If you’re an unpaid carer in Southwark, chances are you’re used to putting everyone else first. You support a loved one day in, day out, emotionally, practically, often invisibly. And too often, decisions about “support” for carers are made without carers truly being heard.
Southwark Council is developing its Unpaid Carers Strategy, and they are inviting unpaid carers to take part in upcoming focus groups to share real experiences, which are your lived reality.
As an unpaid carer myself, I know how rare and valuable this opportunity is.
Why having your say is important because
Policies and strategies shape:
What support is available
How easy (or hard) it is to access help
Whether carers feel recognised, supported, and understood
When carers don’t speak up, systems are built around us, not with us. When we do speak up, its a chance to make change becomes possible.
This isn’t about complaining. It’s about being honest: what works, what doesn’t, and what would genuinely make life easier for carers in Southwark.
Your voice could help shape:
Better access to information and services
More flexible, carer-friendly support
A strategy that reflects the real pressures carers face
A safe, non-judgemental space
One of the most important things about these focus groups is that they are designed to be:
Non-judgemental
Inclusive
Open to carers with any level of responsibility
You don’t need to have all the answers. You don’t need to be an “expert”. You just need your experience.
Whether you care full-time, part-time, occasionally, or don’t even label yourself as a “carer” your perspective still counts.
Focus group dates and details
In-person focus groups 📅 24th February ⏰ 11am – 1pmand2pm – 4pm 📍 Harriet Hardy Community Centre Harriet-Hardy Building, Aylesbury Estate, Albany Road, Walworth SE5 0AH
Online focus group 📅 25th February ⏰ 7pm 💻 Virtual session via Microsoft Teams
How to get involved
You can:
Scan the QR code on the flyer shown above my blog to register your interest
By Matthew McKenzie, A Caring Mind (Carers UK Ambassador)
As an unpaid mental health carer, I have spent years navigating hospital corridors, GP practices, care plans, juggling crises, and long silences where carers are too often left out. I am sure unpaid carers are expected to hold families together, while notice early warning signs, and keep loved ones safe. Still I always mention most of us receive no formal training, and our knowledge is rarely recognised as expertise.
That is why recently teaching a module for the Masters course to mental health nursing students at King’s College London felt so important. Not after they qualify. Not once they are overwhelmed in practice. But before they step out into the field. The session took place 15th of January.
Why carer-led teaching matters
Unpaid carers sit at the sharp edge of the mental health system. We see what works, what harms, and what gets missed when professionals don’t fully understand the family context. When students hear directly from carers, learning moves beyond textbooks into real life into the emotional, practical, and ethical realities of care.
Training mental health professionals without carer voices is like teaching navigation without a map.
What I taught: lived experience as learning
The session I delivered was built entirely from a carer’s perspective and centred on one core message: you cannot deliver effective mental health care without working with carers.
The module covered:
My lived experience as an unpaid mental health carer How I became a carer, the emotional impact, the daily responsibilities, and the toll caring can take on mental and physical health.
The hidden impact on carers Burnout, stigma, isolation, guilt, and the reality that many carers are supporting professionals while receiving little support themselves.
Carers as partners, not problems Exploring what happens when carers are ignored – and how outcomes improve when they are listened to, informed, and included.
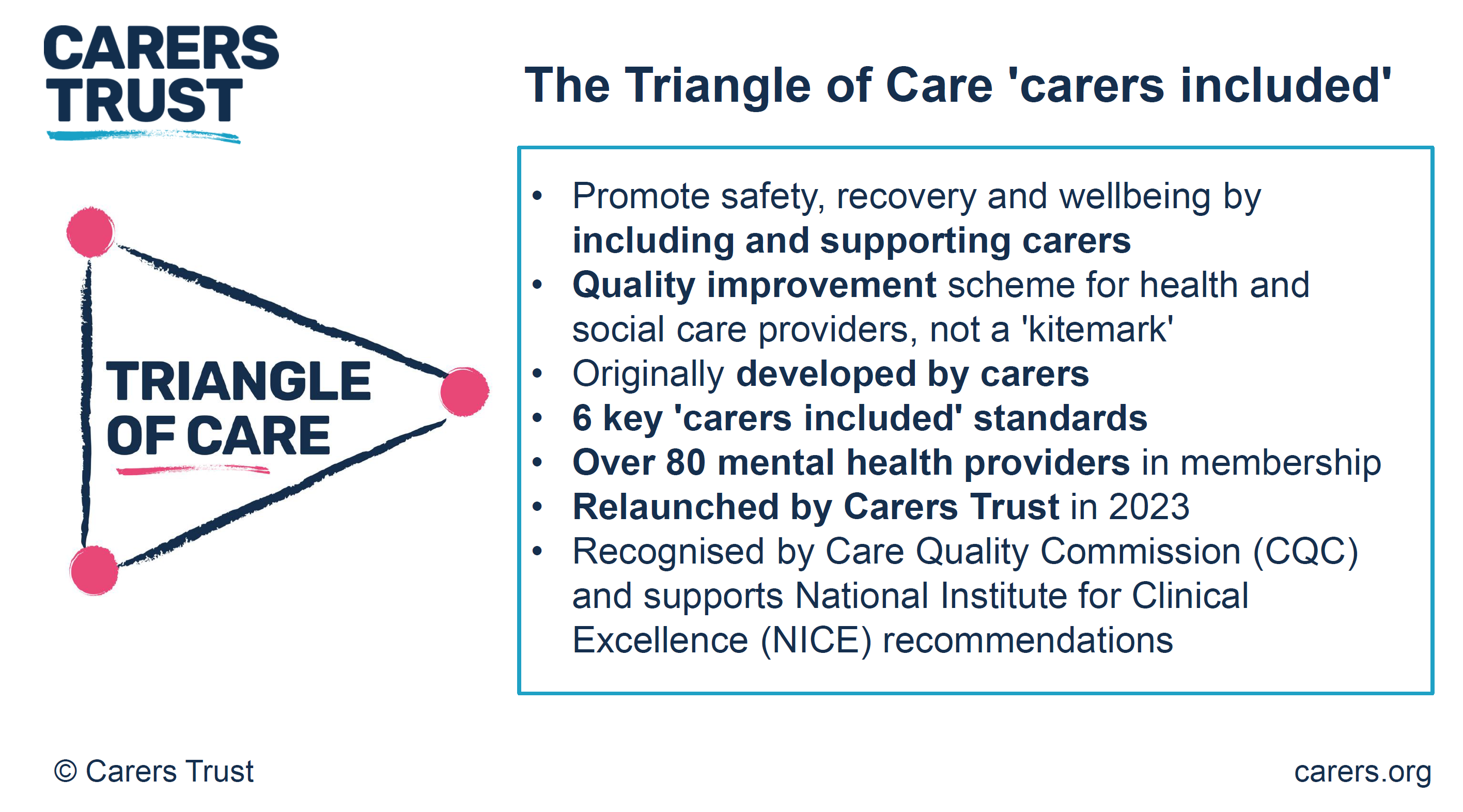
The Triangle of Care A strong emphasis on the Triangle of Care framework: the partnership between service user, carer, and professional. I challenged students to see carers as a vital link in the chain, not an optional extra.
Carers UK and carer identification Highlighting the role of Carers UK in advocacy, rights, resources, and why professionals must help carers identify themselves early so they can access support.
Practical skills for future nurses Listening without defensiveness, sharing information appropriately, involving carers in care planning, and understanding when carers need support themselves.
Interactive discussion and reflection Students worked through real-life scenarios, asking: What would I do differently now that I understand the carer experience?
The shift we need in education
Most unpaid carers are not trained for their role. We learn through crisis, exhaustion, and trial and error. Mental health professionals, however, are trained, which means universities have a responsibility to ensure that training includes those of us living this reality every day.
Carer-led teaching builds empathy, improves communication, and ultimately leads to safer, more effective care. When students learn early that carers matter, they carry that mindset into practice.
A final thought
Unpaid carers are already part of the mental health workforce, it’s just the title unpaid, unsupported, and often unheard. So I feel bringing carers into universities is not a “nice extra”. It is absolutely essential.
If we want a mental health system that truly works, we must start by listening to those who never clock off.
By Matthew McKenzie – Triangle of Care Community Chair.
The meeting opened with a welcome to carers, professionals, and partner organisations, reinforcing the importance of the Community Group as a collaborative and inclusive space. The Chair highlighted the ongoing commitment to co-production, ensuring that lived experience remains central to all Triangle of Care development and decision-making.
The purpose of the meeting was outlined, with emphasis on shared learning, constructive challenge, and influencing national work. Members were reminded that discussions within the group directly inform improvements to Triangle of Care standards, guidance, and implementation across services.
2. Triangle of Care Update (with Q&A)
Mary Patel – Carers Trust
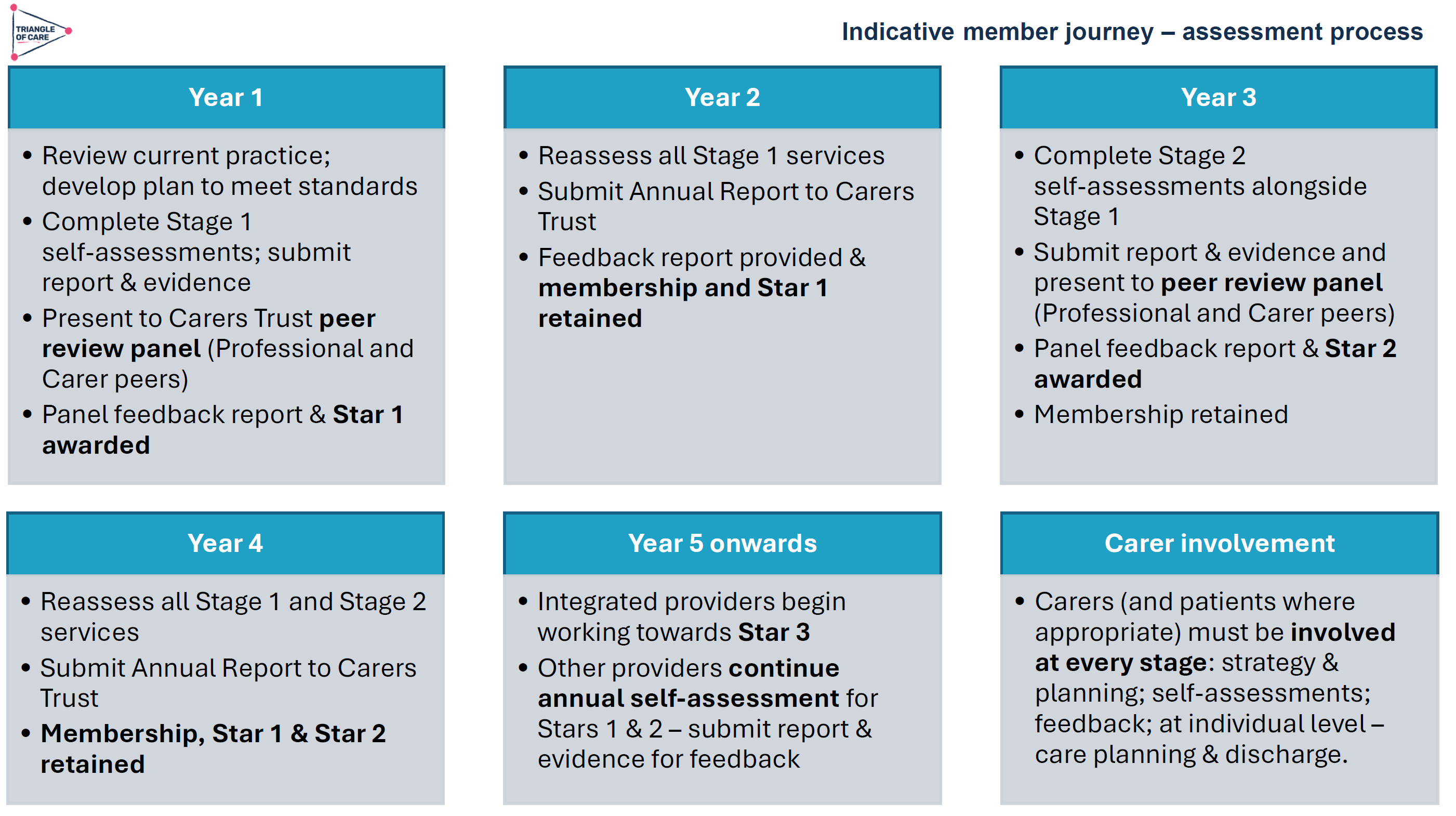
The Triangle of Care update focused on how the programme continues to evolve as a learning-led, improvement-focused framework rather than a compliance or inspection tool. Members were reminded that the Triangle of Care is designed to support services to reflect honestly on how well carers are recognised, involved, and supported, and to identify practical actions for improvement.
The update highlighted the growing maturity of the self-assessment and peer review process. Increasingly, organisations are using the framework not only to evidence good practice but to challenge themselves, learn from others, and embed carer partnership more consistently across teams and pathways.
Self-Assessment and Peer Review: What’s Working Well
The self-assessment process continues to be a key entry point for organisations engaging with the Triangle of Care. Where we were updated on how self-assessment encourages teams to pause and reflect on everyday practice, policies, and culture, rather than relying solely on written procedures. When combined with peer review, this reflection is strengthened by external challenge and lived-experience insight.
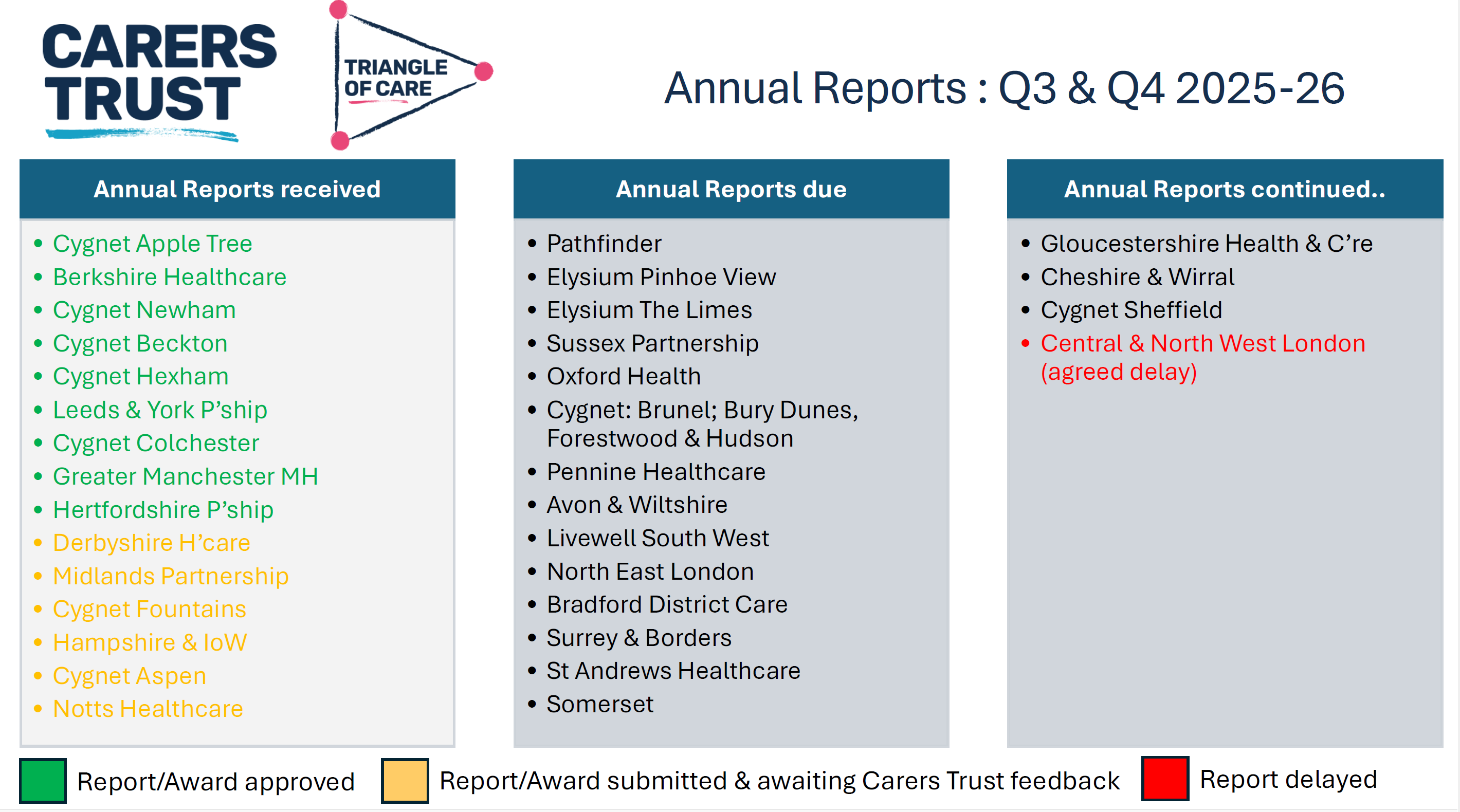
As part of the update, members were updated on emerging learning from Triangle of Care reports, including self-assessment submissions and peer review feedback. These reports were described as an important source of insight into how carer involvement is experienced on the ground, highlighting both areas of strong practice and recurring challenges across services
NOTE: These include reports going back 6 months, so not all NHS trusts listed
Peer review was described as most effective when organisations approach it with openness and curiosity. Lived-experience peer reviewers play a crucial role in asking different questions, highlighting blind spots, and grounding discussions in real-world carer experience.
A key discussion point was how to balance national consistency with local flexibility. Members acknowledged that while the Triangle of Care provides a shared framework and standards, services operate within different contexts, populations, and resource constraints.
Triangle of care and Patient Carer Race Equality Framework updates
The Triangle of Care and PCREF Phase 2 pilot will be launched in April 2026, to test co-produced specialist guidance to support integration of carers from racially marginalised communities into the Triangle of Care.
Alignment with Wider System Priorities
Members discussed how Triangle of Care activity aligns with broader system developments, including Mental Health Act reform, integrated care, and equality frameworks. There was strong agreement that Triangle of Care should not sit in isolation but be embedded within wider quality improvement, safeguarding, and workforce development agendas.
The need to visibly align Triangle of Care with the Patient and Carer Race Equality Framework was reiterated. Members emphasised that carers must be able to see how equality commitments translate into tangible actions within standards, training, and evidence.
Key points
Aligning Triangle of Care with Mental Health Act reform
Embedding within wider system and quality frameworks
Stronger visibility of equality and race equity
Carer Voice and Evidence of Impact
A recurring theme was the importance of demonstrating impact. Members discussed how services can better evidence carer involvement and experience beyond policies and training records. This includes qualitative feedback, lived-experience insight, and examples of how carer input has influenced service design and delivery.
Emerging Challenges and Areas for Development
The update also acknowledged ongoing challenges, including workforce pressures, digital transformation, and uneven awareness of the Triangle of Care across organisations. Members noted that carer involvement can become fragile during periods of change unless it is firmly embedded in systems and culture.
Summary: Where the Programme Is Heading
The Triangle of Care update concluded with a shared understanding that the programme is well-established but still evolving. The focus for the next phase is on deepening impact, strengthening alignment with equality and legislative change, and supporting services to move from intention to consistent, inclusive practice.
Key discussion points
Peer review as a developmental, learning-focused process
Balancing national consistency with local flexibility
Alignment with Mental Health Act reform and equality frameworks
Keeping carer voices central to assessment and review
3. Sharing Experiences as a Peer Reviewer
Carer involved with Avon & whitlshire
A carer presented from her involvement at Avon and Wiltshire Mental Health Partnership NHS Trust, where she is involved as a lived-experience peer reviewer contributing to Triangle of Care.
She shared reflections from her role as a lived-experience peer reviewer. She spoke about the importance of authenticity, trust, and transparency in the peer review process, and how lived experience strengthens both credibility and impact. Her contribution reinforced the value of co-production and highlighted how peer review can challenge assumptions, surface good practice, and promote more carer-inclusive cultures within organisations.
The discussion reinforced that organisational openness and leadership engagement are critical to turning peer review feedback into real change. Members reflected on how hearing directly from peer reviewers deepens understanding of the practical impact of policies on carers.
Q&A / Discussion
Members asked how organisations typically respond to lived-experience feedback.
The involved carer noted that openness and leadership support were key factors in whether reviews led to meaningful change.
Discussion reinforced the importance of preparing services for peer review so that carers feel genuinely welcomed and listened to.
4. Carer Contingency Planning – Presentation and Local Practice
Mary Patel Local example: Carly Driscoll – Bradford District Care
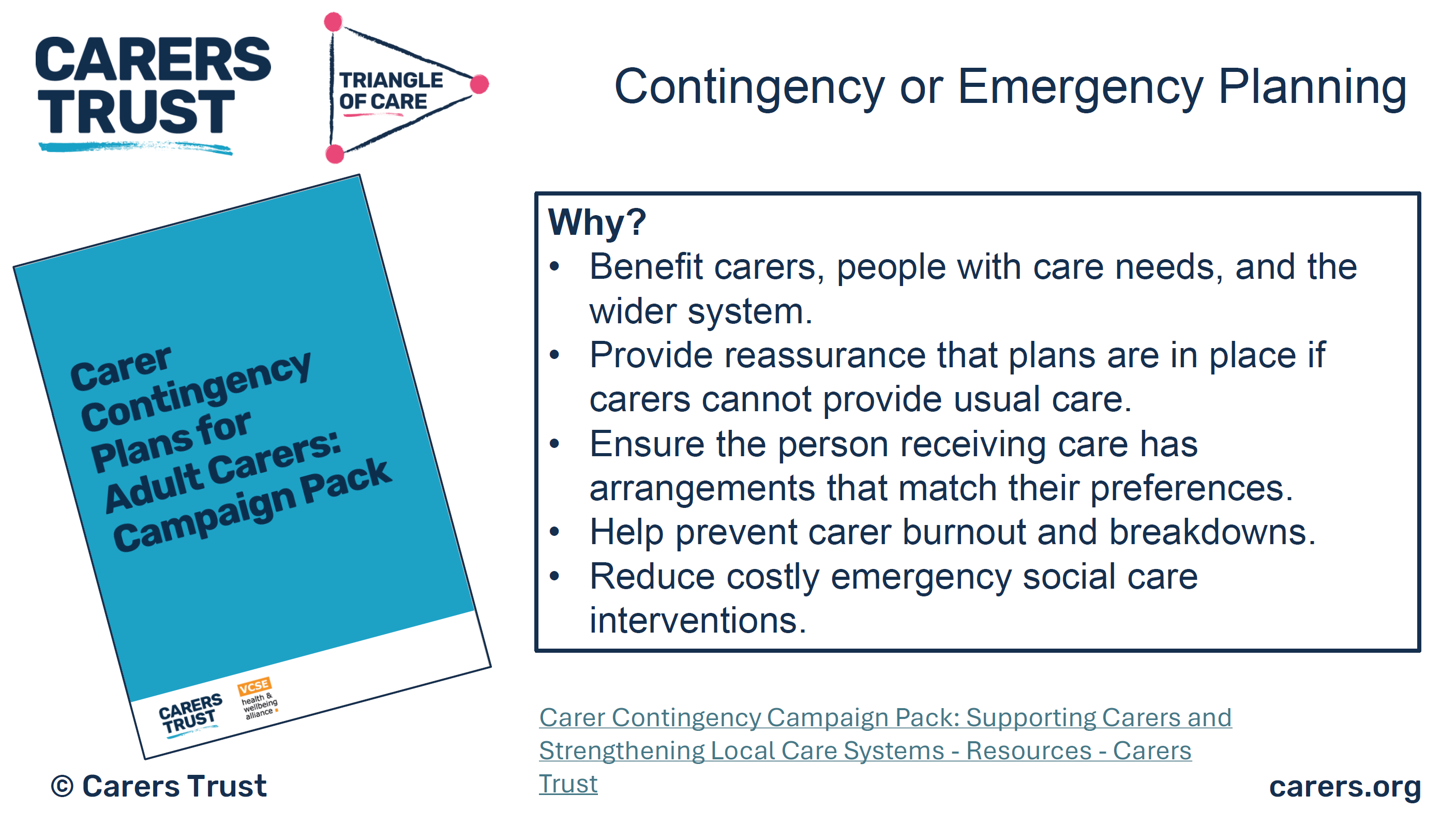
This session focused on carer contingency planning as a key element of carer support and crisis prevention. The presentation outlined why contingency planning is critical in reducing carer anxiety, preventing emergency admissions, and ensuring continuity of care when carers are unable to continue their role.
Carer Contingency Planning (CCP), as championed by Carers Trust, is designed to support carers by planning ahead for times when they might suddenly be unable to continue caring. This might include illness, emergencies, hospitalisation, or other crises. CCP shifts the focus from reactive support during crisis moments to proactive planning that reduces anxiety and prevents avoidable breakdowns in care.
Carers Trust emphasises that CCP is a conversational, personalised process where the carer’s expertise is central. Carers know the routines, preferences, and cues that matter for the person they care for; the goal of CCP is to capture that knowledge in a way that can be shared quickly and effectively with services, families, and emergency responders when needed.
A local practice example from Bradford District Care demonstrated how contingency planning can work in practice, highlighting practical tools, partnership working, and engagement with carers. Discussion explored the benefits of clear, accessible plans, while also acknowledging challenges around awareness, consistency, and uptake
The local practice example demonstrated how contingency planning can be embedded into routine work through partnership approaches and proactive engagement with carers. Members discussed the importance of introducing plans early and reviewing them regularly.
Key features of the Bradford approach
Routine integration: CCP discussions happen early, not just in crisis moments
Partnership working: Health, social care, and voluntary sector staff work in concert
Accessible documentation: Plans are shared in forms that carers can use and update
Support for carers: Carers are supported to lead the planning, not be passive recipients
Ongoing review: Plans are revisited as needs and circumstances evolve
Benefits seen locally
Carers report feeling more confident and less anxious
Greater clarity across professionals when carers are unavailable
Fewer last-minute, unplanned crises or service escalations
Better use of local support networks when official services are stretched
Q&A / Discussion
Questions focused on how contingency plans are introduced to carers and reviewed over time.
Members raised concerns about low awareness of contingency planning among carers not already engaged with services.
Discussion highlighted the need for flexibility, recognising that carers’ circumstances can change rapidly.
5. Carer Contingency Planning – System Perspective
Sara Lewis – SW London ICB
Sara Lewis’s session focused on Carer Contingency Planning (CCP) as a core, preventative element of carer support rather than a reactive or optional add-on. CCP is a structured way of planning for what should happen if a carer is suddenly unable to continue caring due to illness, crisis, exhaustion, or an emergency. At its heart, CCP is about reducing uncertainty and anxiety for carers while ensuring continuity and safety for the person they support.
Sara emphasised that effective CCP recognises carers as partners with expert knowledge of the person they care for. The process supports carers to articulate what matters most, what routines and support are essential, and who needs to be contacted in an emergency. When done well, CCP helps prevent avoidable crises, emergency admissions, and breakdowns in care by making plans visible, accessible, and shared across relevant services.
Accessibility was a major theme, particularly the risks of digital exclusion. While digital tools can be effective, members stressed the need for non-digital options, language support, and culturally appropriate approaches to ensure equity.
Key Takeaways from Sara Lewis’s Session
Carer Contingency Planning is preventative, not reactive
CCP is built on early, ongoing conversations with carers
Plans should reflect what matters to carers and the cared-for person
CCP must be accessible, inclusive, and culturally appropriate
Digital tools can help, but must not increase exclusion
Successful CCP requires shared ownership across services
When embedded well, CCP reduces crisis, anxiety, and system pressure
Q&A / Discussion
Members questioned how to balance digital innovation with the risk of digital exclusion.
Language barriers and accessibility for carers with different communication needs were highlighted.
Discussion emphasised that contingency planning must be embedded into standard care planning processes, not treated as optional or additional.
6. Looking Ahead: Priorities for the Community Group
The “Looking Ahead” discussion focused on how the Triangle of Care Community Group can continue to influence meaningful change for carers in an evolving policy and practice landscape. Members reflected on the increasing complexity of health and care systems and the importance of ensuring that carers are not left behind as reforms, digital transformation, and workforce pressures accelerate.
A strong theme throughout the discussion was visibility, making carer involvement, equality, and partnership explicit in practice, evidence, and outcomes. Participants emphasised that carers must not only be recognised in principle but experience consistent involvement and support in real-world settings. The group agreed that the next phase of work should strengthen both strategic influence and practical implementation.
Mental Health Act Reform and Carer Involvement
Members discussed the implications of upcoming Mental Health Act reform, particularly around carers’ rights, information-sharing, and involvement in decision-making. There was recognition that Triangle of Care principles provide a strong foundation for supporting services to meet new expectations, but that further work will be needed to translate legislation into everyday practice.
The group highlighted the risk that carers could be inconsistently involved if workforce understanding is weak or if systems focus narrowly on legal compliance. Proactive guidance, training, and examples of good practice were seen as essential to ensure carers are meaningfully included rather than consulted as an afterthought.
Equality, Race Equity, and Inclusion
A central priority looking ahead is ensuring that Triangle of Care activity visibly aligns with the Patient and Carer Race Equality Framework (PCREF). Members stressed that carers from racialised and marginalised communities often face additional barriers to involvement, including mistrust, cultural misunderstandings, and unequal access to support.
The group agreed that equality must be embedded into standards, peer review evidence, and training—not treated as a parallel or optional agenda. This includes capturing meaningful data, listening to diverse carer voices, and ensuring culturally responsive practice is clearly demonstrated.
Workforce Training and Education
Workforce development was identified as a critical lever for long-term change. Members highlighted the need to strengthen carer awareness training across all roles, particularly for staff new to mental health and social care settings. Without this foundation, carer involvement remains inconsistent and dependent on individual attitudes rather than organisational culture.
There was strong support for influencing pre-registration education, including universities and training providers, to embed carer awareness earlier. This was seen as an opportunity to normalise partnership with carers from the start of professional careers rather than trying to retrofit it later.
Key points
Strengthening carer awareness across the workforce
Embedding Triangle of Care principles early in training
Influencing universities and pre-registration pathways
Moving from individual goodwill to system-wide culture change
Digital, Data, and Accessibility
Digital transformation featured prominently in the discussion, with members acknowledging both its potential and its risks. While improved data systems and digital tools can support information-sharing and coordination, there was concern that carers without digital access or confidence may be excluded.
Participants emphasised that digital solutions must be designed inclusively, with non-digital alternatives always available. Data collection should support understanding of carer experience and inequality, not become a barrier to support.
Key points
Digital tools should support, not replace, relationships
Risk of digital exclusion for some carers
Importance of non-digital alternatives
Using data to improve equity, not reinforce gaps
Young Carers and Marginalised Groups
Supporting young carers and carers from marginalised communities was highlighted as a continuing priority. Members noted that these groups are often under-identified and less likely to be involved in care planning or decision-making, despite carrying significant caring responsibilities.
The group agreed that future work should focus on visibility, early identification, and tailored approaches that recognise the specific needs and challenges faced by these carers. Partnership with education, community, and voluntary sector organisations was seen as essential.
Key points
Improving identification of young carers
Addressing barriers faced by marginalised carers
Tailored, age-appropriate and culturally sensitive support
Stronger partnership working beyond health services
Collective Commitment Moving Forward
The discussion concluded with a shared commitment to using the Community Group as a platform for influence, learning, and accountability. Members recognised the value of continuing to share practical examples alongside strategic discussion, ensuring that Triangle of Care principles are translated into everyday practice.
Looking ahead, the group aims to remain proactive, inclusive, and responsive—supporting services to recognise carers as equal partners and ensuring that no carer is left unseen or unsupported as systems evolve.
Key discussion points
Preparing for Mental Health Act reform
Embedding the Patient and Carer Race Equality Framework
Improving workforce training and education pathways
Supporting young carers and marginalised communities
Improving data and digital systems without exclusion
As Chair I thanked contributors and reaffirmed the importance of continued collaboration to ensure carers are recognised as equal partners in care, with Triangle of Care principles translated into meaningful practice across services.
For those interested to hear more about triangle of care, see details below
Matthew McKenzie FRSA BEM, poet and advocate for unpaid ethnic mental health carers, is inviting carers involved in NHS Trusts, PCREF (Patient and Carer Race Equality Framework), and Trust involvement registers to submit their poems for an upcoming 2026 poetry collection. This collection will spotlight minority carers’ voices and explore themes of race, culture, and lived experience in mental health care.
About the Poetry Collection
The collection will focus on amplifying minority carers’ experiences through poetry. It will be part of the paperback version of Matthew’s upcoming poetry book Unpaid, Unseen and Yet Unbroken and will include poems from carers all over the country. This is a unique opportunity for minority ethnic carers to have their voices heard and their stories shared on a national platform, contributing to the ongoing conversation about race equality, care, and mental health.
Why Should You Submit a Poem?
If you’re a minority carer or carers from underrepresented community, your voice matters. PCREF is committed to creating systemic change, and this collection will work alongside it to ensure that carers from minority communities are not left unheard. Submitting your poem gives you the chance to:
Raise awareness of the emotional, cultural, and psychological realities of being a carer.
Inspire others by sharing your lived experience.
Amplify minority voices within NHS Trusts, PCREF spaces, and mental health care systems.
Who Can Submit?
We welcome submissions from unpaid ethnic mental health carers who are:
Involved in NHS Trusts, PCREF, or trust involvement registers.
Attending ethnic mental health carer peer groups at carer centres
Interested in sharing their personal experiences and reflections through poetry.
How to Submit Your Poem:
Submit an original poem that reflects the emotional, cultural, and psychological realities of being an unpaid mental health carer.
Poems can focus on themes such as:
Emotional challenges of care
The hidden burden of caring
Resilience and survival
Navigating mental health services
Coping with racial and cultural barriers in care
Family dynamics in caregiving
Deadline for submissions is late April 2026.
Submission Guidelines:
Format: Poems can be submitted in Word, PDF, or plain text format.
Length: There is no strict length, but we recommend that submissions be no longer than 1 page.
Multiple submissions: You can submit more than one poem if desired.
Contact Information: Please include your full name, contact details along with your poem, so i can credit you. Unless you wish to be anonymous.
You can also reach out to Matthew directly if you have any questions about the submission process or the collection.
What Happens After You Submit?
Once submissions are received, I will review all entries and select poems that align with the themes of the collection. All selected poets will be notified and credited in the final publication.
Need Inspiration or Support?
If you’re unsure where to start or need some encouragement, consider reflecting on your personal journey as a carer. Think about moments where language failed to express your experience or times when your strength surprised you. Your story is valuable, and this collection is about lifting up voices that have often been overlooked.
Contact Information:
For any questions or additional information, please contact Matthew McKenzie:
This is your chance to raise awareness and inspire others by sharing your lived experiences through poetry. Help shape a future where minority carers are valued, heard, and recognized for the essential work they do. We look forward to reading your stories!
On Thursday 20th November, I had the privilege of attending and speaking at the Memory, Wellbeing and Brain Health event hosted at Broadfield Community Centre in Crawley. Organised by Carers Support West Sussex, the event formed part of Carers Rights Day, bringing together carers, professionals, community teams, and people living with dementia for a day of learning, connection, and support.
Although I couldn’t stay for the full programme due to travelling to another Carers Rights Day engagement later that afternoon, I was grateful to take part in the early sessions and witness the energy and compassion that shaped the whole day.
By Matthew McKenzie – Cancer Carer forum Facilitator
Partnering for Better Outcomes – Reflections on My Latest RCN Blog
Supporting someone living with cancer is a journey filled with uncertainty, responsibility, and deep emotional commitment. As many carers know, much of this work happens quietly in the background. But every so often, there’s an opportunity to shine a light on the realities carers face and the vital partnerships that make a difference.
I’m proud to share that the Royal College of Nursing (RCN) recently invited me to contribute to their blog as part of a wider piece exploring how nurses support cancer caregivers. Written by Shannon Copeland (PhD researcher at Queen’s University Belfast), Partnering for better outcomes: How nurses support cancer caregivers highlights the evolving role of informal carers and the essential collaboration between families and nursing professionals.
In the blog, I shared my lived experience as an unpaid carer, the challenges, the emotional strain, and most importantly, the difference nurses can make when they recognise and support carers as part of the care team. Simple acts such as clear communication, continuity of support, and acknowledgment of a carer’s role can transform the caregiving experience.
Nurses often stand at the intersection of patient and carer needs. When they listen, guide, and empower carers, both patients and families benefit. I’m grateful to Shannon and the RCN for giving space to these conversations, and for highlighting the importance of carer voices in cancer care.
If you’re a carer, a nurse, or someone interested in improving cancer support, I encourage you to give it a read and join the discussion. Together, we can continue raising awareness of the carer journey and push for better recognition, resources, and collaboration across health and social care.
Walking into the RCN PSI Alumni Conference at Cowdray Hall on that crisp November morning, I felt a mix of pride, gratitude, and curiosity. It’s been many years since I first began speaking at RCN events like this, yet every time feels new because each gathering brings together nurses, carers, service users, and leaders who continue to shape the future of mental health care.
Before I continue to describe the event, let me sum up the Royal College of Nursing PSI programme. Basically the Psychosocial Interventions (PSI) programme is a nationally recognised training initiative designed to strengthen therapeutic skills of mental health professionals and embed recovery-focused, relationship-based care across services.
The PSI program is rooted in the principles of collaboration, reflection, co-production and empowerment, PSI equips practitioners with practical tools to support individuals experiencing mental distress, while also valuing the insight of carers and families.
I think what makes PSI stand out is its emphasis on seeing people beyond their diagnosis and fostering empathy, curiosity, and shared understanding between nurses, service users, and carers.
At the start of the conference and during it, I spoke to a few nurses over coffee, each reflecting on how PSI had shaped their practice one mental health nurse told me it had helped her “find her voice again.” For me, as a carer with lived experience, it was great to witness this sense of renewal. It reminded me why collaboration between professionals and lived experience communities is so essential.
Around 10 a.m., Catherine Gamble formally opened the event, setting a tone of gratitude and shared learning. Her introduction reminded us how much the alumni network had grown and how lived experience was now firmly part of the PSI culture.
As someone with lived experience of caring for my mum, who lived with schizophrenia, I approached the events not just as an observer but as someone deeply invested in the stories and struggles that bring us together as a triangle.
When I was invited to open the event and share my reflections as a carer, I knew I wanted to do more than talk about carers, I wanted to speak for them, and with them.
My Opening Talk – “The Nurses Who Walk With Us”
Standing at the podium, looking out at rows of passionate mental health nurses and lived experience, I began with gratitude. My words were simple but heartfelt:
“This is really about the nurses who walk with us, the ones who move beyond the labels, beyond the charts, and see the person, not the problem.”
I read a poem I had written to honour the compassion and resilience of those in the room a piece I called The Nurses Who Walk With Us.
The poem spoke about presence, about listening, and about the small acts of care that ripple into great change.
After my talk, I was moved by the warmth of the response. Many came up to share how my words mirrored their experiences or reminded them of why they came into nursing. That moment of connection that shared understanding set the tone for the day.
The Locksmiths Animation and Alumni Showcase
Following our opening session, Ellie Gordon and Stephen Jones launched the new animation “We Are the Locksmiths.” The film poetically portrayed mental health nurses as key-cutters shaping, adapting, and helping people find the right fit for recovery.
Watching it, I was struck by how accurately it captured the emotional labour of care, the balancing of vulnerability, patience, and professionalism
Next we had the Mentimeter session that morning, which was led by Professor Sally Hardy. She guided participants through reflective wellbeing questions using the interactive Mentimeter tool, encouraging everyone to think about how to sustain personal and professional wellbeing in mental health practice. Sally’s session wasn’t just about gathering feedback
Afterwards, the Alumni and Facilitators’ “Show and Tell Time” began. Groups from Sheffield NHS Trust, Sussex Mental Health Partnership, Lancashire Mental Health NHS trust, and Hereford NHS Trust sharing creative projects and reflections from their PSI practice. There were posters, poems, and community initiatives that had grown directly from the training. I wandered around the tables, speaking with participants who described how PSI had changed their teams. I think One mental health nurse told me, “We stopped seeing interventions as techniques and started seeing them as relationships.” It was inspiring
Workshop One – Working Together in Risk and Safety
After refreshments, we broke into workshops. I joined Workshop One: Lived Experience and Co-Production – Utilising Our Expertise, led by Hannah Cadogan and colleagues. It was energising to see lived experienced and mental health nurses working side by side.
I spoke about what co-production really means from a carer’s point of view. I shared my journey as someone who has cared for a family member living with schizophrenia and another with autism, and how those experiences taught me the importance of being included as an equal partner in care.
I explained that carers often hold a deep understanding of the person they support insights that can make a real difference if professionals take the time to listen and involve us from the start, not as an afterthought. Drawing on my work with Carers UK, the Carers Trust, and the Triangle of Care as many nurses from the mental health trusts were members of triangle of care programme., I spoke about how true co-production is built on trust, openness, and shared learning.
We discussed barriers time, fear, power differences but also solutions, like embedding co-production in supervision and reflective practice.
In this session, the discussion turned to how we can meaningfully involve carers and service users in planning safety not as tick-box exercises, but as genuine collaborations. I found myself reflecting on my own experiences of sitting in meetings where decisions were made about my mum rather than with us.
Hearing the nurses speak so openly about their challenges about time pressures, fear of getting it wrong, and the emotional toll of risk reminded me that we’re all human in this process. True co-production means sharing not only responsibility but also vulnerability.
One participant spoke about the importance of patience: “We’re not here to fix; we’re here to find a way in.” That line stayed with me. It echoed my own philosophy that care starts with listening, not solving.
By the end of the workshop, we agreed that co-produced safety isn’t about removing risk; it’s about building trust so we can face risk together.
Workshop Two – Co-Production and Carer Involvement
Lunch provided another opportunity for networking. The Mental Health Forum stand and MHP stall displayed resources on psychosocial practice.
I met others who had recently completed the course.
Conversations were open, curious, and full of mutual respect the kind of professional empathy that sustains hope in challenging work.
After lunch we heard from Professor Nicola Ranger, RCN General Secretary, who welcomed everyone back, commending the alumni for sustaining PSI’s legacy. Her words “you are the custodians of compassion” perfectly captured the spirit of the day.
The evaluation session of the RCN PSI Alumni Conference was presented in partnership with London South Bank University (LSBU), who have been key academic collaborators in examining the outcomes and long-term impact of the Psychosocial Interventions (PSI) programme. This section was introduced by Stephen Jones, and Professor Chris Flood, a leading figure in mental health nursing and research at LSBU.
Together, they outlined how LSBU’s evaluation seeks to capture not just the quantitative outcomes of PSI such as improved confidence and competence among practitioners but also the qualitative stories of change, growth, and compassion that the alumni community embodies.
There will be several teams at LSBU, but I was impressed on the make up of the Advisory and Supervisory Team provides academic oversight and strategic direction.
Professor Patrick Callaghan, Professor of Mental Health Science at LSBU, offers extensive expertise in psychosocial interventions and nursing research leadership.
Professor Chris Flood, a leading mental health and adult nurse researcher, specialises in health economics, survey design, and qualitative inquiry.
Professor Neil Brimblecombe, Professor of Mental Health and Learning Disability, contributes his expertise in workforce development, nurse prescribing, and policy analysis linking the PSI evaluation to broader NHS workforce strategies.
Professor Eddie Chaplin, an expert in intellectual disabilities and psychosocial interventions, supports the development of inclusive frameworks for peer support, guided self-help, and service co-production.
Afternoon workshop
In the afternoon, I attended Workshop Three: Working Together in Risk – Co-Production, Suicide and Personalised Safety. It was deeply emotional. We discussed how carers can be crucial in early warning and safety planning, but only if professionals create safe spaces for them to speak. The workshop was presented by Berkshire Healthcare NHS Foundation Trus
During the workshop, we took part in reflective exercises that encouraged us to consider what “shared safety” truly means. We were asked to think of times when communication broke down between families, patients and professionals, and how different outcomes might have been possible if trust and collaboration had been stronger.
Celebrating Archievements
Those who finished the RCN PSI programm were presented with a RCN PSI alumni badge, which i felt was a small but powerful symbol of commitment, compassion, and continued learning. For many, receiving that badge wasn’t just about completing a programme; it represented belonging to a network that values empathy, partnership, and the courage to keep improving mental health care together.
Reflections and Looking Ahead
As the day drew to a close, we took a quiet moment to reflect. Conferences like this are not just about learning they are about belonging. They remind me that, while the caring role can often feel isolating, there is a wider network of understanding and solidarity.
I missed out a lot more that took place at the alumni event, but watch out for more exciting news from the RCN in future.
To find out more about the RCN PSI Progamme, click link below.
By Matthew McKenzie, Facilitator, National Ethnic Mental Health Carer Forum
Introduction: A Forum that Connects and Challenges
As the facilitator of the National Ethnic Mental Health Carer Forum, I never take for granted how special these sessions are. Each month, carers, professionals, and researchers from all over the UK log in to share knowledge, raise awareness, and push for change in how mental health services understand and support ethnic minority communities.
Our October 2025 session was a powerful one. Falling on the last day of Black History Month, it brought together crucial themes on race equality, co-production, research, and carer visibility.
We heard from two key areas shaping mental health equity right now:
The OSMOSIS Project, led by Dr. Jacqueline Sin and Sharon Galliford, focusing on developing social care-based support for carers of people with psychosis.
The Patient and Carer Race Equality Framework (PCREF), presented by Aboobaker Bhana, Equality and Involvement Manager for South West Yorkshire Partnership NHS Foundation Trust.
By Matthew McKenzie – Carer activist with Think Tenacity Academy CIC at Nando’s High Street Kensington (Event held during Black History Month 2025)
A Warm Welcome and a Powerful Beginning
On Tuesday 28 October 2025 at Nando’s, 229 Kensington High Street.
As soon as I entered, the scent of grilled peri-peri wings mixed with the buzz of conversation. The event Making Time for Black Mental Health was hosted by Think Tenacity Academy CIC, led by founder Bella Rareworld.
The recent Carers Forum brought together unpaid carers, health professionals, and community organisations from across South London to share updates, experiences, and ideas for improving mental health support. The event, chaired by Matthew McKenzie, created a safe and open space for carers to connect, exchange information, and have their questions heard by local health leaders.
Setting the Scene
Matthew opened the session by welcoming carers from across Lambeth, Lewisham, and Southwark. He spoke about the importance of providing carers with dedicated time to hear from service providers, particularly those supporting someone with mental ill-health and to ensure their voices shape local mental health strategies.