I feel Unpaid carers play a vital role in supporting loved ones experiencing mental health challenges. Much of this caring happens quietly in homes, during sleepless nights, through appointments, advocacy, and everyday acts of protection and support.
For many carers from minority communities, this experiences also includes navigating the cultural understanding, language differences, and systems that sometimes do not always recognise or reflect communities. Despite the knowledge carers hold, I feel our voices can sometimes feel overlooked in those decisions about care.
I recently wrote and recorded a short spoken word poem titled “Nothing About Us Without Us.” This poem reflects a simple and important message: carers bring lived experience that should be included in conversations about mental health services.
The poem is taken from the book I am developing called “Unpaid, Unseen and Yet Unbroken”
Carers are not just supporters in the background. Carers can carry knowledge shaped by lived reality by caring, advocating, and supporting our families through complex systems.
The poem also speaks to the importance of co-production. When carers, communities, and professionals work together, services can become more understanding and culturally responsive, and equitable.
I think this message is especially relevant to ongoing work around the Patient and Carer Race Equality Framework (PCREF), which encourages meaningful involvement of people with lived experience in shaping mental health services.
The poem is a small creative contribution to that conversation. It invites us to reflect on a few simple questions:
Are carers from different backgrounds being listened to?
Are those lived experiences shaping services?
Are decisions being made with carers, not about them?
Listening to carers is not just a gesture of inclusion it can lead to better understanding, stronger partnerships, and better care.
If you would like to watch the poem, you can find the video here:
I hope my poem encourages reflection and conversation about how we can continue building services with communities, and not just for them.
On 25th February 2026, I had the privilege of speaking at the Carers’ Forum hosted by Involve Kent.
Involve is a voluntary sector infrastructure organisation in Kent that supports unpaid carers by providing information, advice and practical help to make caring more manageable.
They organise regular carers’ forums and events where carers can meet each other, access specialist support services, hear from guest speakers on issues like benefits, legal rights and wellbeing, and contribute their lived experience to local planning and decision-making. Involve also connects carers with tailored resources, signposts to relevant services across health, social care and community sectors, and advocates for carers’ voices to be heard by policymakers and service providers
The forum ran from 10:30am to 1:30pm and brought together unpaid carers from across Kent to connect, learn and have their voices heard.
It was my second time speaking at this forum, and once again I was struck by something powerful: the room was full. That might sound simple, but in the world of unpaid caring which can often feel isolating and invisible a full room means solidarity. It means people are choosing, despite exhaustion and competing demands, to show up for themselves and each other.
Arriving and the atmosphere
From the moment I walked in, there was a real sense of warmth. Information stands lined the hall Involve, Citizens Advice, mental health services, energy advice, leisure services and more. Tables were covered in leaflets, conversations were already flowing, and carers were reconnecting with familiar faces.
The purpose of the forum was clear:
To enable those caring unpaid for an adult family member, partner or friend to meet, gain information about services in their community and have their voices heard .
That last part to have their voices heard is what resonated most with me.
It was also good to see Carer leads from Cygnet Maidstone engaging with carers in the community of Kent.
My talk: Caring for someone with a mental health diagnosis
I spoke about caring for someone with a mental health diagnosis and the Patient and Carer Race Equality Framework .
As many know, I cared for my mother who lived with schizophrenia, and I now support a close friend who lives with personality disorder and addiction challenges. I don’t speak as a clinician. I spoke as someone who has sat in GP waiting rooms, on inpatient wards, in crisis meetings, and at home during those “screaming silences” that carers know too well.
I shared:
The confusion I felt when I didn’t even realise I was a “carer”
The frustration of confidentiality barriers
The loneliness of not being listened to
The emotional exhaustion that comes from constantly firefighting crises
I then shared a poem to promote carers rights
But I also shared something equally important: growth, advocacy and solidarity.
I encouraged carers to:
Educate themselves about the condition they are supporting
Learn the difference between symptoms and personality
Understand triggers
Forgive themselves for mistakes
And most importantly, look after their own wellbeing
One message I always return to was – You cannot pour from an empty cup.
I also spoke about The Patient Carer Race Equality Framework
It exists because there is clear evidence of:
Disproportionate detentions under the Mental Health Act
Poorer outcomes for Black and minority ethnic patients
Higher levels of distrust between communities and services
Carers feeling unheard or excluded
I spoke about how minority carers can face:
Cultural misunderstandings
Language barriers
Stigma around mental health within communities
Fear of services due to past discrimination
A lack of culturally appropriate support
Discussion tables: Carers influencing change
After my talk, Clara from Involve led discussions feeding into Kent’s Health Needs Assessment for carers. Carers were asked:
How do you recognise when it’s time to ask for help?
What causes burnout?
What would a carer-friendly community look like?
These wete not token questions. Staff took notes (without identifying details) so carers’ lived experiences could directly inform local planning .
I moved around the room speaking with carers. Some were open and vocal. Others were quieter, but their listening was just as powerful. Not everyone wants to speak publicly and that’s okay. Being present is also participation too.
Power of Attorney – protecting your voice
Later in the morning, Glen Miles spoke about the Mental Capacity Act and Lasting Power of Attorney .
As carers, we often assume we will automatically be consulted in crises. The reality is different. Without legal authority, our ability to advocate can be limited.
One key takeaway:
Don’t delay in arranging Lasting Powers of Attorney.
If you want your voice – or your loved one’s voice – to be heard, formalise it.
For carers who have experienced being excluded from decisions, this was a particularly important session.
Citizens Advice & practical support
Ian from Citizens Advice spoke before lunch about benefits, debt, housing and confidential support .
With the cost of living crisis, carers are under immense financial pressure. Many reduce employment hours or leave work entirely. The session was a reminder that:
Advice is free
It is confidential
You can attend anonymously
You are not judged
Lunch followed – catered by Fusion – and honestly, some of the most meaningful conversations happen over sandwiches. Carers swapping stories. Sharing phone numbers. Recommending services. That peer-to-peer support is priceless.
What stayed with me
What stayed with me most wasn’t just the agenda or the presentations.
It was:
The older carer quietly nodding as I spoke about emotional exhaustion.
The new carer asking, “Is it normal to feel this angry sometimes?”
The male carers who stayed behind to speak to me privately.
The carers from minority backgrounds who spoke about cultural barriers and stigma.
These forums matter because carers matter.
Unpaid carers save the system billions. But beyond economics, we hold families together. We absorb crises. We advocate in rooms where we’re not always welcomed.
The Patient and Carer Race Equality Framework (PCREF) is a landmark policy designed to improve racial equity in NHS mental health care. But if it’s going to deliver meaningful change, one key voice must be placed at its centre: the carer.
Watch the video
Putting the “C” (Carer) into PCREF
In this vlog, I explore why unpaid ethnic minority carers — who are often the backbone of support for people with mental health needs — are still too often excluded from decision-making, planning, and implementation in services designed to support both them and their loved ones
A Shared Movement
Integrating PCREF and Triangle of Care is a commitment to transforming relationships in mental health care.
Carers are not just an add-on. They are central to safe, equitable, and culturally competent services.
Watch the video above, share your thoughts, and join the conversation.
By Matthew McKenzie – Triangle of Care Community Chair.
The meeting opened with a welcome to carers, professionals, and partner organisations, reinforcing the importance of the Community Group as a collaborative and inclusive space. The Chair highlighted the ongoing commitment to co-production, ensuring that lived experience remains central to all Triangle of Care development and decision-making.
The purpose of the meeting was outlined, with emphasis on shared learning, constructive challenge, and influencing national work. Members were reminded that discussions within the group directly inform improvements to Triangle of Care standards, guidance, and implementation across services.
2. Triangle of Care Update (with Q&A)
Mary Patel – Carers Trust
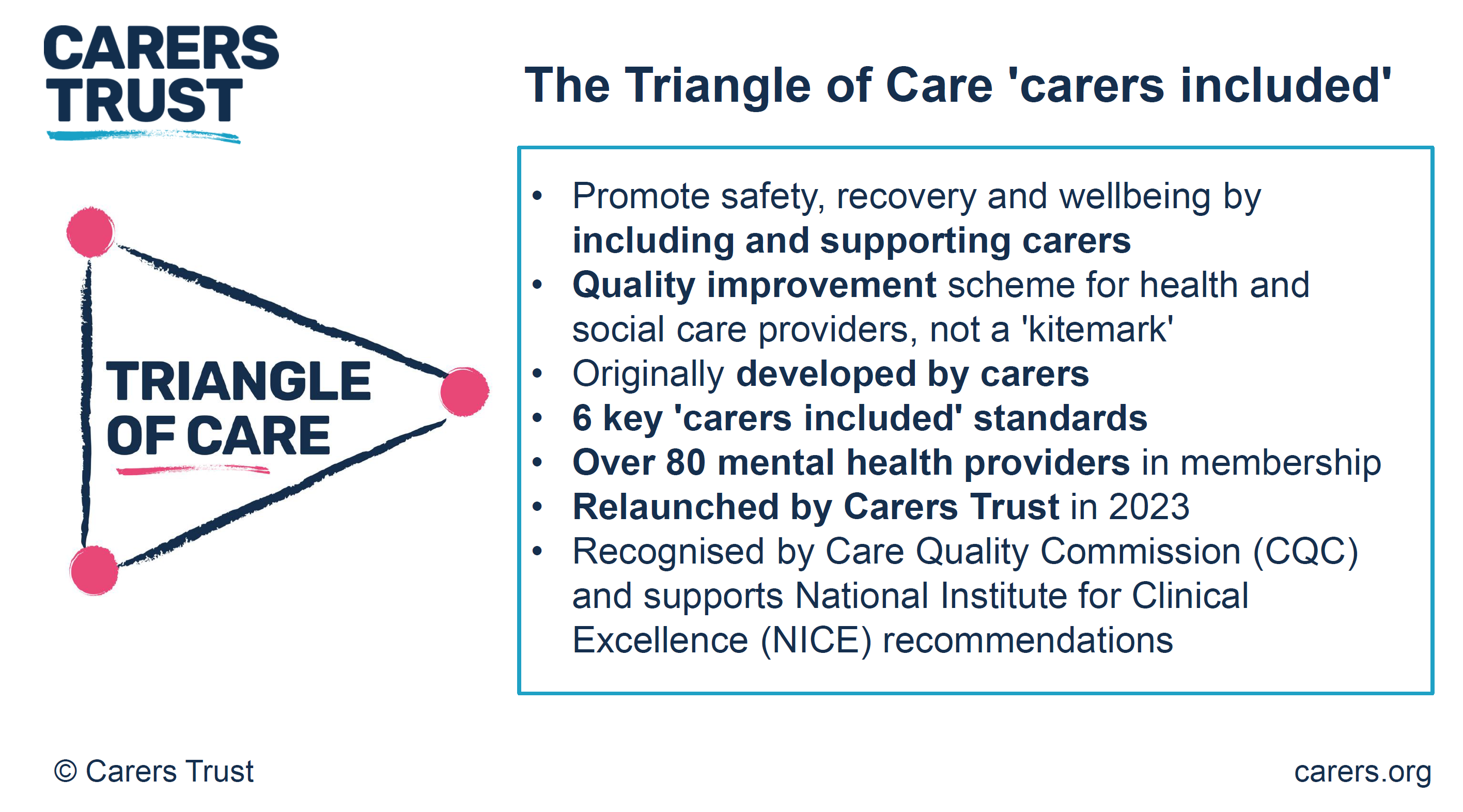
The Triangle of Care update focused on how the programme continues to evolve as a learning-led, improvement-focused framework rather than a compliance or inspection tool. Members were reminded that the Triangle of Care is designed to support services to reflect honestly on how well carers are recognised, involved, and supported, and to identify practical actions for improvement.
The update highlighted the growing maturity of the self-assessment and peer review process. Increasingly, organisations are using the framework not only to evidence good practice but to challenge themselves, learn from others, and embed carer partnership more consistently across teams and pathways.
Self-Assessment and Peer Review: What’s Working Well
The self-assessment process continues to be a key entry point for organisations engaging with the Triangle of Care. Where we were updated on how self-assessment encourages teams to pause and reflect on everyday practice, policies, and culture, rather than relying solely on written procedures. When combined with peer review, this reflection is strengthened by external challenge and lived-experience insight.
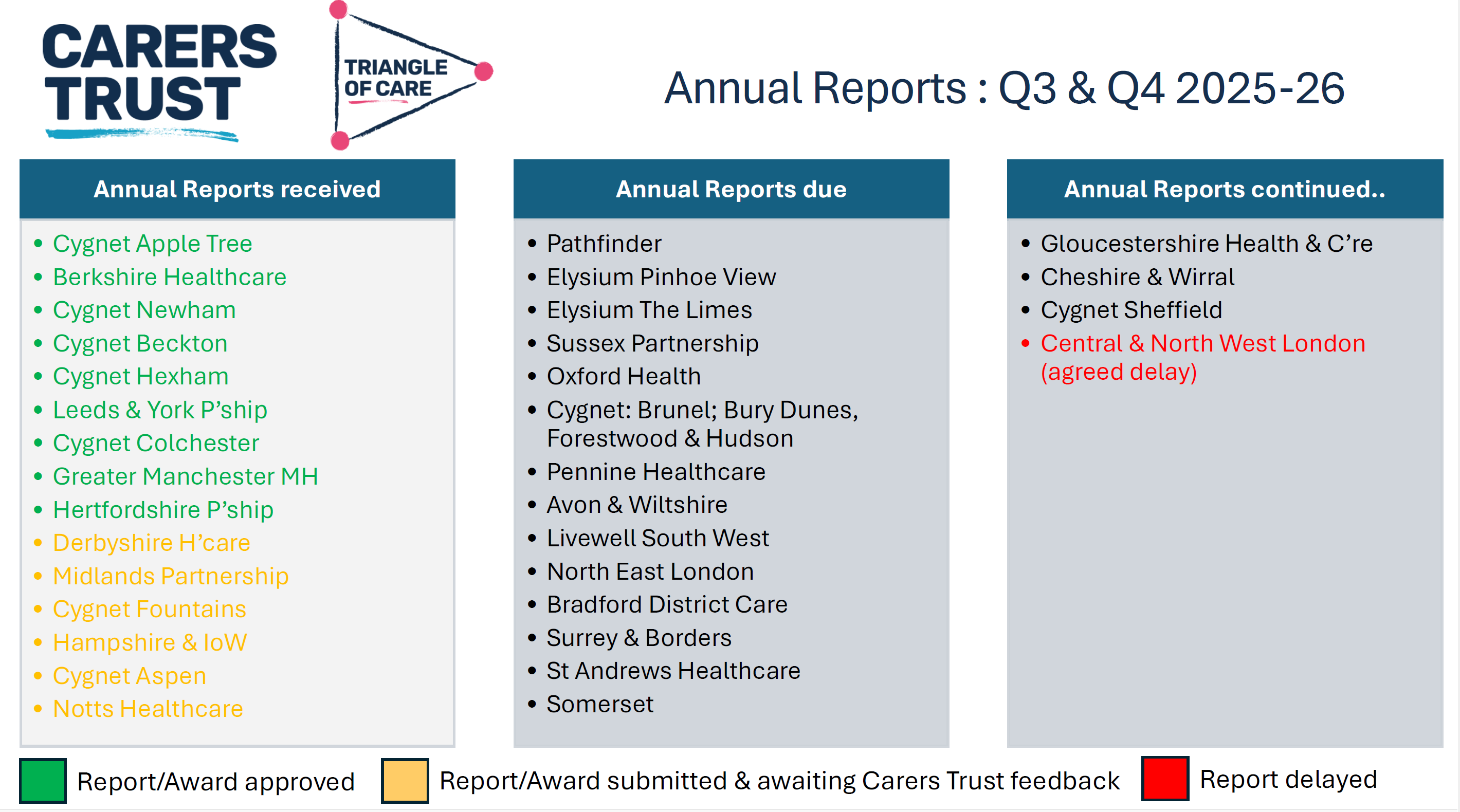
As part of the update, members were updated on emerging learning from Triangle of Care reports, including self-assessment submissions and peer review feedback. These reports were described as an important source of insight into how carer involvement is experienced on the ground, highlighting both areas of strong practice and recurring challenges across services
NOTE: These include reports going back 6 months, so not all NHS trusts listed
Peer review was described as most effective when organisations approach it with openness and curiosity. Lived-experience peer reviewers play a crucial role in asking different questions, highlighting blind spots, and grounding discussions in real-world carer experience.
A key discussion point was how to balance national consistency with local flexibility. Members acknowledged that while the Triangle of Care provides a shared framework and standards, services operate within different contexts, populations, and resource constraints.
Triangle of care and Patient Carer Race Equality Framework updates
The Triangle of Care and PCREF Phase 2 pilot will be launched in April 2026, to test co-produced specialist guidance to support integration of carers from racially marginalised communities into the Triangle of Care.
Alignment with Wider System Priorities
Members discussed how Triangle of Care activity aligns with broader system developments, including Mental Health Act reform, integrated care, and equality frameworks. There was strong agreement that Triangle of Care should not sit in isolation but be embedded within wider quality improvement, safeguarding, and workforce development agendas.
The need to visibly align Triangle of Care with the Patient and Carer Race Equality Framework was reiterated. Members emphasised that carers must be able to see how equality commitments translate into tangible actions within standards, training, and evidence.
Key points
Aligning Triangle of Care with Mental Health Act reform
Embedding within wider system and quality frameworks
Stronger visibility of equality and race equity
Carer Voice and Evidence of Impact
A recurring theme was the importance of demonstrating impact. Members discussed how services can better evidence carer involvement and experience beyond policies and training records. This includes qualitative feedback, lived-experience insight, and examples of how carer input has influenced service design and delivery.
Emerging Challenges and Areas for Development
The update also acknowledged ongoing challenges, including workforce pressures, digital transformation, and uneven awareness of the Triangle of Care across organisations. Members noted that carer involvement can become fragile during periods of change unless it is firmly embedded in systems and culture.
Summary: Where the Programme Is Heading
The Triangle of Care update concluded with a shared understanding that the programme is well-established but still evolving. The focus for the next phase is on deepening impact, strengthening alignment with equality and legislative change, and supporting services to move from intention to consistent, inclusive practice.
Key discussion points
Peer review as a developmental, learning-focused process
Balancing national consistency with local flexibility
Alignment with Mental Health Act reform and equality frameworks
Keeping carer voices central to assessment and review
3. Sharing Experiences as a Peer Reviewer
Carer involved with Avon & whitlshire
A carer presented from her involvement at Avon and Wiltshire Mental Health Partnership NHS Trust, where she is involved as a lived-experience peer reviewer contributing to Triangle of Care.
She shared reflections from her role as a lived-experience peer reviewer. She spoke about the importance of authenticity, trust, and transparency in the peer review process, and how lived experience strengthens both credibility and impact. Her contribution reinforced the value of co-production and highlighted how peer review can challenge assumptions, surface good practice, and promote more carer-inclusive cultures within organisations.
The discussion reinforced that organisational openness and leadership engagement are critical to turning peer review feedback into real change. Members reflected on how hearing directly from peer reviewers deepens understanding of the practical impact of policies on carers.
Q&A / Discussion
Members asked how organisations typically respond to lived-experience feedback.
The involved carer noted that openness and leadership support were key factors in whether reviews led to meaningful change.
Discussion reinforced the importance of preparing services for peer review so that carers feel genuinely welcomed and listened to.
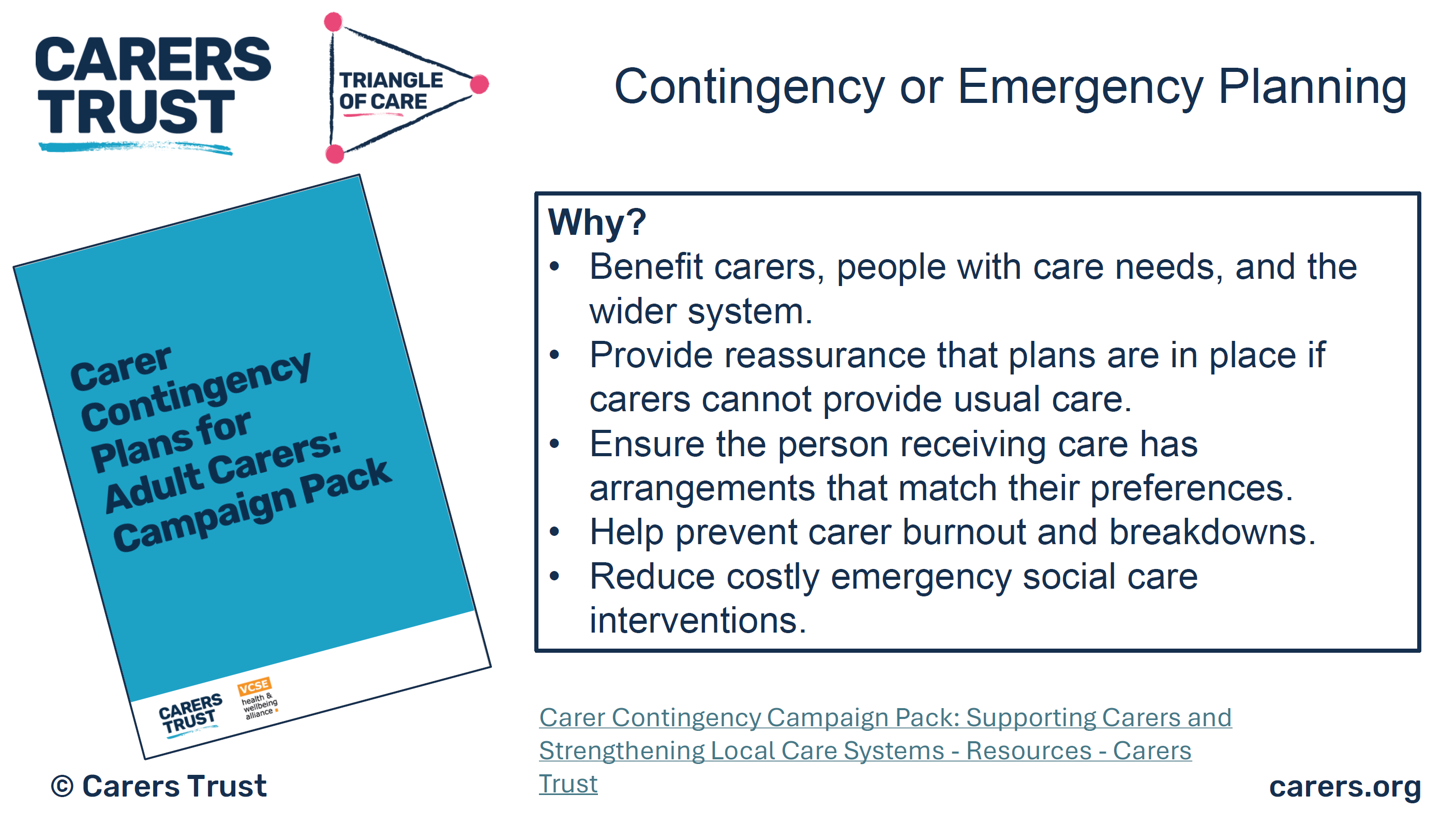
4. Carer Contingency Planning – Presentation and Local Practice
Mary Patel Local example: Carly Driscoll – Bradford District Care
This session focused on carer contingency planning as a key element of carer support and crisis prevention. The presentation outlined why contingency planning is critical in reducing carer anxiety, preventing emergency admissions, and ensuring continuity of care when carers are unable to continue their role.
Carer Contingency Planning (CCP), as championed by Carers Trust, is designed to support carers by planning ahead for times when they might suddenly be unable to continue caring. This might include illness, emergencies, hospitalisation, or other crises. CCP shifts the focus from reactive support during crisis moments to proactive planning that reduces anxiety and prevents avoidable breakdowns in care.
Carers Trust emphasises that CCP is a conversational, personalised process where the carer’s expertise is central. Carers know the routines, preferences, and cues that matter for the person they care for; the goal of CCP is to capture that knowledge in a way that can be shared quickly and effectively with services, families, and emergency responders when needed.
A local practice example from Bradford District Care demonstrated how contingency planning can work in practice, highlighting practical tools, partnership working, and engagement with carers. Discussion explored the benefits of clear, accessible plans, while also acknowledging challenges around awareness, consistency, and uptake
The local practice example demonstrated how contingency planning can be embedded into routine work through partnership approaches and proactive engagement with carers. Members discussed the importance of introducing plans early and reviewing them regularly.
Key features of the Bradford approach
Routine integration: CCP discussions happen early, not just in crisis moments
Partnership working: Health, social care, and voluntary sector staff work in concert
Accessible documentation: Plans are shared in forms that carers can use and update
Support for carers: Carers are supported to lead the planning, not be passive recipients
Ongoing review: Plans are revisited as needs and circumstances evolve
Benefits seen locally
Carers report feeling more confident and less anxious
Greater clarity across professionals when carers are unavailable
Fewer last-minute, unplanned crises or service escalations
Better use of local support networks when official services are stretched
Q&A / Discussion
Questions focused on how contingency plans are introduced to carers and reviewed over time.
Members raised concerns about low awareness of contingency planning among carers not already engaged with services.
Discussion highlighted the need for flexibility, recognising that carers’ circumstances can change rapidly.
5. Carer Contingency Planning – System Perspective
Sara Lewis – SW London ICB
Sara Lewis’s session focused on Carer Contingency Planning (CCP) as a core, preventative element of carer support rather than a reactive or optional add-on. CCP is a structured way of planning for what should happen if a carer is suddenly unable to continue caring due to illness, crisis, exhaustion, or an emergency. At its heart, CCP is about reducing uncertainty and anxiety for carers while ensuring continuity and safety for the person they support.
Sara emphasised that effective CCP recognises carers as partners with expert knowledge of the person they care for. The process supports carers to articulate what matters most, what routines and support are essential, and who needs to be contacted in an emergency. When done well, CCP helps prevent avoidable crises, emergency admissions, and breakdowns in care by making plans visible, accessible, and shared across relevant services.
Accessibility was a major theme, particularly the risks of digital exclusion. While digital tools can be effective, members stressed the need for non-digital options, language support, and culturally appropriate approaches to ensure equity.
Key Takeaways from Sara Lewis’s Session
Carer Contingency Planning is preventative, not reactive
CCP is built on early, ongoing conversations with carers
Plans should reflect what matters to carers and the cared-for person
CCP must be accessible, inclusive, and culturally appropriate
Digital tools can help, but must not increase exclusion
Successful CCP requires shared ownership across services
When embedded well, CCP reduces crisis, anxiety, and system pressure
Q&A / Discussion
Members questioned how to balance digital innovation with the risk of digital exclusion.
Language barriers and accessibility for carers with different communication needs were highlighted.
Discussion emphasised that contingency planning must be embedded into standard care planning processes, not treated as optional or additional.
6. Looking Ahead: Priorities for the Community Group
The “Looking Ahead” discussion focused on how the Triangle of Care Community Group can continue to influence meaningful change for carers in an evolving policy and practice landscape. Members reflected on the increasing complexity of health and care systems and the importance of ensuring that carers are not left behind as reforms, digital transformation, and workforce pressures accelerate.
A strong theme throughout the discussion was visibility, making carer involvement, equality, and partnership explicit in practice, evidence, and outcomes. Participants emphasised that carers must not only be recognised in principle but experience consistent involvement and support in real-world settings. The group agreed that the next phase of work should strengthen both strategic influence and practical implementation.
Mental Health Act Reform and Carer Involvement
Members discussed the implications of upcoming Mental Health Act reform, particularly around carers’ rights, information-sharing, and involvement in decision-making. There was recognition that Triangle of Care principles provide a strong foundation for supporting services to meet new expectations, but that further work will be needed to translate legislation into everyday practice.
The group highlighted the risk that carers could be inconsistently involved if workforce understanding is weak or if systems focus narrowly on legal compliance. Proactive guidance, training, and examples of good practice were seen as essential to ensure carers are meaningfully included rather than consulted as an afterthought.
Equality, Race Equity, and Inclusion
A central priority looking ahead is ensuring that Triangle of Care activity visibly aligns with the Patient and Carer Race Equality Framework (PCREF). Members stressed that carers from racialised and marginalised communities often face additional barriers to involvement, including mistrust, cultural misunderstandings, and unequal access to support.
The group agreed that equality must be embedded into standards, peer review evidence, and training—not treated as a parallel or optional agenda. This includes capturing meaningful data, listening to diverse carer voices, and ensuring culturally responsive practice is clearly demonstrated.
Workforce Training and Education
Workforce development was identified as a critical lever for long-term change. Members highlighted the need to strengthen carer awareness training across all roles, particularly for staff new to mental health and social care settings. Without this foundation, carer involvement remains inconsistent and dependent on individual attitudes rather than organisational culture.
There was strong support for influencing pre-registration education, including universities and training providers, to embed carer awareness earlier. This was seen as an opportunity to normalise partnership with carers from the start of professional careers rather than trying to retrofit it later.
Key points
Strengthening carer awareness across the workforce
Embedding Triangle of Care principles early in training
Influencing universities and pre-registration pathways
Moving from individual goodwill to system-wide culture change
Digital, Data, and Accessibility
Digital transformation featured prominently in the discussion, with members acknowledging both its potential and its risks. While improved data systems and digital tools can support information-sharing and coordination, there was concern that carers without digital access or confidence may be excluded.
Participants emphasised that digital solutions must be designed inclusively, with non-digital alternatives always available. Data collection should support understanding of carer experience and inequality, not become a barrier to support.
Key points
Digital tools should support, not replace, relationships
Risk of digital exclusion for some carers
Importance of non-digital alternatives
Using data to improve equity, not reinforce gaps
Young Carers and Marginalised Groups
Supporting young carers and carers from marginalised communities was highlighted as a continuing priority. Members noted that these groups are often under-identified and less likely to be involved in care planning or decision-making, despite carrying significant caring responsibilities.
The group agreed that future work should focus on visibility, early identification, and tailored approaches that recognise the specific needs and challenges faced by these carers. Partnership with education, community, and voluntary sector organisations was seen as essential.
Key points
Improving identification of young carers
Addressing barriers faced by marginalised carers
Tailored, age-appropriate and culturally sensitive support
Stronger partnership working beyond health services
Collective Commitment Moving Forward
The discussion concluded with a shared commitment to using the Community Group as a platform for influence, learning, and accountability. Members recognised the value of continuing to share practical examples alongside strategic discussion, ensuring that Triangle of Care principles are translated into everyday practice.
Looking ahead, the group aims to remain proactive, inclusive, and responsive—supporting services to recognise carers as equal partners and ensuring that no carer is left unseen or unsupported as systems evolve.
Key discussion points
Preparing for Mental Health Act reform
Embedding the Patient and Carer Race Equality Framework
Improving workforce training and education pathways
Supporting young carers and marginalised communities
Improving data and digital systems without exclusion
As Chair I thanked contributors and reaffirmed the importance of continued collaboration to ensure carers are recognised as equal partners in care, with Triangle of Care principles translated into meaningful practice across services.
For those interested to hear more about triangle of care, see details below
By Matthew McKenzie, facilitator of National ethnic mental health carers forum
Welcome to my first blog for 2026.
I am working on a new poetry project linked to my forum and poetry groups. This poem turned into song is written from the perspective of an unpaid ethnic mental health carer, and explores identity, pride, self-worth, and refusing shame in systems that don’t always listen or recognise lived experience.
The poem is taken from my forthcoming poetry book in development, Unpaid, Unseen and Yet Unbroken (due 2026), which centres the voices of ethnic mental health carers and aligns closely with the aims of PCREF (Patient and Carer Race Equality Framework), particularly around listening, inclusion, and lived experience shaping systems.
I’m using poetry and creative formats as another way to:
amplify carer voices
explore race and care with honesty
support conversations about equity, culture, and confidence in mental health services
If this resonates with your work, community, or organisation, please feel free to share. Listening is an act of care.
The recent Carers Forum brought together unpaid carers, health professionals, and community organisations from across South London to share updates, experiences, and ideas for improving mental health support. The event, chaired by Matthew McKenzie, created a safe and open space for carers to connect, exchange information, and have their questions heard by local health leaders.
Setting the Scene
Matthew opened the session by welcoming carers from across Lambeth, Lewisham, and Southwark. He spoke about the importance of providing carers with dedicated time to hear from service providers, particularly those supporting someone with mental ill-health and to ensure their voices shape local mental health strategies.
by Matthew McKenzie – National Ethnic Mental Health Carer Forum Chair
In August, the online National Ethnic Mental Health Carer Forum came together once again to confront difficult but necessary conversations about systemic racism, discrimination, and the experiences of ethnic minority carers within health and social care. The forum, hosted by Matthew McKenzie, provided a platform for carers, professionals, and researchers to share insights, frustrations, and plans for change.
Focus on Racism and Discrimination
This month’s forum was unflinching in its focus: racism in health and mental health systems. Attendees shared powerful testimonies of racial abuse and discrimination, highlighting how these experiences undermine trust in services and affect both carers and those they support. There was a clear call for honesty – participants stressed the importance of naming racism directly, rather than disguising it behind euphemisms.
The group also discussed the overrepresentation of Black and brown people in prisons, the lack of tailored initiatives for older Black carers, and the persistent inequalities faced by ethnic minority families trying to navigate mental health and social care support.
Research and Evidence from Carers Trust
A key presentation came from Andrew of Carers Trust, who shared research into the barriers faced by Black, Asian, and minoritised ethnic carers. The findings highlighted widespread issues: discrimination, language barriers, lack of cultural competence, and difficulties in accessing benefits. Andrew emphasised the need for culturally inclusive services and stronger outreach strategies, while acknowledging feedback from the forum that research and advocacy must be explicit about racism rather than avoiding the term.
Andrew expanded on the importance of equity in benefit advice, pointing out that many carers miss out on their entitlements because information is inaccessible, overly complex, or not communicated in culturally relevant ways. He called for dedicated advice services that are not only multilingual but also sensitive to carers who may not self-identify as such.
He also spoke about the impact of social isolation on carers from ethnic minority backgrounds, who often have fewer support networks and face stigma within their own communities. Addressing this requires building trust with local organisations and ensuring carer support is visible in spaces where communities already gather, such as faith centres or community hubs.
Finally, Andrew outlined the Carers Trust’s national strategy, which involves working more closely with local carer organisations, producing research that amplifies marginalised voices, and lobbying for systemic reforms. He highlighted how this forum’s feedback directly shapes their advocacy, showing a real commitment to partnership.
Questions raised during Carers Trust’s presentation:
How can Carers Trust ensure its research explicitly names racism rather than using softer language?
What specific support can be offered to carers who do not self-identify as carers and miss out on benefits?
How can Carers Trust improve its complaints handling processes, particularly for carers facing racism and discrimination?
What role can MPs and lobbying groups play in supporting Carers Trust’s advocacy for ethnic minority carers?
How will Carers Trust ensure its multilingual materials are distributed widely enough to reach isolated communities?
Hampshire & Isle of Wight NHS Anti-Racism Initiatives
Usually NHS Mental Health trust representatives update on anti-racism initiatives at the forum. This time Hampshire and Isle of Wight engaged with minority carers.
Elton who is the Diversity and Inclusion Partner from Hampshire and Isle of Wight NHS Trust provided an update on their anti-racist programmes, including the rollout of the Patient and Carer Race Equality Framework (PCREF). The trust has begun implementing cultural competence training, engaging with local communities, and embedding anti-racism into its wider mental health services. While early in its journey, the trust is already seeing changes in communication and engagement across different wards and services.
Elton shared that the trust is actively developing training modules on implicit bias, with the aim of reaching every staff member across its services. This training is intended not as a one-off exercise but as part of a sustained culture change programme. Early feedback from staff has been encouraging, with more frontline workers recognising how unconscious bias can influence treatment decisions.
He also described the trust’s efforts to engage directly with service users and carers, ensuring that their lived experiences feed into decision-making. Listening events, surveys, and advisory panels are being used to capture diverse perspectives, with a particular focus on groups who historically felt excluded from consultation.
In addition, Elton emphasised the need for transparency and accountability. The trust will publish regular updates on its PCREF action plan, allowing communities and stakeholders to scrutinise progress. He acknowledged that this is just the beginning, but stressed that embedding anti-racism into healthcare systems requires openness, humility, and sustained commitment.
Participants raised questions about how these initiatives address specific groups, such as older Black carers and prisoners’ families, as well as concerns about public misconceptions of anti-racism work. Elton acknowledged these challenges and committed to following up with colleagues on gaps raised during the discussion.
Questions raised during NHS Trust’s presentation:
How will PCREF specifically address the needs of older Black adults who often feel invisible in services?
What is being done to support the mental health of prisoners (e.g. Albany and Parkhurst prisons) and their families within this anti-racist framework?
How will the trust prevent the public misconception that PCREF “excludes” white people?
What mechanisms are in place to ensure transparency and accountability in publishing progress updates?
How will the trust measure the long-term impact of cultural competence and implicit bias training?
Academic Research Contributions
The forum also heard from Shylet, a PhD researcher from University of Glasgow, who is focusing on learning disabilities. She presented her work on the lived experiences of Black African families caring for adults with learning disabilities, and invited participants to take part in interviews. Their contributions highlighted the importance of academic research in documenting and amplifying carers’ lived realities.
Another important theme was the financial challenges facing carers. The group discussed the complexity of benefits like Carer’s Allowance and how misinformation or fear of losing other entitlements often deters carers from claiming support. A carer expressed reluctance to claim due to concerns about how it might affect their relative’s benefits, while another highlighted the importance of valuing one’s own contribution and recognising caring work. There was frustration with bureaucratic systems that seem designed to exclude, particularly when layered with the additional barriers of language, culture, and discrimination.
Carers also highlighted the immense value of unpaid care, with estimates placing its worth at over £180 billion per year if it were to be paid for by the NHS. This figure underscored the urgent need for better recognition and support of carers’ contributions.
Strengthening Complaints and Accountability
There was a debate around how carers can raise complaints when faced with racism or poor treatment. Many participants expressed a lack of trust in formal systems like the CQC or Ombudsman, feeling that complaints disappear into bureaucracy without change. Suggestions included working with MPs, lobbying groups, or the media to ensure voices are heard.
Final Reflections
The August forum showed once again how necessary it is to hold these difficult conversations. Carers spoke bravely about racism and exclusion, professionals shared updates on anti-racist strategies, and researchers sought to bring lived experience into policy. Yet the message was clear: systemic change requires more than frameworks and research reports. It requires honesty, collaboration, and persistence.
As host, I was encouraged by the passion and determination in the room. The forum continues to grow as a national voice for ethnic minority carers, and our commitment to addressing racism head-on remains at the heart of this work.
Caring for someone with long-term mental illness is a profound act of love and responsibility, just as i cared for my mother, but it is also fraught with emotional complexities, especially within culturally tight-knit communities. The experience of unpaid carers, those who provide care without financial compensation, can be shaped by powerful cultural expectations, traditions, and social pressures. These factors often lead to hidden challenges such as guilt and shame, which can create barriers to seeking help and support.
This blog post which is a transcript of my video explores the intricate dynamics of care guilt and shame, drawing on my insights as facilitator of the National Ethnic Mental Health Care Forum.
While the focus often falls on ethnic minority carers, many of the themes discussed I feel are universal, affecting unpaid carers from all backgrounds. However By examining the cultural ideals, emotional burdens, and systemic challenges faced by carers, we can better understand how to support them and promote positive change in mental health care.
The Role of Culture in Shaping the Carer Experience
Family Duty and Community Honor
In many tight-knit communities, caring for a family member is seen as a moral duty and a source of honor. The expectation is clear: “We look after our own.” This deeply rooted tradition fosters strong family bonds and a sense of belonging. The carer’s role is often defined by values handed down through generations, reinforcing the idea that caring is not just a responsibility but an essential part of one’s identity.
However, these cultural ideals can also create significant challenges. The notion that the “perfect carer never complains or needs help” sets an unrealistic standard, making it difficult for carers to express their struggles or seek support. Weakness is discouraged, and the pressure to cope without showing strain is especially pronounced among men, who may feel compelled to “man up” and avoid displaying vulnerability.
Keeping Illness Within the Family
Another common theme is the tendency to keep issues of ill health, particularly mental illness, within the family or community. This approach is often seen as a way to protect the family’s reputation and maintain social cohesion. Religious and cultural beliefs may further reinforce the idea that problems should be addressed privately, sometimes through prayer or spiritual practices, rather than seeking external help.
While these traditions can provide comfort and a sense of solidarity, they can also lead to isolation and prevent carers from accessing the support they need. The fear of gossip, judgment, or being seen as failing in one’s duty can be overwhelming, especially when mental health is stigmatized or misunderstood within the community.
The Emotional Weight of Caring: Guilt and Shame
How Guilt Creeps In
Guilt is a pervasive emotion among carers, particularly when cultural norms dictate that they should be able to handle all challenges alone. The demands of caring often mean missing out on community events, family gatherings, or social obligations. Community leaders or members may notice these absences and interpret them as letting the community down, adding to the carer’s sense of guilt.
This guilt can manifest in several ways:
Resentment and Frustration: Carers may feel frustrated with themselves or the person they are caring for, leading to emotional strain and potential conflict.
Personal Guilt: The belief that needing a break or personal time is selfish can prevent carers from prioritizing their own well-being, even when burnout is imminent.
Fear of Judgment: In large families or communities, the expectation to manage alone can be overwhelming. Carers may worry about being judged or seen as failing in their role.
The Catch-22 of Self-Care
The need for personal time and self-care is undeniable, yet carers often feel trapped in a catch-22. Taking time for themselves is viewed as selfish, but neglecting their own needs can have detrimental effects on their mental and physical health. The pressure to uphold cultural ideals and avoid showing weakness makes it difficult to break this cycle.
In some communities, there may not even be a word for “carer”—it is simply assumed that family members will step in as needed. This lack of recognition further compounds the challenges, as carers struggle to articulate their needs or seek validation for their efforts.
The Impact of Shame and Stigma
Saving Face and Avoiding Help
Shame is closely linked to guilt, and both emotions can prevent carers from reaching out for help. The desire to “save face” is strong in many communities, where reputation and social standing are highly valued. Admitting to struggles or accepting support may be seen as a sign of weakness or failure, leading carers to reject offers of assistance from mental health services or outreach programs.
Internalized comments such as “this is your duty,” “you must put up a front,” or “we don’t put family in care” reinforce the belief that seeking help is unacceptable. The fear of gossip and misunderstanding is real, especially in communities where mental health is poorly understood or lacks a cultural vocabulary.
Religious and Cultural Barriers
Religious identity can also play a role in shaping attitudes toward mental health and caring. In some faith-based communities, there may be little space for open discussion about mental illness, and spiritual solutions may be favored over professional support. This can create additional barriers for carers, who may feel unsupported or misunderstood by both their community and the wider mental health system.
Systemic Challenges: Inequalities in Mental Health Care
The Patient Care Race Equality Framework (PCREF)
Recognizing the unique challenges faced by minority carers, NHS England has developed the Patient Care Race Equality Framework (PCREF). These set of policies aims to tackle inequalities in mental health care, particularly for ethnic minority groups. The framework emphasizes the importance of breaking down guilt and shame, promoting better outcomes for minority communities, and ensuring that carers’ voices are central to service design and decision-making.
However, systemic barriers persist. Minority carers may be reluctant to engage with mental health services due to fears of poor outcomes, discrimination, or further isolation. The double tragedy is that those who need support the most are often the least likely to receive it, as both community and systemic factors conspire to keep them from seeking help.
The Importance of Carers’ Voices
A key focus of the National Ethnic Mental Health Care Forum is to ensure that carers’ voices are heard and valued. Too often, the emphasis is placed solely on patients or those with lived experience, overlooking the vital role that families and carers play. Guilt and shame can stop carers from engaging with services, making it essential for mental health systems to recognize and address cultural barriers.
Breaking the Cycle: Towards Better Support and Outcomes
Engaging with Communities
To break the cycle of guilt and shame, it is crucial to engage directly with communities. This means attending religious and cultural gatherings, listening to minority carers and patients, and understanding the specific struggles they face. Education is key!! both for carers and for mental health professionals. Training staff to appreciate community values and avoid assumptions about disengaged carers can help foster trust and collaboration.
Creating Safe, Non-Judgmental Spaces
Safe spaces where carers feel invited and heard are essential. These settings should be non-judgmental and designed to encourage open dialogue. Just like my Ethnic carer forum. Co-production, where patients and carers are involved in designing and delivering services and can help ensure that support is tailored to the needs of diverse communities.
Promoting Positive Role Models
Just as I mentioned when I spoke at the North East London NHS PCREF event, I feel that Role models play a powerful role in challenging stigma and inspiring change. Mental health trusts and systems should promote positive examples of carers who have reached out for help and benefited from support. Sharing stories and experiences can help others see that seeking help is not a weakness, but a strength.
Self-Care as Strength
Promoting self-care as a strength, rather than a weakness, is vital. Carers need to recognize that it is okay to ask for help and take time for themselves. Engaging with community leaders and faith networks can help change attitudes and reduce stigma, using trusted voices to advocate for better understanding and support.
The Path Forward: Building Inclusive Mental Health Services
Co-Production and Service Design
Including carers in service design and decision-making is essential for building inclusive mental health services. By putting carers at the center of policy and practice, systems can better address the unique challenges they face and promote positive outcomes for all.
Education and Awareness
Ongoing education and awareness-raising are critical. Carers, communities, and professionals must work together to challenge stigma, promote understanding, and create environments where everyone feels supported.
The Power of Conversation
Ultimately, breaking the cycle of care guilt and shame requires open conversation and a willingness to learn from each other. By sharing experiences, listening to diverse voices, and fostering empathy, we can build stronger, more inclusive communities and mental health systems.
Conclusion
Care guilt and shame are complex, deeply rooted issues that affect unpaid carers across culturally tight-knit communities. The emotional weight of caring, compounded by cultural expectations and systemic barriers, can lead to isolation, burnout, and reluctance to seek help. Addressing these challenges requires a multifaceted approach engaging with communities, promoting positive role models, creating safe spaces, and ensuring carers’ voices are central to service design.
By working together to challenge stigma and promote understanding, we can support carers in their vital role and build mental health services that truly meet the needs of all. The journey is ongoing, but with awareness, education, and compassion, positive change is possible.
Caring for someone with mental illness? Check out our Ethnic carer forum. Dates shown below.