By Matthew McKenzie – Carer and Carers UK Ambassador
As unpaid carers, many of us know what it feels like to operate in the background. We juggle complex health systems, care for our loved ones, and manage our own lives, all too often feeling invisible.
That is why I am excited to share a major milestone for our community.
The Department of Health and Social Care (DHSC), alongside the Departments for Education, Business and Trade, and Work and Pensions has officially launched the Unpaid Carers Action Plan: Recognize, Refer, Reach.
This is England’s first-ever cross-government action plan dedicated entirely to supporting unpaid carers.
I was honored to attend the official launch event to represent our community, meet with Minister for Care Stephen Kinnock MP, and participate in the official DHSC launch video.
This isn’t just another policy document; it is a commitment across multiple government sectors to drive real, practical change.
The plan is built around three core pillars:
1. Recognise
Carers must be identified early. One of the most exciting digital updates is a new “MyCarer” section being introduced on the NHS App, allowing us to easily register our caring role so healthcare staff know who we are from the start.
2. Refer
No carer should have to navigate the system alone. This pillar focuses on making sure we are directed to local carer centres, financial advice, and emotional support early on. Crucially, it aims to ensure we are formally included in major healthcare decisions, like hospital discharge planning.
3. Reach
Caring shouldn’t mean giving up on your own future. For working carers, the plan explores paid carer’s leave and will require large employers (250+ staff) to publish carer support plans from spring 2027. For young carers, it means stronger support within schools so their education doesn’t suffer.
A Message to My Fellow Carers and Carer Centres
For years, we have argued that caring is not just a “health” issue, it impacts our jobs, our education, our finances, and our mental health. Seeing four government departments finally come together to address I feel is a massive step forward.
To my fellow unpaid carers: Please know that using your voice gives you a chance at being heard. It is important to get carers “on the map” to be recognised, and this plan is a direct result of carers sharing their lived experiences.
To Carer Centres and Forums: This action plan is a powerful tool for us. It gives us a framework to hold local services accountable and ensure the “Recognise, Refer, Reach” goals are delivered on the ground.
Of course change doesn’t happen overnight, but this plan gives us a vital foundation to build on. Let’s keep pushing, keep connecting, and make sure every single unpaid carer gets the recognition and support they deserve.
By Matthew McKenzie – Carer, Author, Poet and Host of the Carers UK Information Stall 10 June 2026, Perceval House, Ealing
As a carer myself, supporting both of my brothers, I understand that caring is often a role we never planned for, yet one we embrace out of love, duty and commitment. It can be rewarding, but it can also be isolating, exhausting and overwhelming. That is why events such as the Carers Week Celebration 2026, organised by Ealing Carers Partnership, Ealing Carers Hub and Ealing Council, are so important.
I think it reminds us that carers matter, that our voices are heard and that we are not alone.
Having the privilege of hosting the Carers UK information stall, while also attending as a carer, poet and author, I witnessed first-hand the incredible sense of community that filled Perceval House throughout the day.
The event brought together carers, professionals, charities, community organisations and council representatives for a celebration that was both informative and inspiring. Alongside the opportunity to gather information and advice, carers enjoyed complimentary refreshments, free manicures from students of Uxbridge College, artwork exhibitions and the chance to connect with others who truly understand the caring journey.
Carer Stalls of Support and Opportunities
One of the highlights of the day was the large exhibition area, where carers could meet a wide range of organisations offering support, guidance and practical services.
The information stalls represented the breadth of support available across Ealing and North West London. Throughout the day carers visited displays from organisations including:
Carers UK
Ealing Carers Partnership
Ealing Carers Hub
Mind
RISE
Ealing Advice Service
Harlington Hospice / Harlington Care
Independent Mental Health Advocacy Services
Volunteer Centre Ealing
Eating Disorders Support Services
Community wellbeing organisations
Health and social care providers
Local voluntary sector groups
Arts and creativity projects for carers
Community engagement and peer support groups
Many stalls offered practical information about carers’ rights, benefits, wellbeing support, mental health services, respite opportunities, advocacy and volunteering. Others showcased creative projects and community activities designed to reduce isolation and improve wellbeing.
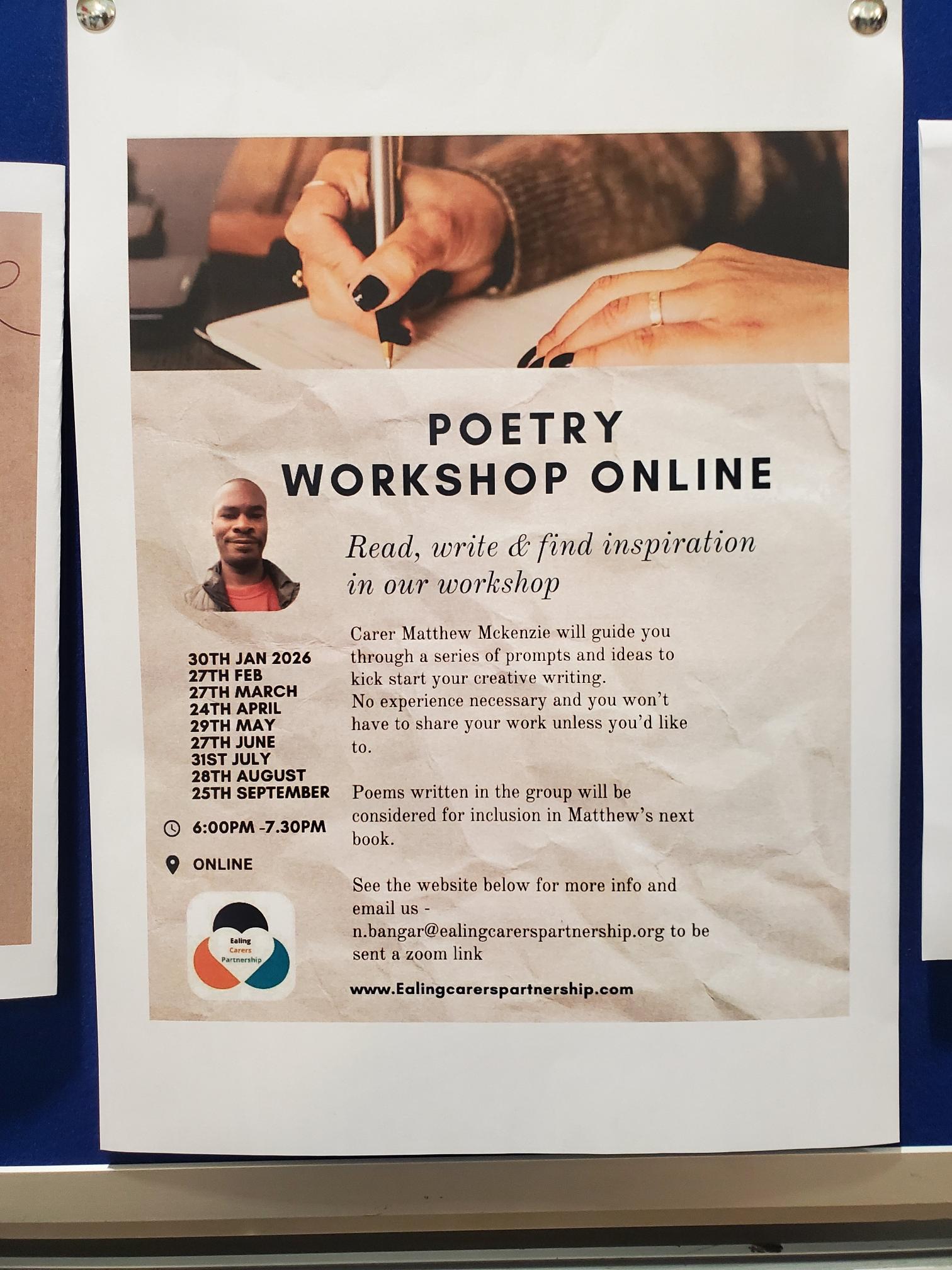
It was also great to see Carer Poetry displayed including the Carer Poetry group I run with Ealing Carers.
At the Carers UK stall, I had numerous conversations with carers who were seeking information about financial support, carers’ assessments, employment rights and how to balance caring responsibilities with their own health and wellbeing. What struck me most was how many carers were attending such an event for the first time and discovering services they never knew existed.
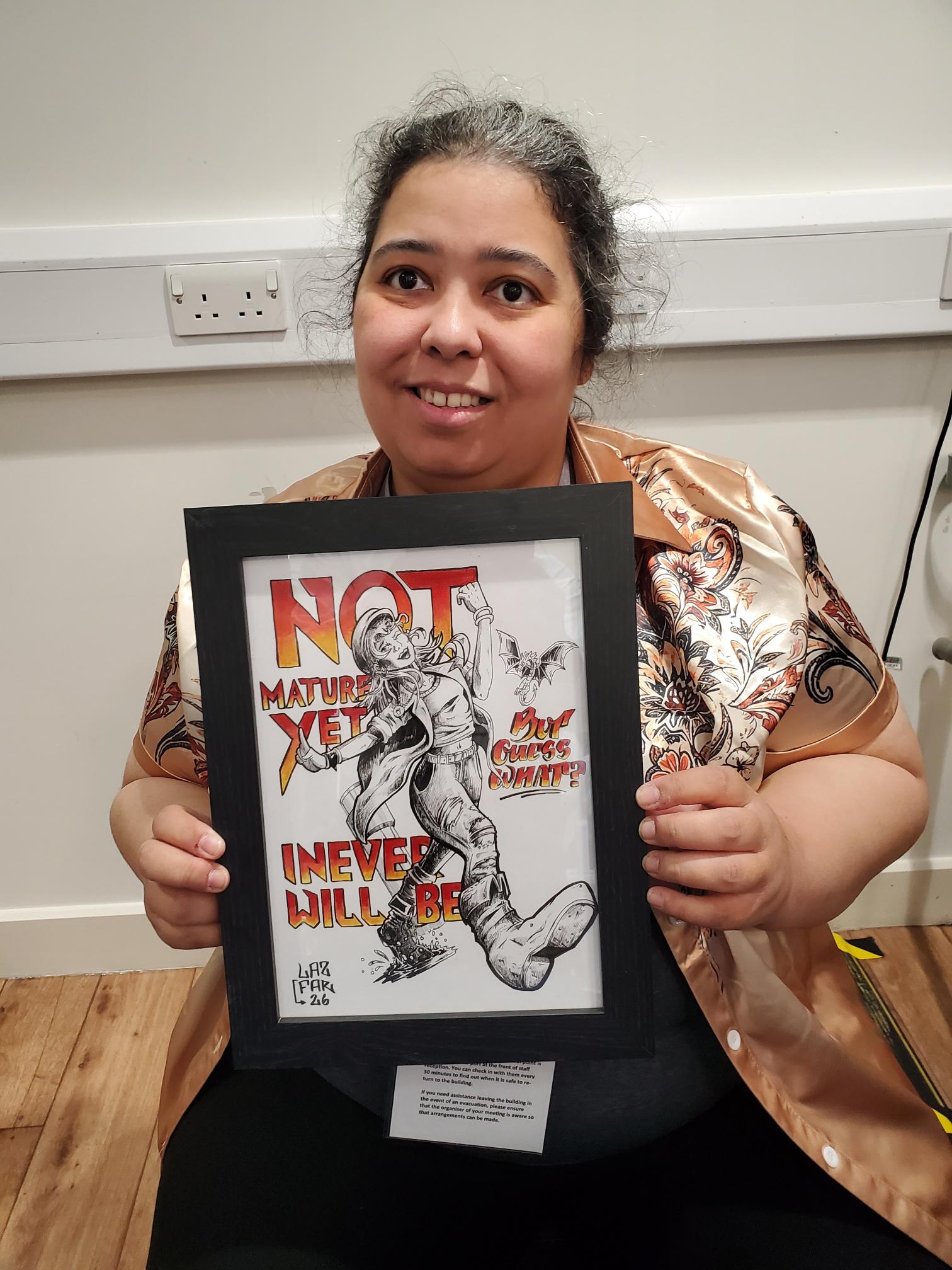
The exhibition also featured the moving “A Carer Is…” artwork display, where carers expressed their experiences through art. The exhibition provided a powerful reminder that caring is not simply a task—it is an emotional journey filled with love, sacrifice, resilience and hope.
Listening to Carers: The Ealing Carers Forum and Council Presentations
A major focus of the day was the Carers Forum and Question & Answer Session, where carers had the opportunity to hear directly from council leaders and ask questions about services, support and future plans.
The event was opened by senior representatives who acknowledged the enormous contribution carers make every day.
Among the key speakers were:
Paul Driscoll, Cabinet Member for Healthy Equal Lives, Ealing Council
Kashmir Takhar, Ealing’s Carers Commissioner
Senior representatives from Adult Social Care
Sophie (Assistant Director, Adult Social Care)
Representatives from Ealing Carers Partnership
Representatives from Ealing Carers Hub
Jane Wheeler, Chief Executive of Harlington Hospice
Paul Driscoll spoke about his commitment to understanding carers’ experiences and ensuring that Ealing’s Carers Strategy becomes a meaningful reality rather than simply another policy document. He emphasised the importance of recognition, support and partnership working with carers.
The presentation by Kashmir Takhar focused on Ealing’s Carers Strategy, a joint strategy developed in partnership with carers, health services, social care and voluntary sector organisations. The strategy highlights four key priorities:
Identifying carers early in their caring journey.
Helping carers maintain family and community life.
Supporting carers’ physical and mental wellbeing.
Helping carers maximise income and achieve their potential.
The presentation revealed that there are approximately 24,000 carers in Ealing, although many remain hidden and do not identify themselves as carers. It also highlighted the growing challenges carers face around mental health, financial pressures, access to services, respite care and social isolation.
Particularly encouraging was hearing about plans to improve access to information, increase wellbeing activities, strengthen respite opportunities and expand support for young carers and working carers.
The Power of Carers’ Voices
One of the most important aspects of the forum was the open discussion session.
Carers shared their personal experiences, raising concerns about respite services, communication between council departments, transport arrangements and the challenges of navigating complex systems while already carrying significant caring responsibilities.
A particularly powerful contribution came from a carer who described how difficult it had been to arrange respite care due to poor coordination between services. The honesty and emotion behind this contribution resonated with many people in the room because it reflected experiences that carers often face but rarely have opportunities to discuss publicly.
Council representatives acknowledged these concerns and committed to improving communication, responsiveness and coordination across services. Assistant Director Sophie openly recognised that carers deserve better experiences and welcomed continued feedback to help shape future improvements.
Representatives from frontline organisations, including Ealing Advice Service, also highlighted recurring issues encountered by carers and stressed the importance of joined-up working between agencies.
Later in the session, Jane Wheeler from Harlington Hospice explained how the organisation’s carers’ short break service supports carers through home-based respite, community outings and specialist support. Her presentation reinforced the message that carers themselves need care, support and opportunities to recharge.
It was more than just a Carers Event
As the day came to a close, what remained was a sense of connection.
For many carers, simply being in a room full of people who understood their experiences was invaluable. There was laughter, conversation, shared stories and moments of reflection. New friendships were formed, information was exchanged and carers left knowing that support is available.
From my own perspective, hosting the Carers UK stall and speaking with so many dedicated carers reinforced why events like this matter. Caring can often feel invisible. The hours spent supporting loved ones frequently go unnoticed by wider society. Yet carers are the backbone of our communities and health systems.
The Carers Week Celebration reminded us that carers deserve recognition not just during one week each year but every day.
To everyone who organised the event, staffed a stall, delivered a presentation, volunteered their time or simply attended and shared their story, I thank you.
Most importantly, to every unpaid carer reading this: thank you for everything you do.
By Matthew McKenzie – Chair of the Carers Hospital Discharge group
Hospital discharge remains one of the most critical and stressful moments for unpaid carers, patients and healthcare professionals alike. During the recent Carers Hospital Discharge Group meeting held in May 2026, professionals, carers, NHS leaders, hospital representatives and community organisations came together to discuss major developments affecting carers across London and beyond.
The Carers Hospital Discharge meeting runs every 2 months and for the month of May we discussed improving hospital discharge processes, strengthening carer identification, digital inclusion, community support and the growing role of technology in healthcare planning.
The blog update is for those unable to attend, here is a summary of the key discussions, presentations, questions and responses shared during the session.
Universal Care Plan Expansion Through the NHS App
One of the biggest updates came from NHS England, who shared exciting news about the expansion of the Universal Care Plan (UCP).
The new development allows patients and members of the public to begin creating their own Universal Care Plans directly through the NHS App. Previously, only clinicians could initiate many aspects of these plans.
NHS England explained that editable sections now include areas such as:
“What matters to me”
Communication preferences
Care and contingency plans
Personal support needs
Clinical sections, however, remain under healthcare professional control.
Updates described the project as a major milestone after years of discussion about allowing people greater control over their own care information.
Question from attendee:
“Will carers be able to input on behalf of their cared-for person?”
response from presenter:
At present, carers cannot directly complete plans on behalf of another person due to safeguarding and proxy access concerns. However, carers can still complete their own care contingency plans within the system.
It was explained that this means if a carer suddenly becomes unable to provide care, emergency services and healthcare providers would be alerted that a contingency plan exists.
They also noted that community organisations could potentially support individuals with completing plans, provided appropriate governance and data security arrangements are in place.
The discussion highlighted both the opportunities and challenges of balancing digital access with safeguarding responsibilities
*****
For more developments on the Universal Care PLan, I have provided the link below of the recent Webinar
New Research on Social Networks and Healthcare Support
Matthew McKenzie introduced an emerging research project led by Queen Mary University of London alongside several major universities including Harvard, Oxford and Warwick.
The project aims to explore how patients’ social support networks influence health outcomes, hospital admissions and long-term wellbeing.
Researchers are developing tools to map patients’ support systems, including:
Family carers
Friends
Peer groups
Community support
Online social networks
The project seeks to better understand how strong support systems can improve self-management and reduce avoidable hospital admissions.
Matthew explained that researchers are particularly interested in understanding:
Whether support network mapping would feel helpful or intrusive
How carers should be recognised within healthcare systems
How cultural differences affect support networks
What safeguards around privacy and consent are needed
The proposal sparked interest among attendees because it reflects a wider NHS shift toward community-based care and prevention.
NHS England connected the project to wider work around “family group conferencing,” where whole-family approaches are used to plan care and support more collaboratively.
NHS England’s Urgent and Emergency Care Strategy 2025/26
A major section of the meeting focused on NHS England’s emerging Urgent and Emergency Care (UEC) Strategy.
Matthew presented some notes on NHS England UEC outlining plans to:
Reduce avoidable hospital admissions
Deliver more care within communities
Expand digital healthcare access
Improve hospital discharge pathways
Strengthen operational efficiency
Key proposals included:
AI-enabled triage systems
NHS App navigation tools
Digitally coordinated urgent care
Expanded community-based treatment
Greater use of early intervention models
However, the discussion quickly moved toward the potential risks associated with rapid digital transformation.
Participants concerns:
Representatives covering Hospitals, raised important concerns about how discharge pressures could negatively affect carers.:
“If somebody urgently needs that hospital bed, the pressure becomes getting people discharged quickly. That may not always leave enough time to identify carers properly.”
They stressed that carer identification should happen throughout the patient journey not only during discharge.
They highlighted opportunities for identification during:
Outpatient appointments
Pre-assessment clinics
Routine hospital interactions
Concerns About Digital Poverty
Another major concern involved digital exclusion.
Participants warned that:
Older people
People with dementia
Individuals without smartphones
People facing poverty
Non-English speakers
Neurodivergent individuals
could all struggle if urgent care becomes too dependent on digital systems.
It was mentioned that meeting carers who still rely entirely on phone calls rather than online platforms and stressed the need for alternative accessible routes into care.
Others agreed and referenced an Equality Impact Assessment linked to the NHS 10-Year Plan, which explores risks around digital inequality and vulnerable groups being left behind.
A major highlight will be the attendance of Sir Ed Davey, who is himself a well-known advocate for unpaid carers due to his own lived experience caring for family members. His involvement is expected to help raise awareness of the challenges carers face daily.
KCN also spoke about Kingston Carers Network’s ongoing efforts to strengthen links with Kingston Hospital. The organisation already receives referrals through the hospital’s carers liaison department, helping unpaid carers access emotional support, information and practical guidance following hospital admissions or discharge.
However, KCN is now trying to expand its presence inside the hospital itself through more direct face-to-face outreach work. Plans are being discussed to establish regular information stands within hospital settings so carers can receive support earlier and more proactively.
KCN explained that while these conversations are progressing, coordinating regular in-hospital outreach remains challenging due to logistical pressures and scheduling issues. Despite this, the organisation continues to work closely with hospital teams to improve visibility and engagement with carers.
Beyond hospital settings, Kingston Carers Network continues to deliver several outreach programmes throughout the borough. Staff regularly attend local groups, community spaces and events to identify carers who may not realise support is available to them.
North Central London Carers Support Project
Eleanor updated the group on work taking place across:
Barnet
Camden
Enfield
Haringey
Islington
The project works in partnership with multiple NHS trusts and carers organisations across North Central London with the aim of creating a more consistent and coordinated approach to identifying and supporting unpaid carers.
At the centre of the programme is the development of a standard operating procedure for carers within hospitals and healthcare settings. The goal is to ensure carers are recognised earlier, referred more efficiently and supported more consistently regardless of which hospital or borough they engage with.
One of the project’s biggest developments has been the creation of a dedicated carers referral website. Eleanor explained that the system is designed to simplify the referral process for healthcare professionals. When a referral is submitted through the portal, the system automatically directs the carer to the appropriate local carers organisation based on their postcode.
The intention is to remove confusion for hospital staff while helping carers access support much faster.
Eleanor described the project as an effort to make support pathways:
Easier for professionals to navigate
More accessible for carers
Better integrated across borough boundaries
Less dependent on individual staff knowledge
A major focus of the project continues to be embedding carer awareness into everyday hospital practice.
Carer Awareness Training Expanding Across Hospitals
The team has made significant progress with carer awareness training sessions delivered across several NHS trusts.
Regular drop-in training sessions are now taking place with:
The Whittington Trust
The Royal Free
North London Mental Health Trust services
Eleanor shared that attendance at some sessions has now exceeded 40 healthcare staff members, which she described as a major success.
The training focuses on:
Identifying unpaid carers earlier
Understanding carers’ rights and needs
Improving referral pathways
Increasing staff confidence when supporting carers
Embedding carer recognition into routine clinical practice
Importantly, the project measures the effectiveness of these sessions using confidence ratings before and after training. Eleanor reported that most staff attending show at least a one- or two-level increase in confidence around identifying and supporting carers after participating.
North Central London’s Focus on Carers Week and Community Engagement
Preparations for Carers Week are also a major priority for the project.
The team plans to host information stalls and awareness events at several hospitals including:
The Whittington Hospital
University College London Hospital (UCLH)
Barnet Hospital
These events aim to:
Raise awareness of unpaid carers
Promote available support services
Encourage hospital staff to make referrals
Help carers connect with local organisations
Lewisham Council Developments
Updates from Lewisham was on the ongoing work taking place across Lewisham to improve support for unpaid carers, particularly through closer collaboration between hospitals, carers organisations and local commissioners.
A major development has been Lewisham Hospital’s involvement in the South East London pilot programme focused on creating a standard operating procedure for carers across NHS trusts. The pilot aims to improve consistency in how carers are identified, supported and referred within hospital settings.
It was explained that Lewisham Hospital has been working closely with Imago, the borough’s commissioned carers support provider, to strengthen partnerships with hospital nursing teams and improve awareness of carers across wards and services.
Particular emphasis is now being placed on:
Increasing carer awareness training
Improving communication between services
Embedding carer identification into routine hospital practice
Strengthening links between healthcare and community support
Inspired by discussions during the meeting, it was also highlighted plans to explore integrating carer identification into regular auditing and review processes within hospital settings similar to initiatives already underway in other trusts.
Redesigning Lewisham’s Future Carers Service
One of the most significant updates involved the redesign of Lewisham’s carers support service model.
They shared that the current commissioned contract for carers services is due to end in January 2027, and work is already underway to shape the next phase of support provision.
Importantly, unpaid carers themselves are playing a central role in developing the new model.
A series of co-production sessions has been held with carers across the borough to ensure their lived experiences directly influence future service design. These discussions are helping shape priorities around:
Access to support
Communication with carers
Outreach and identification
Emotional wellbeing services
Practical support needs
Hospital discharge experiences
The borough hopes to move into procurement for the redesigned service later this year.
Carers Hub Lambeth
Carers Hub Lambeth shared an update on the organisation’s ongoing work supporting unpaid carers across King’s College Hospital and Guy’s and St Thomas’ NHS Foundation Trusts.
Although the current hospital carers project funding has been extended for an additional six months, Jen explained that the programme is now approaching its final phase, with funding currently due to end in September 2026.
As a result, the team’s main focus is now on ensuring hospitals become as self-sufficient as possible in identifying and supporting carers once the dedicated project ends.
Expanding Carer Awareness Training
A major priority for Lambeth Carers Hub is expanding carer awareness training for healthcare professionals.
It was explained that the organisation has:
Increased training sessions from once to twice monthly
Begun arranging bespoke sessions with individual hospital teams
Expanded engagement with primary care networks
Updated training materials to address barriers to carer identification
The training aims to help healthcare staff:
Recognise unpaid carers earlier
Understand carers’ support needs
Improve referral pathways
Build confidence in conversations with carers
Embed carers into routine healthcare practice
Carers Hub Lambeth acknowledged that while training sessions often generate an immediate increase in referrals, maintaining long-term momentum remains challenging.
It was mentioned that a familiar pattern where professionals attend training, referrals increase temporarily, and then gradually reduce again as competing clinical pressures take over.
Because of this, the organisation is now trying to better understand:
Why carers continue to be missed
What barriers staff face in identifying carers
How carer awareness can become part of everyday practice rather than an additional task
This reflects a wider challenge discussed throughout the meeting — ensuring carer support becomes embedded within healthcare systems rather than dependent on individual staff enthusiasm.
Embedding Carer Recognition Into Everyday Hospital Practice
One of the most practical discussions came from GESH update on integrating carers into routine hospital auditing processes.
St George’s and Epsom and St Helier Hospitals are now:
Adding carer identification questions into ward audits
Including carers within routine quality checks
Training volunteers to identify carers on wards
Embedding carers into “business as usual” practice
Wendy also spoke extensively about the NHS “Reasonable Adjustments Digital Flag,” a major NHS initiative designed to ensure patients’ accessibility needs are recognised across services.
The system aims to help hospitals and GP services better identify:
Communication needs
Disabilities
Neurodivergence
Mental health conditions
Carer-related support needs
The long-term goal is for healthcare systems to automatically recognise and share reasonable adjustment requirements across services.
Final Reflections
The meeting demonstrated both optimism and concern about the future direction of health and social care.
There was strong agreement that:
Community-based care is necessary
Earlier intervention can prevent hospital admissions
Carers must be identified earlier
Digital systems offer opportunities
However, participants repeatedly stressed that healthcare transformation must not leave vulnerable people behind.
Carers remain central to safe discharge, patient wellbeing and long-term community support. As NHS services increasingly move toward digital and community-led models, ensuring carers are recognised, supported and included will remain critical.
The next Carers Hospital Discharge Group meeting is expected to take place in July 2026.
Update by Matthew McKenzie – Chair of South London Mental Health Carers Forum
The South London Mental Health Carers Group met for the month of May for a wide-ranging and thoughtful discussion covering carers’ experiences, mental health support systems, involvement opportunities, and an important research presentation focused on support networks and long-term care.
The group covers areas of Lewisham, Southwark, Lambeth & Croydon, although Mental Health Carers from outside those areas are welcime to attend
The session brought together carers, advocates, involvement leads, and guest speaker Dr Anna De Simone from Queen Mary University of London. As always, the discussion highlighted both the challenges carers continue to face and the value of shared lived experience and peer support.
Opening Discussions: Challenges in Mental Health Care Systems
The meeting began with carers sharing experiences of navigating mental health services for loved ones with complex needs. There was extensive discussion around:
difficulties accessing appropriate placements,
safeguarding concerns,
discharge planning,
lack of continuity between NHS trusts and local authorities,
and ongoing challenges around funding responsibility between different services.
A recurring issue raised was the pressure on inpatient beds and the concern that discharge decisions can sometimes feel driven more by system pressures than by clinical readiness. Carers spoke openly about the emotional impact of repeatedly having to advocate for vulnerable loved ones while navigating fragmented systems.
There was also discussion around the importance of carers being recognised and included in communication and planning processes. Participants highlighted how carers are often the people most aware of deterioration, risks, or safeguarding concerns, and how vital it is that services engage meaningfully with families and informal supporters where appropriate.
Despite frustrations, carers also acknowledged examples of good practice and supportive professionals within mental health services. Several attendees noted that they had seen gradual improvements in carer involvement and listening exercises within parts of South London and Maudsley NHS Foundation Trust (SLAM), particularly in Lambeth.
Updates on Carer Involvement and Support Activities
The group received updates from carers and representatives involved in local mental health engagement work and carers’ organisations.
Carers Week Activities
Karen from Carers Hub Lambeth shared details of upcoming Carers Week activities, including:
outreach events,
wellbeing sessions,
information stalls,
and activities for both adult and young carers.
The events aim to provide carers with opportunities for support, networking, practical advice, and wellbeing activities.
There was also discussion around changes and developments within SLAM involvement structures, including:
continuation of family and carers meetings,
changes to involvement leads,
and ongoing reviews of the involvement register.
Attendees reflected positively on the increasing recognition of carers’ voices in some forums and clinical meetings, while acknowledging that there is still much work to do to ensure consistent involvement across all boroughs and services.
Guest Presentation: Mapping Patient Support Networks
The second half of the meeting focused on a presentation from Dr Anna De Simone, GP and Associate Professor of Primary Care at Queen Mary University of London.
Anna introduced a proposed research project exploring how healthcare systems might better understand and map patients’ support networks using electronic health records and social network tools.
The research proposal focuses particularly on patients with long-term conditions such as COPD (Chronic Obstructive Pulmonary Disease), many of whom also experience multiple additional health conditions and varying levels of social isolation.
The Core Idea
Anna explained that while healthcare professionals can currently access limited information such as next of kin or household members, they often lack a fuller understanding of:
who actually supports the patient,
how reliable that support is,
whether support networks are connected or fragmented,
and how socially isolated a patient may be.
The proposed research would explore whether creating visual “maps” of support networks could help:
improve care planning,
reduce crises,
improve coordination between services,
and enhance patients’ quality of life.
The project would also examine how social prescribing, community services, online support groups, and carers fit into these wider support networks.
Carers’ Feedback on the Research Proposal
The discussion following Anna’s presentation was extremely rich and constructive, with carers offering both enthusiasm and important cautionary perspectives.
Strong Support for the Concept
Many attendees felt the project addressed an important gap in healthcare planning. Several carers spoke about how informal support networks had been essential to helping them or their loved ones survive periods of crisis.
Participants agreed that professionals often underestimate the role played by:
friends,
neighbours,
online communities,
peer groups,
and unpaid carers.
The ability to visualise these networks was seen as potentially valuable for both professionals and patients themselves.
Importance of Non-Traditional Support Networks
A strong theme throughout the discussion was that support does not always come from family.
Some carers explained that family relationships can sometimes be unsafe or abusive, and that support may instead come from trusted friends, neighbours, carers’ groups, or online communities.
The group stressed that any future system should avoid assuming that family automatically equals safety or support.
Online Communities and Digital Support
Participants also highlighted the increasing importance of online support systems.
Several carers explained that:
Zoom groups,
Facebook communities,
online peer support,
and digital communication can provide essential social connection, especially for disabled or isolated people.
One participant noted that online support networks had directly helped them access practical support and reduce isolation when physical mobility was limited.
At the same time, carers cautioned that not everyone has equal access to digital services. Concerns were raised about:
digital exclusion,
accessibility barriers,
lack of digital skills,
and the risk of widening inequalities.
The importance of offering both digital and non-digital forms of support was strongly emphasised.
Privacy, Consent, and Mental Health
Carers also discussed potential challenges around privacy and consent, particularly for people experiencing paranoia or severe mental illness.
Some attendees noted that patients may not always feel comfortable sharing details about their social networks, and that trust and safeguarding would need to be central to any future system.
There was discussion about the delicate balance between:
confidentiality,
safety,
carer involvement,
and patient autonomy.
Role of Social Prescribers
The group generally agreed that social prescribers could play an important role in helping patients map support networks, because they often have more time and a stronger focus on community support than standard GP appointments allow.
However, concerns were raised about long-term funding and sustainability for social prescribing services.
Looking Ahead
Anna thanked the group for their detailed feedback and explained that carers’ insights would help shape the next stage of the research proposal before submission later this year.
There was strong interest from attendees in remaining involved should the project move forward, particularly around future patient and public involvement opportunities.
The meeting once again demonstrated the depth of knowledge, experience, and expertise held by unpaid carers. The discussion reflected not only the challenges carers continue to face, but also the importance of ensuring carers are recognised as essential partners in both healthcare delivery and future research.
Taking time for yourself as a carer isn’t always easy. The daily responsibilities, emotional demands, and constant care for others can often mean your own wellbeing takes a back seat. That’s why initiatives like Carers Active Together matter more than ever.
This Wednesday 15 April, a national day of action is bringing carers across the UK together to focus on movement, wellbeing, and community and you’re invited to be part of it.
A simple step that makes a difference
As part of the day, Carers UK is hosting a free, friendly wellbeing walk in Hyde Park, which is a chance to pause, breathe, and connect with others who understand the caring journey.
Whether you’re caring for a loved one full-time or supporting someone alongside work and life commitments, this walk is designed to be inclusive, relaxed, and welcoming. There’s no pressure, just an opportunity to enjoy fresh air, gentle movement, and good company.
Event details
Date: Wednesday 15 April
Time: 11:00am
Location: Meet at Serpentine Bar and Kitchen, Hyde Park
Cost: Free
As highlighted on the event flyer (page 1), the walk is all about giving carers a chance to “get some fresh air, connect with your community, and enjoy a supportive stroll with local carers.”
Why join the walk?
Sometimes the smallest actions like a walk in the park can have the biggest impact. Taking part in this event can help you:
Boost your physical and mental wellbeing
Meet other carers and share experiences
Feel part of a supportive community
Take a well-deserved break in a beautiful setting
You’re not alone
Carers play an essential role in our communities, often quietly and without recognition. Carers Active Together is a reminder that your wellbeing matters too and that support is out there.
If you know someone who is a carer, consider sharing this with them. A simple invitation could make a meaningful difference.
Register your place
Spaces are free, but registration is encouraged. You can sign up here: 👉 https://bit.ly/4uEXwJO
To mark World Bipolar Day 2026, I’ve created a short video highlighting the reality of living with bipolar and the vital role of unpaid carers, friends, and family. Awareness is important, but understanding and everyday support matter just as much.
In this video, I share reflections as a mental health carer and activist, focusing on the human side of bipolar and the people who often support quietly in the background. 👉 Watch the video here: https://www.youtube.com/watch?v=gnn0tfLs2z8
World Bipolar Day is supported globally by organisations including:
In the UK, Bipolar UK (https://www.bipolaruk.org) provides vital peer support for people affected by bipolar, including carers. Carer organisations also play a crucial role in supporting unpaid carers:
I chaired our March hospital discharge network meeting with a real sense of momentum building across the system. What continues to strike me is the mix of voices in the room, commissioners, carers centres, hospital representatives, and grassroots advocates all trying to tackle the same persistent issue: how we properly involve and support unpaid carers during and after hospital discharge.
As someone with lived experience, particularly in mental health and complex care, I always come back to one key question: Are carers being treated as partners, or are they still being treated as visitors?
This meeting gave us a very honest answer progress is happening, but there is still a long way to go.
Key Presentation: Derbyshire HConnect Project
Emma’s presentation was, for me, an important part of the meeting not because it introduced something completely new, but because it clearly articulated what many carers have been saying for years, and then actually did something about it.
What stood out immediately was that this wasn’t a project designed in isolation. It was built directly from carer voice and lived experience. The starting point wasn’t “how do we improve discharge?” it was “what are carers actually experiencing right now?”
And what carers described was difficult to hear, but not surprising.
Carers spoke about not being recognised at all. Some said no one had even asked if they were a carer. Others described situations where their knowledge of the person they care for was ignored, even when it was critical. One example that stayed with me was a carer describing their loved one being discharged in the middle of winter, late at night, without proper clothing or preparation.
There was a consistent feeling that once someone enters hospital, the carer’s role is almost paused or worse, dismissed entirely.
What the HConnect project does differently is acknowledge that this isn’t just a communication issue it’s a system and culture issue.
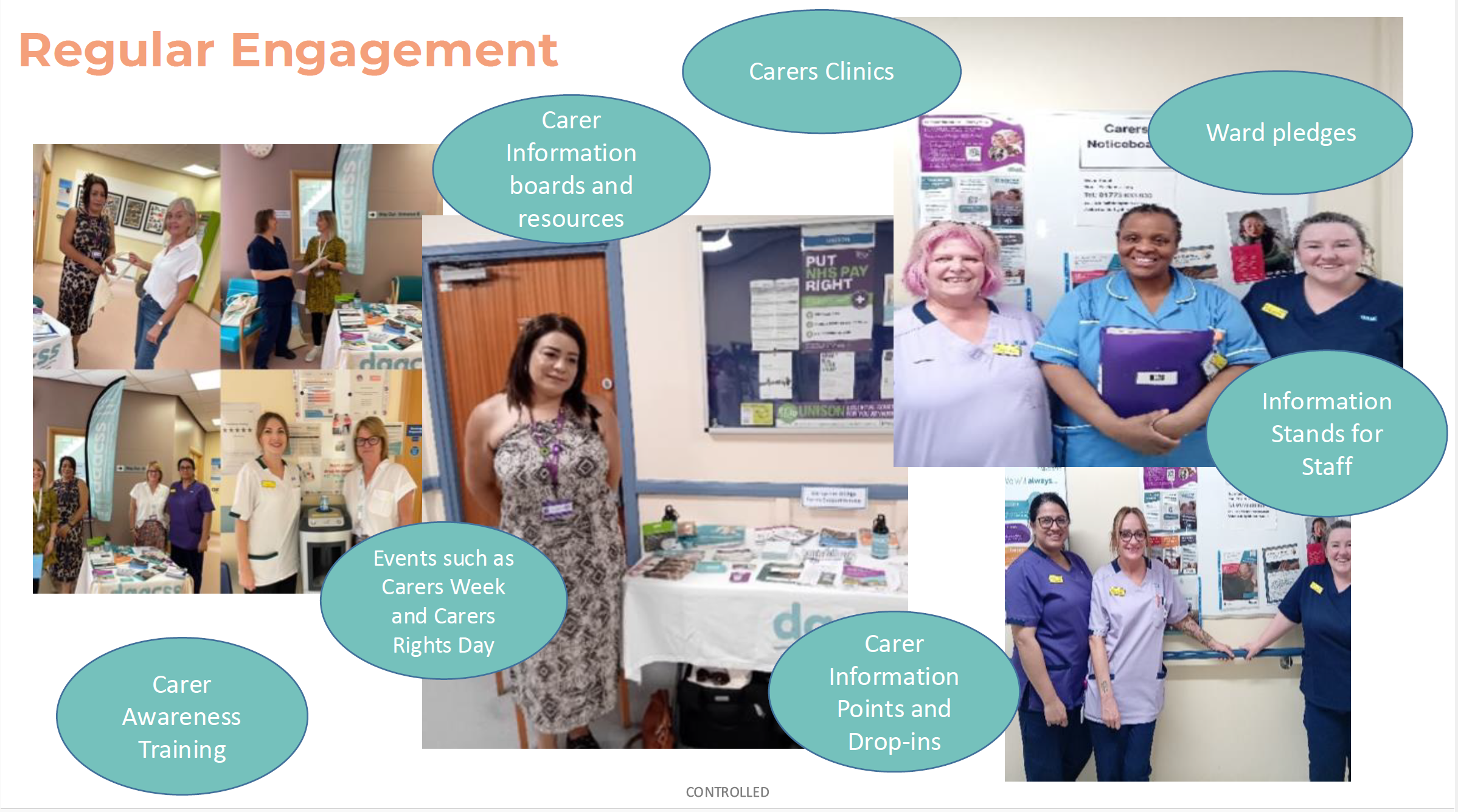
Instead of relying on one intervention, the model works across multiple layers of the hospital system. It introduces dedicated hospital liaison workers who build relationships with wards, while also ensuring carers themselves are visible and supported directly on-site. At the same time, it invests in staff through training, guidance, and practical tools so that engaging carers becomes part of everyday practice rather than an optional extra.
What I found particularly important is that the project doesn’t assume staff are unwilling—it recognises that many staff simply lack the confidence, knowledge, or structure to engage carers properly. In fact, the findings showed that many hospital teams had never received any formal carer awareness training and were often unaware that carers even have a legal right to be involved in discharge planning.
The research element of the project adds another layer of depth. Through interviews with carers, several consistent themes emerged.
Carers described feeling invisible—treated as visitors rather than partners in care. They talked about their expertise being dismissed, even when they knew the patient best. Communication was often unclear or inconsistent, and discharge frequently felt rushed, with little notice or preparation. In many cases, carers ended up acting as the safety net catching mistakes, coordinating care, and managing complex needs on their own once the person returned home.
What struck me most is that these issues aren’t just isolated incidents they are patterns.
But importantly, the presentation didn’t just focus on what’s going wrong. It also highlighted what good looks like. In situations where carers were listened to, involved early, and treated as equal partners, the entire experience changed for both the carer and the patient. The challenge now is making that level of practice consistent, not exceptional.
The project is already showing tangible impact. There has been a noticeable increase in carers being identified within hospital settings, more referrals coming directly from health professionals, and hundreds of carers receiving support through the programme.
For me, the biggest takeaway from this presentation is this:
This isn’t about adding more services it’s about changing behaviour across the system.
The HConnect model recognises that for carers to be properly involved, three things need to be in place: staff need the capability to identify carers, the opportunity within the system to engage them, and the motivation to see this as a core part of care. Without all three, change simply won’t stick.
And that’s why this work matters. Because until carers are consistently seen, heard, and included, we will continue to see the same issues repeating no matter how many initiatives we introduce.
Lewisham Commissioner Update
From Lewisham’s commissioning side, there were some strong practical developments.
A key initiative is the rollout of a carer welcome pack, designed to be:
Clearly visible in hospital settings
Easily accessible to carers at the point of need
This is being strengthened through:
Increased collaboration with hospital staff
Plans to expand distribution across wards
From Lewisham, we also received a really significant update around system-level change, particularly the development of a Standard Operating Procedure (SOP) for engaging unpaid carers in hospital settings.
This work has been led across South East London ICB, with an external partner supporting the design. The aim of the SOP is to provide:
Clear guidance to hospital wards
Practical prompts and questions for staff
A consistent approach to identifying and engaging carers during hospital stays
What stood out to me is that this isn’t just a document, it’s designed to change behaviour on the ground. It focuses on something simple but powerful: how staff start conversations with carers and recognise the people already supporting patients.
In Lewisham, University Hospital Lewisham was selected as one of the pilot sites, with two wards testing the approach. The next stage is particularly important:
The SOP is being embedded into Trust templates
It is due to be presented to the Trust board for formal approval
There are plans to roll this out across Lewisham and Greenwich NHS Trust, including Queen Elizabeth Hospital (Woolwich)
What I found especially encouraging is that carers have been involved throughout:
Input gathered through workshops
Further feedback taken to the Lewisham Council’s Open Carers Forum
Ongoing opportunity for boroughs to adapt the SOP to local needs
Alongside this, Lewisham is continuing practical work on the ground:
Strengthening links between commissioned carers services and hospital staff
Expanding visibility through carer welcome packs and information points within the hospital
For me, this is one of the most important developments discussed in the meeting. If implemented properly, a shared SOP like this has the potential to:
Reduce inconsistency across wards
Embed carer identification into everyday practice
Move us closer to a system where carers are routinely recognised—not accidentally discovered
Hospital Update: Lewisham & Greenwich NHS Trust
A really important contribution came from the patient experience perspective at Lewisham and Greenwich NHS Trust, which covers University Hospital Lewisham and Queen Elizabeth Hospital (Woolwich).
From the Trust side, there was clear recognition that:
The work carers are doing is valuable and essential to patient outcomes
There is a need to improve physical visibility of carer support within hospital settings
Space and infrastructure need to better support engagement (for example, identifying a permanent location for carer engagement and resources)
There was also a willingness to:
Explore how carer-led engagement (including my own involvement) can be better embedded within the hospital environment
Strengthen links between patient experience teams and carers organisations
From my perspective, this was a positive and practical discussion. Too often we talk about engagement in theory—but here we were talking about where the table actually goes on the ward, and that level of detail matters.
Because if carers can’t see you, they can’t access you.
Greenwich (Commissioning & Mental Health)
Greenwich colleagues spoke about their broader system approach, particularly within mental health.
Their focus includes:
Identifying gaps in carer support across services
Embedding carers within commissioning priorities
Understanding what carers themselves want from local systems
They also posed an important question to the group: What should local authorities prioritise for carers?
My answer was straightforward: We need clear leadership and accountability, a named person or role responsible for carers across the system.
Without that, good work risks becoming fragmented.
Lambeth Carers Hub (King’s College Hospital & St Thomas’ Hospital)
Lambeth shared a detailed and honest update regarding their work across King’s College Hospital and Guys and St Thomas Hospital
Key points included:
Their hospital discharge project is continuing, but with reduced capacity due to funding constraints
They have secured a short-term extension, allowing work to continue until September
A major focus is now embedding carer awareness training into staff induction processes
Importantly, they raised a systemic issue:
The need to hold commissioned care agencies accountable, particularly when carers report poor-quality care after discharge
This is critical. Discharge doesn’t end at the hospital door—if the care package fails, the whole system fails.
Southwark Council Update
From Southwark, we heard about work being done at a system level, particularly linked to:
Development of discharge information resources across South East London
Collaboration across boroughs and NHS partners
The intention is for these resources to be:
Widely accessible and adaptable
Used across multiple organisations, rather than siloed locally
Given the proximity to major hospitals like King’s College Hospital and GSTT hosptal, this kind of coordinated approach is essential.
City & Hackney Carers Centre (Homerton Hospital)
A more concerning update came from City & Hackney, particularly regarding work linked to Homerton Hospital.
They reported:
The loss of a hospital discharge worker role
A significant drop in referrals to the carers centre as a result
Reduced presence within the hospital environment
This clearly demonstrates something we often say but don’t always quantify:
When you remove dedicated roles, you remove outcomes.
The worker’s presence had been directly contributing to engagement and referrals. Without that, carers are once again at risk of being missed.
Richmond Carers Centre (Kingston Hospital)
Updates from Richmond Carers Centre highlighted both strong engagement and opportunities to build further.
Positives:
Strong referral pathways coming through from Kingston Hospital, particularly linked to discharge activity
Ongoing professional awareness work, helping improve understanding of carers across services
There is a clear foundation here, with established relationships already supporting carers into services. The opportunity now is to build on that by increasing visibility and strengthening in-hospital engagement further.
Richmond Borough Mind (Springfield Hospital – SWLSTG)
From Richmond Borough Mind, the focus was more specifically on their work within South West London and St George’s Mental Health Trust (SWLSTG), particularly at Springfield Hospital.
Key challenges highlighted:
Difficulty accessing wards within Springfield Hospital, limiting direct engagement with carers
Limited contact with carers when based in general hospital areas rather than embedded on wards
Ongoing challenge in identifying where carers are most visible and reachable within mental health settings
What came through strongly is that, despite proactive efforts such as setting up stands and being present on-site, footfall from carers remains low unless services are embedded directly into ward environments.
This reinforces a key point for me:
In mental health settings especially, access is everything—if you’re not where carers are, you simply won’t reach them.
Bexley Carers (Post-Discharge & Reablement Focus)
Bexley brought an important perspective that often gets overlooked what happens after discharge.
Their work is focusing on:
Supporting carers once reablement packages end
Recognising that carers often deprioritise themselves during discharge, only to struggle later
Increasing concern around safeguarding and mental health, particularly in dementia care
This is where we need to shift thinking: Discharge is not the endpoint—it’s the start of a new phase of care.
Cross-Cutting Reflections
Across all updates, several consistent themes emerged:
Inconsistent carer identification across wards and trusts
Funding fragility, with projects often short-term
Need for embedded training, not optional sessions
Importance of visibility within hospital environments
Gaps in post-discharge support, especially after reablement
My Closing Thoughts
Chairing this meeting, I was struck by both the progress and the gaps.
There is innovation happening in Derbyshire, in Lambeth, in Lewisham, across South East London. But it’s uneven. And carers feel that inconsistency every day.
For me, the priority remains clear:
Identify carers early
Involve them properly
Support them beyond discharge
Because when we get that right, everything else improves—outcomes, safety, and experience.
And until we get that right consistently, we still have work to do.
This week as of this blog post, the London Assembly published a major new report on unpaid carers: “London’s unpaid carers: Caring for the carers.”
I had the opportunity to contribute to this work as a carer and advocate, alongside others who shared their lived experience. Seeing those voices reflected in the final report is both encouraging and a reminder of how much still needs to change for unpaid carers in London.
One of the strongest messages in the report is that many unpaid carers are still not identified.
Too often, people caring for a partner, parent, or child don’t even realise they are classed as a “carer” which means they miss out on financial support, services, and basic recognition.
From my own experience, and what was shared at the Assembly, this is especially true for:
Mental health carers
Carers from ethnic minority backgrounds
Indentification of unpaid carers
If you’re not identified, I feel you don’t exist in the system.
Financial pressure is a major issue
The report possibly confirms what many carers already know:
Nearly 1 in 3 carers in London are living in poverty
Carer’s Allowance is not enough to live on
Many carers have to reduce work or leave employment entirely
There are positive recommendations here like reviewing Carer’s Allowance and reducing travel costs, but these need to turn into real change, not just policy discussions.
Support isn’t working as it should
Another issue raised in the report and something I spoke about is that support often feels like a “tick-box exercise”.
Carers go through assessments, but:
Support is limited
Funding is inconsistent
Real help (like respite care) is hard to access, especially for mental health carers, I mean what does respite actually mean for mental health unpaid carers?
Identification alone isn’t enough. I think It has to lead to meaningful, practical support.
So what needs to happen next?
The report makes some important recommendations:
Better identification of carers across London
More funding for local carer services
Changes to Carer’s Allowance
Improved workplace support
and a lot more, but you would have to go through the report.
But the key question now is: will this actually be implemented?
Carers don’t need more recognition alone we need action.
Final thoughts
Unpaid carers are holding up the health and social care system every single day.
This report is a very important step forward. But it should be the beginning of change not the end of the conversation.
If you are a carer, or know someone who is, I’d encourage you to read the report and share your experiences. The more visible carers are, the harder it is for the system to ignore us.
If you’re an unpaid carer in Southwark, chances are you’re used to putting everyone else first. You support a loved one day in, day out, emotionally, practically, often invisibly. And too often, decisions about “support” for carers are made without carers truly being heard.
Southwark Council is developing its Unpaid Carers Strategy, and they are inviting unpaid carers to take part in upcoming focus groups to share real experiences, which are your lived reality.
As an unpaid carer myself, I know how rare and valuable this opportunity is.
Why having your say is important because
Policies and strategies shape:
What support is available
How easy (or hard) it is to access help
Whether carers feel recognised, supported, and understood
When carers don’t speak up, systems are built around us, not with us. When we do speak up, its a chance to make change becomes possible.
This isn’t about complaining. It’s about being honest: what works, what doesn’t, and what would genuinely make life easier for carers in Southwark.
Your voice could help shape:
Better access to information and services
More flexible, carer-friendly support
A strategy that reflects the real pressures carers face
A safe, non-judgemental space
One of the most important things about these focus groups is that they are designed to be:
Non-judgemental
Inclusive
Open to carers with any level of responsibility
You don’t need to have all the answers. You don’t need to be an “expert”. You just need your experience.
Whether you care full-time, part-time, occasionally, or don’t even label yourself as a “carer” your perspective still counts.
Focus group dates and details
In-person focus groups 📅 24th February ⏰ 11am – 1pmand2pm – 4pm 📍 Harriet Hardy Community Centre Harriet-Hardy Building, Aylesbury Estate, Albany Road, Walworth SE5 0AH
Online focus group 📅 25th February ⏰ 7pm 💻 Virtual session via Microsoft Teams
How to get involved
You can:
Scan the QR code on the flyer shown above my blog to register your interest
By Matthew McKenzie, Co-Facilitator – SW London Carers Forum
About the South West London Carers Group
The South West London Carers Group brings together unpaid mental health carers from across the boroughs of Sutton, Merton, Wandsworth, Richmond and Kingston, to share experiences, gain peer support, and stay informed about local health and social care developments.
The group provides a safe and welcoming space where carers can discuss the challenges of supporting loved ones particularly those with long-term conditions or mental health needs while also learning from guest speakers, professionals, and each other. Co-facilitated by myself, the forum plays an important role in making carers’ voices heard and strengthening connections between carers and local NHS, mental health, and community services.
Our November South West London Carers Group meeting brought one of the most informative sessions we’ve had all year. We were joined by Dalvinder, the Patient Experience Lead for NHS 111, who provided a thorough and eye-opening look at how the 111 urgent care service really works, what carers can expect, and how the system is evolving.
Dal’s role involves reviewing patient feedback, monitoring the quality of calls, and ensuring that the service remains compassionate, safe, and responsive. He also regularly meets with community groups, like ours to raise awareness of what 111 can offer.
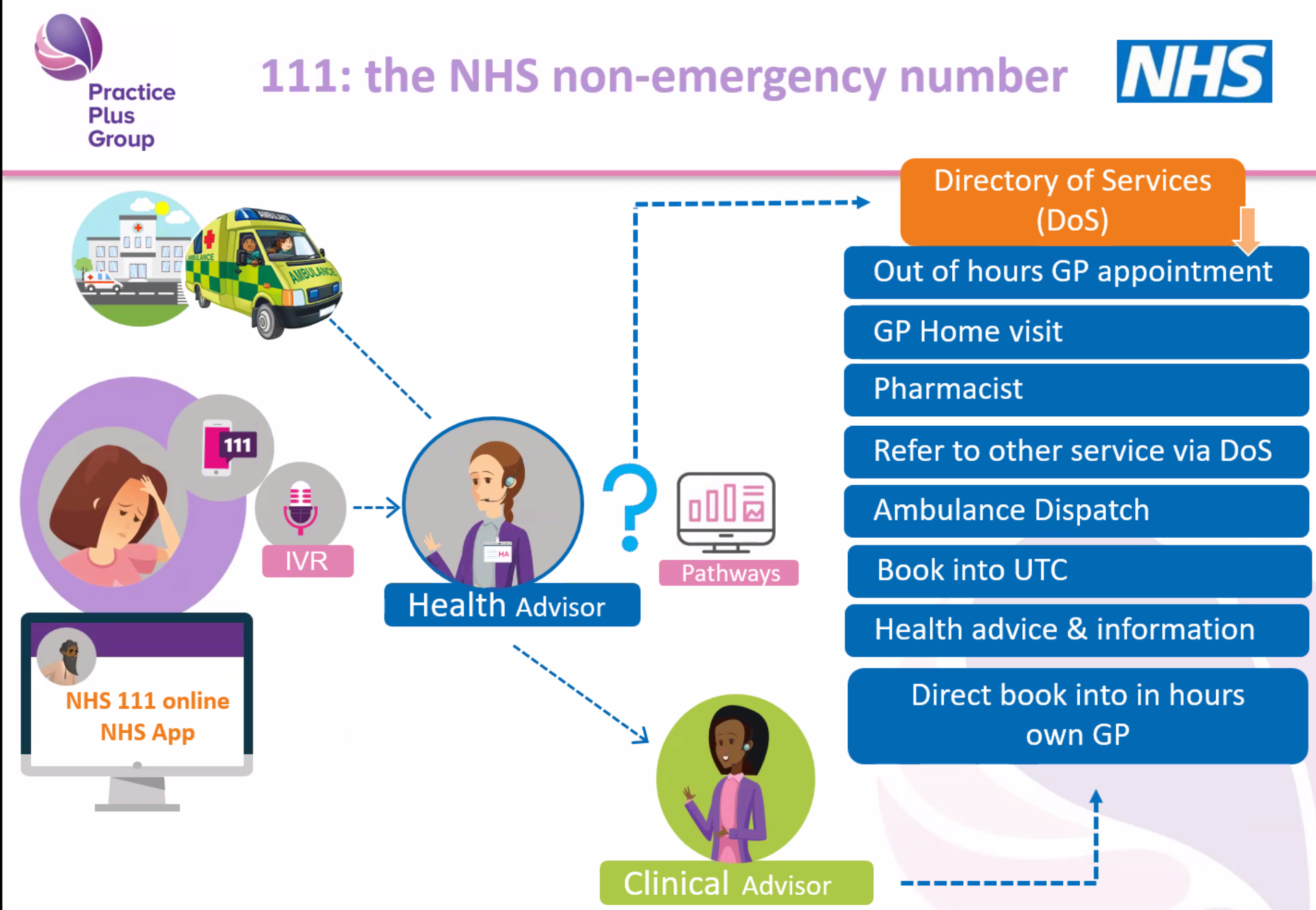
24/7 Telephone Assessments
Dal opened by reminding us that NHS 111 operates 24 hours a day, 365 days a year, and never closes. The telephone assessment is often the first point of contact, and callers speak to a trained health advisor who uses the NHS Pathways system to ask structured questions. This ensures the call handler can rule out serious issues and direct the caller to the right service quickly. Dal emphasised that while questions can feel detailed or repetitive, each answer opens or closes clinical “pathways,” helping the system determine the safest next step.
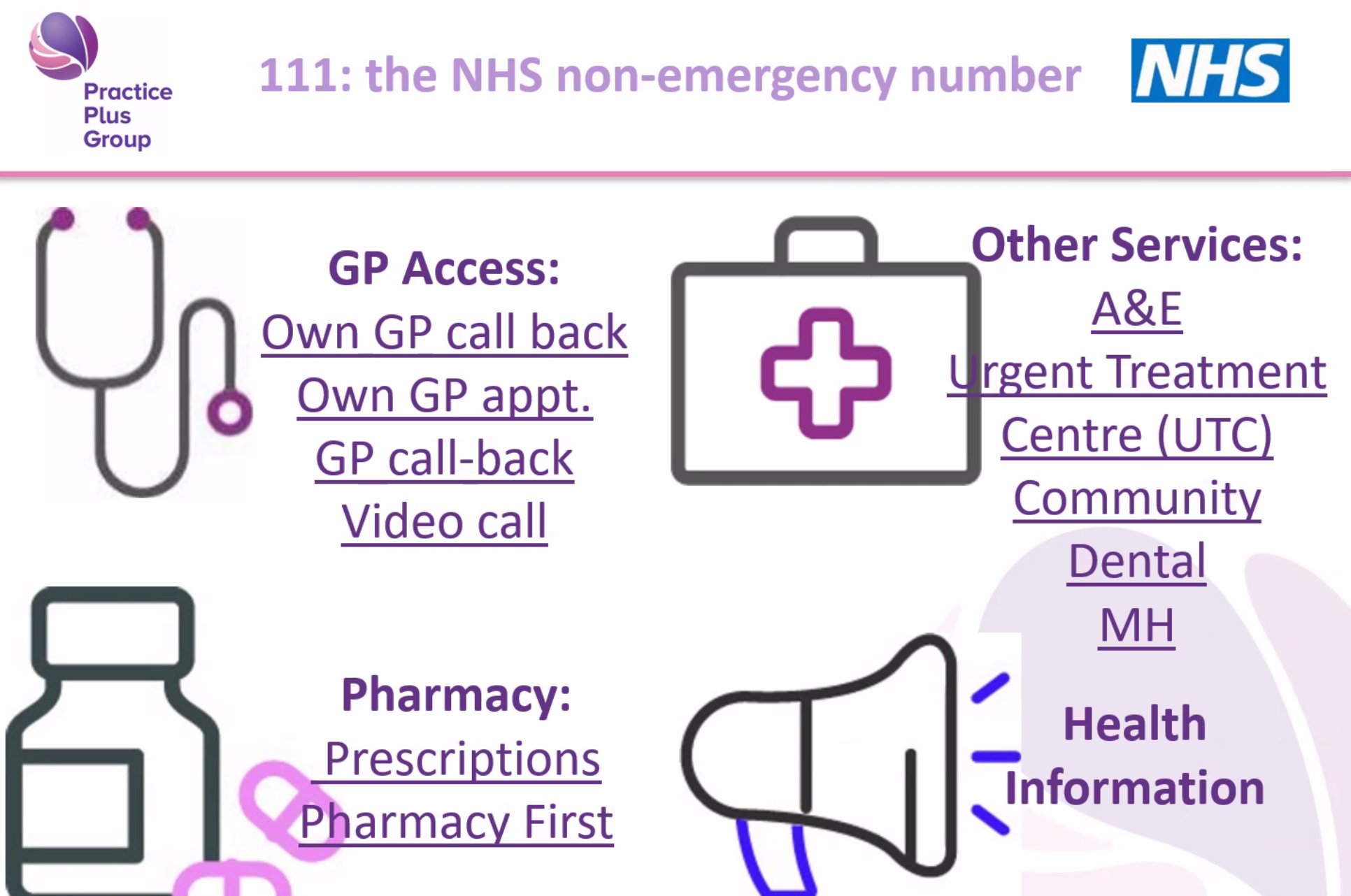
GP Home Visiting (Evenings, Overnights, Weekends)
One of the biggest surprises for many carers was learning that NHS 111 has a GP home visiting service, specifically for times when GP surgeries are closed weekday evenings, overnight, weekends, and bank holidays. This service is intended for people who cannot safely travel, including those with mobility issues, caring responsibilities, or urgent health needs that don’t require hospital care. If a home visit is determined to be appropriate, a GP working for 111 can visit in a dedicated GP car and may provide medication on the spot or issue prescriptions if needed.
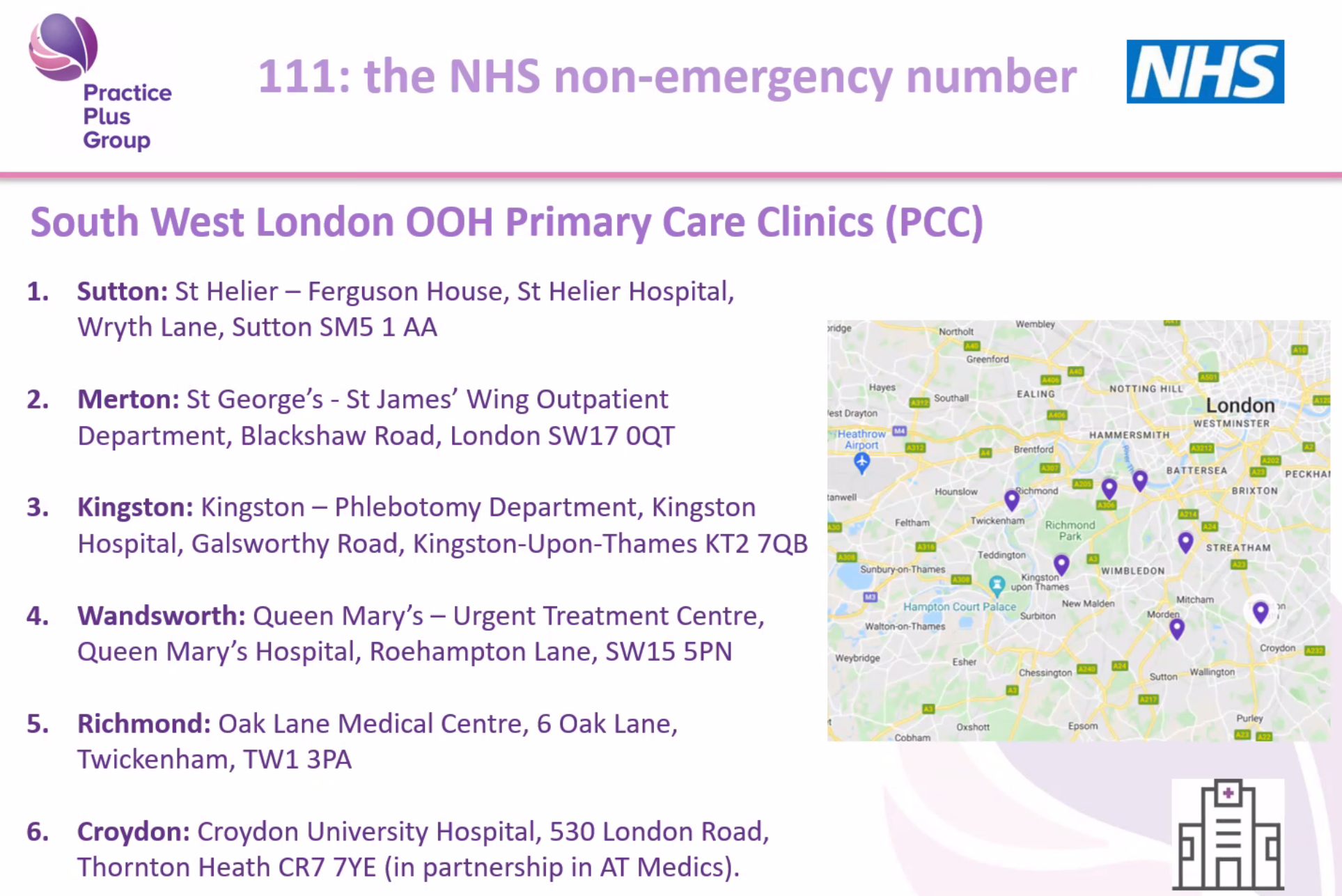
Primary Care Clinics (PCCs) – Same-Day Appointments via 111
Dal also explained the role of Primary Care Clinics (PCCs) located across South West London. These clinics operate outside normal GP hours and can see patients the same day—but crucially, access is by 111 referral only. If 111 decides that someone needs to see a GP face-to-face and can travel, they may be booked into a PCC appointment. Carers learned that you cannot walk into these clinics directly; 111 must assess the situation and confirm the appointment. This helps manage demand and ensures that appointments go to those who need them most urgently.
The Expanding Role of Pharmacies and “Pharmacy First”
Another major theme was the evolving role of pharmacies in urgent care. Dal explained that pharmacists are highly trained professionals—more trained than many realise—and 111 can now direct callers to pharmacists for assessments, repeat prescriptions, and urgent medication needs. The Pharmacy First scheme allows some pharmacies to provide consultations and treatment in private rooms for a range of minor illnesses. 111 can also arrange emergency prescription access if someone runs out of routine medication while travelling, provided the medication is part of their regular treatment.
Arranging Call-Backs From Your Own GP
In certain situations, NHS 111 can request that your own GP practice contacts you, especially for non-face-to-face issues such as renewal of regular medication, questions about paperwork, or administrative needs. While GP appointment slots reserved for 111 are limited and fill quickly, the service can still send urgent notifications to GP surgeries when clinically necessary. Dal encouraged carers to mention when the need is time-sensitive so the system can prioritise appropriately.
Mental Health Support via 111 Option 2
One of the most important updates for mental health carers was the introduction of 111 Option 2, currently being trialled across London. When callers choose this option, the call is diverted away from standard 111 and straight to local specialist mental health teams, who can assess issues such as relapse, agitation, distress, changes in behaviour, or crises at home. Dal emphasised that while 111 is not a specialist mental health service, Option 2 ensures that people with mental health needs receive expert support. Data from the pilot is expected next year, and Dal offered to return to share the outcomes.
What We Learned About NHS 111
Many carers know the NHS 111 number exists, but few realise the range of services behind it. Dal explained that 111 is a free, 24/7 service (including weekends and holidays) designed for urgent health concerns that are not life-threatening.
Many carers commented that they had no idea 111 provided such a broad range of services.
Questions From Carers
Carers asked many thoughtful and practical questions during the session, including:
1. Mental Health Crises
A carer asked how 111 responds to mental health emergencies, particularly when someone becomes distressed, unwell, or difficult to support at home.
Dal explained that 111 itself is a generic urgent care service, but Option 2 sends callers straight to trained mental health professionals, who can triage cases such as relapse, agitation, or risk concerns in a more specialist way.
2. Access to Medical Records
A question was raised about whether 111’s clinicians can view a patient’s medical history.
Dal clarified that clinicians have access to the Summary Care Record, containing essential medical information, medications, conditions, and recent interactions—if the caller gives consent.
3. Home Visiting Times and Coverage
Carers asked about response times and geographical limits.
Dal explained that SW London is fully covered, though travel times vary depending on the area and how busy the service is. Home visiting is evenings, nights, and weekends only.
4. Staffing Levels and Training
One question focused on whether call handlers are medically trained.
Dal shared that 111 employs 180 health advisors in SW London—non-clinical staff who have completed an intensive six-week training program. They follow the NHS Pathways system and are supported by clinical advisors (GPs, nurses, paramedics) who can join or take over calls when needed.
5. Using 111 When Travelling
A carer asked about getting medication while away from home.
Dal explained that 111 can arrange for prescription collections at pharmacies in another part of England, which has helped many travellers who forget medication.
6. Hearing Impairment and Accessibility
There was interest in support for people who cannot make phone calls.
Dal confirmed services such as text relay, online 111, and the NHS App, all of which improve accessibility for carers and patients with additional needs.
Carer Reflections and Experiences
Several carers shared personal experiences both positive and challenging. One described how 111 triage was vital when they urgently needed treatment for a severe infection, while another discussed difficulties when GP surgeries didn’t always respond quickly to reports sent by 111. These real stories helped emphasise how important it is for carers to know when and how to use the service, and how essential accurate information is during triage.
Key Tips Dal Shared for Carers
Give as much information as possible, including social factors such as caring responsibilities, mobility challenges, or inability to travel.
Stay with the person you’re calling about, as the call handler will ask you to check symptoms in real time.
Tell 111 if symptoms change—this can alter the urgency and outcome.
Always keep your phone nearby when waiting for a callback; 111 will try only three times.
Don’t hesitate to call again if you’re unsure or worried.
Closing Thoughts
The session was incredibly well-received. Many carers said they learned things they never knew, even though they had used 111 before. Dal’s openness and honesty—both about what the service can do and what its limitations are—made his presentation especially valuable.
As co-facilitator, I (Matthew McKenzie) will continue to share information like this to help carers navigate local health services more confidently. We hope to invite Dal back once the evaluation of 111 Option 2 (mental health) is published, we also have a keen interest on what the ICB is doing especially regarding carer involvement.