is written from the perspective of an unpaid ethnic mental health carer, and explores identity, pride, self-worth, and refusing shame in systems that don’t always listen or recognise lived experience.
The poem is taken from my forthcoming poetry book in development, Unpaid, Unseen and Yet Unbroken (due 2026), which centres the voices of ethnic mental health carers and aligns closely with the aims of PCREF (Patient and Carer Race Equality Framework), particularly around listening, inclusion, and lived experience shaping systems.
I’m using poetry and creative formats as another way to:
amplify carer voices
explore race and care with honesty
support conversations about equity, culture, and confidence in mental health services
If this resonates with your work, community, or organisation, please feel free to share. Listening is an act of care.
Matthew McKenzie FRSA BEM, poet and advocate for unpaid ethnic mental health carers, is inviting carers involved in NHS Trusts, PCREF (Patient and Carer Race Equality Framework), and Trust involvement registers to submit their poems for an upcoming 2026 poetry collection. This collection will spotlight minority carers’ voices and explore themes of race, culture, and lived experience in mental health care.
About the Poetry Collection
The collection will focus on amplifying minority carers’ experiences through poetry. It will be part of the paperback version of Matthew’s upcoming poetry book Unpaid, Unseen and Yet Unbroken and will include poems from carers all over the country. This is a unique opportunity for minority ethnic carers to have their voices heard and their stories shared on a national platform, contributing to the ongoing conversation about race equality, care, and mental health.
Why Should You Submit a Poem?
If you’re a minority carer or carers from underrepresented community, your voice matters. PCREF is committed to creating systemic change, and this collection will work alongside it to ensure that carers from minority communities are not left unheard. Submitting your poem gives you the chance to:
Raise awareness of the emotional, cultural, and psychological realities of being a carer.
Inspire others by sharing your lived experience.
Amplify minority voices within NHS Trusts, PCREF spaces, and mental health care systems.
Who Can Submit?
We welcome submissions from unpaid ethnic mental health carers who are:
Involved in NHS Trusts, PCREF, or trust involvement registers.
Attending ethnic mental health carer peer groups at carer centres
Interested in sharing their personal experiences and reflections through poetry.
How to Submit Your Poem:
Submit an original poem that reflects the emotional, cultural, and psychological realities of being an unpaid mental health carer.
Poems can focus on themes such as:
Emotional challenges of care
The hidden burden of caring
Resilience and survival
Navigating mental health services
Coping with racial and cultural barriers in care
Family dynamics in caregiving
Deadline for submissions is late April 2026.
Submission Guidelines:
Format: Poems can be submitted in Word, PDF, or plain text format.
Length: There is no strict length, but we recommend that submissions be no longer than 1 page.
Multiple submissions: You can submit more than one poem if desired.
Contact Information: Please include your full name, contact details along with your poem, so i can credit you. Unless you wish to be anonymous.
You can also reach out to Matthew directly if you have any questions about the submission process or the collection.
What Happens After You Submit?
Once submissions are received, I will review all entries and select poems that align with the themes of the collection. All selected poets will be notified and credited in the final publication.
Need Inspiration or Support?
If you’re unsure where to start or need some encouragement, consider reflecting on your personal journey as a carer. Think about moments where language failed to express your experience or times when your strength surprised you. Your story is valuable, and this collection is about lifting up voices that have often been overlooked.
Contact Information:
For any questions or additional information, please contact Matthew McKenzie:
This is your chance to raise awareness and inspire others by sharing your lived experiences through poetry. Help shape a future where minority carers are valued, heard, and recognized for the essential work they do. We look forward to reading your stories!
By Matthew Mckenzie – facilitator of national ethnic mental health carers forum
I’m pleased to share “Unpaid, Unseen and Yet Unbroken”, a spoken word poetry video that marks the first poem released from my forthcoming poetry collection of the same name.
This first poem speaks from within the lived reality of unpaid mental health carers, particularly those from ethnic and marginalised communities whose labour is often overlooked, misunderstood, or taken for granted. It reflects moments many carers will recognise: waiting rooms, misrecognition, quiet endurance, and the strength it takes to keep showing up without acknowledgement.
🎥 Watch the spoken word video here:
The wider collection I am currently working on brings together poems shaped by care, fatigue, love, resilience, and survival. It is a body of work rooted in lived experience and community voices, offering poetry not only as expression, but as witness and affirmation.
This first poem sets the tone for what is to come, promoting honest, reflective, and unapologetic in its call for carers to be seen, heard, and respected.
This work is part of my ongoing commitment through my A Caring Mind youtube channel to use creativity as a way to challenge stigma, amplify unheard voices, and centre care as a vital social contribution.
More poems from this collection will be shared in the coming months.