By Matthew McKenzie, A Caring Mind (Carers UK Ambassador)
As an unpaid mental health carer, I have spent years navigating hospital corridors, GP practices, care plans, juggling crises, and long silences where carers are too often left out. I am sure unpaid carers are expected to hold families together, while notice early warning signs, and keep loved ones safe. Still I always mention most of us receive no formal training, and our knowledge is rarely recognised as expertise.
That is why recently teaching a module for the Masters course to mental health nursing students at King’s College London felt so important. Not after they qualify. Not once they are overwhelmed in practice. But before they step out into the field. The session took place 15th of January.
Why carer-led teaching matters
Unpaid carers sit at the sharp edge of the mental health system. We see what works, what harms, and what gets missed when professionals don’t fully understand the family context. When students hear directly from carers, learning moves beyond textbooks into real life into the emotional, practical, and ethical realities of care.
Training mental health professionals without carer voices is like teaching navigation without a map.
What I taught: lived experience as learning
The session I delivered was built entirely from a carer’s perspective and centred on one core message: you cannot deliver effective mental health care without working with carers.
The module covered:
My lived experience as an unpaid mental health carer How I became a carer, the emotional impact, the daily responsibilities, and the toll caring can take on mental and physical health.
The hidden impact on carers Burnout, stigma, isolation, guilt, and the reality that many carers are supporting professionals while receiving little support themselves.
Carers as partners, not problems Exploring what happens when carers are ignored – and how outcomes improve when they are listened to, informed, and included.
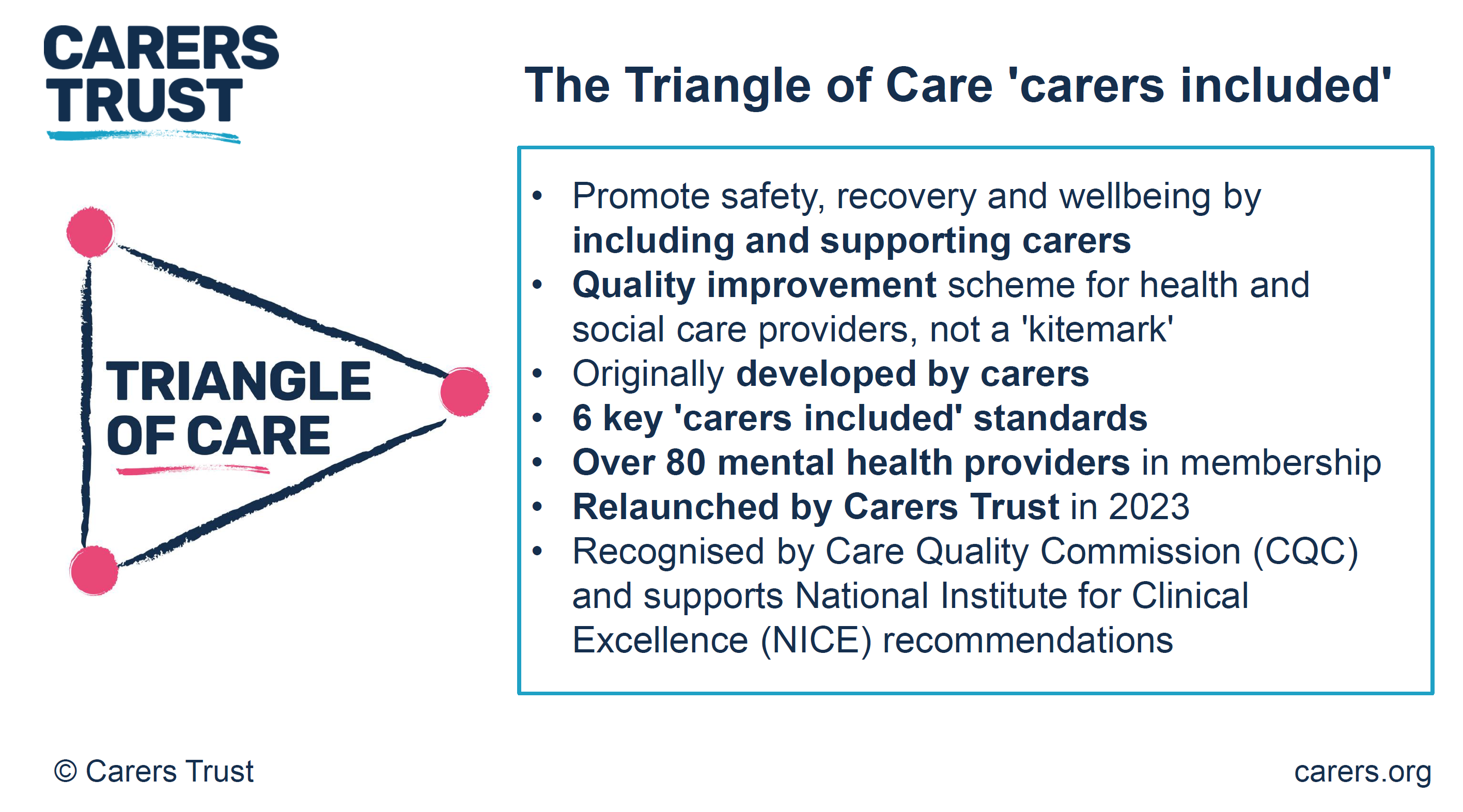
The Triangle of Care A strong emphasis on the Triangle of Care framework: the partnership between service user, carer, and professional. I challenged students to see carers as a vital link in the chain, not an optional extra.
Carers UK and carer identification Highlighting the role of Carers UK in advocacy, rights, resources, and why professionals must help carers identify themselves early so they can access support.
Practical skills for future nurses Listening without defensiveness, sharing information appropriately, involving carers in care planning, and understanding when carers need support themselves.
Interactive discussion and reflection Students worked through real-life scenarios, asking: What would I do differently now that I understand the carer experience?
The shift we need in education
Most unpaid carers are not trained for their role. We learn through crisis, exhaustion, and trial and error. Mental health professionals, however, are trained, which means universities have a responsibility to ensure that training includes those of us living this reality every day.
Carer-led teaching builds empathy, improves communication, and ultimately leads to safer, more effective care. When students learn early that carers matter, they carry that mindset into practice.
A final thought
Unpaid carers are already part of the mental health workforce, it’s just the title unpaid, unsupported, and often unheard. So I feel bringing carers into universities is not a “nice extra”. It is absolutely essential.
If we want a mental health system that truly works, we must start by listening to those who never clock off.
By Matthew McKenzie – Triangle of Care Community Chair.
The meeting opened with a welcome to carers, professionals, and partner organisations, reinforcing the importance of the Community Group as a collaborative and inclusive space. The Chair highlighted the ongoing commitment to co-production, ensuring that lived experience remains central to all Triangle of Care development and decision-making.
The purpose of the meeting was outlined, with emphasis on shared learning, constructive challenge, and influencing national work. Members were reminded that discussions within the group directly inform improvements to Triangle of Care standards, guidance, and implementation across services.
2. Triangle of Care Update (with Q&A)
Mary Patel – Carers Trust
The Triangle of Care update focused on how the programme continues to evolve as a learning-led, improvement-focused framework rather than a compliance or inspection tool. Members were reminded that the Triangle of Care is designed to support services to reflect honestly on how well carers are recognised, involved, and supported, and to identify practical actions for improvement.
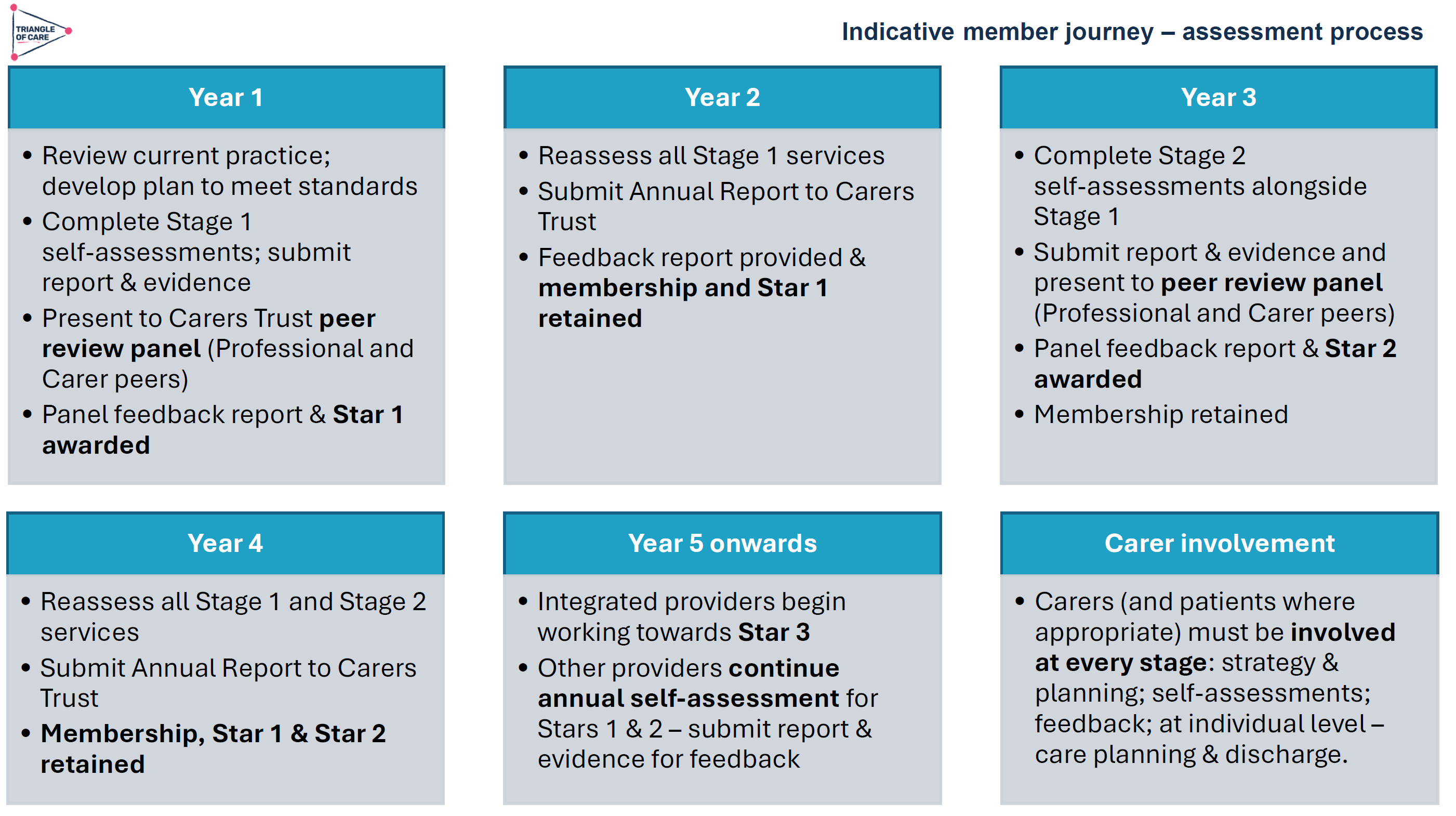
The update highlighted the growing maturity of the self-assessment and peer review process. Increasingly, organisations are using the framework not only to evidence good practice but to challenge themselves, learn from others, and embed carer partnership more consistently across teams and pathways.
Self-Assessment and Peer Review: What’s Working Well
The self-assessment process continues to be a key entry point for organisations engaging with the Triangle of Care. Where we were updated on how self-assessment encourages teams to pause and reflect on everyday practice, policies, and culture, rather than relying solely on written procedures. When combined with peer review, this reflection is strengthened by external challenge and lived-experience insight.
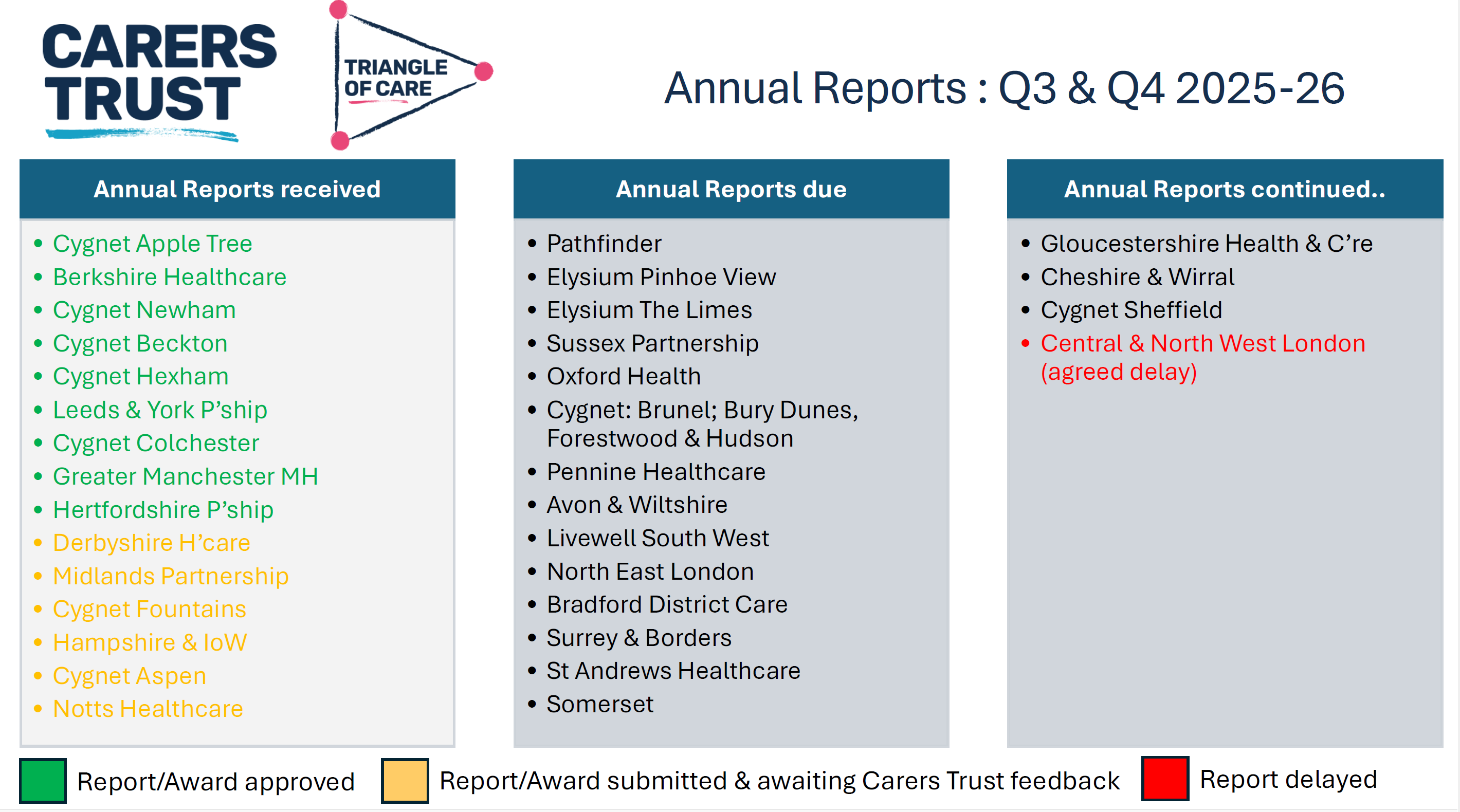
As part of the update, members were updated on emerging learning from Triangle of Care reports, including self-assessment submissions and peer review feedback. These reports were described as an important source of insight into how carer involvement is experienced on the ground, highlighting both areas of strong practice and recurring challenges across services
NOTE: These include reports going back 6 months, so not all NHS trusts listed
Peer review was described as most effective when organisations approach it with openness and curiosity. Lived-experience peer reviewers play a crucial role in asking different questions, highlighting blind spots, and grounding discussions in real-world carer experience.
A key discussion point was how to balance national consistency with local flexibility. Members acknowledged that while the Triangle of Care provides a shared framework and standards, services operate within different contexts, populations, and resource constraints.
Triangle of care and Patient Carer Race Equality Framework updates
The Triangle of Care and PCREF Phase 2 pilot will be launched in April 2026, to test co-produced specialist guidance to support integration of carers from racially marginalised communities into the Triangle of Care.
Alignment with Wider System Priorities
Members discussed how Triangle of Care activity aligns with broader system developments, including Mental Health Act reform, integrated care, and equality frameworks. There was strong agreement that Triangle of Care should not sit in isolation but be embedded within wider quality improvement, safeguarding, and workforce development agendas.
The need to visibly align Triangle of Care with the Patient and Carer Race Equality Framework was reiterated. Members emphasised that carers must be able to see how equality commitments translate into tangible actions within standards, training, and evidence.
Key points
Aligning Triangle of Care with Mental Health Act reform
Embedding within wider system and quality frameworks
Stronger visibility of equality and race equity
Carer Voice and Evidence of Impact
A recurring theme was the importance of demonstrating impact. Members discussed how services can better evidence carer involvement and experience beyond policies and training records. This includes qualitative feedback, lived-experience insight, and examples of how carer input has influenced service design and delivery.
Emerging Challenges and Areas for Development
The update also acknowledged ongoing challenges, including workforce pressures, digital transformation, and uneven awareness of the Triangle of Care across organisations. Members noted that carer involvement can become fragile during periods of change unless it is firmly embedded in systems and culture.
Summary: Where the Programme Is Heading
The Triangle of Care update concluded with a shared understanding that the programme is well-established but still evolving. The focus for the next phase is on deepening impact, strengthening alignment with equality and legislative change, and supporting services to move from intention to consistent, inclusive practice.
Key discussion points
Peer review as a developmental, learning-focused process
Balancing national consistency with local flexibility
Alignment with Mental Health Act reform and equality frameworks
Keeping carer voices central to assessment and review
3. Sharing Experiences as a Peer Reviewer
Carer involved with Avon & whitlshire
A carer presented from her involvement at Avon and Wiltshire Mental Health Partnership NHS Trust, where she is involved as a lived-experience peer reviewer contributing to Triangle of Care.
She shared reflections from her role as a lived-experience peer reviewer. She spoke about the importance of authenticity, trust, and transparency in the peer review process, and how lived experience strengthens both credibility and impact. Her contribution reinforced the value of co-production and highlighted how peer review can challenge assumptions, surface good practice, and promote more carer-inclusive cultures within organisations.
The discussion reinforced that organisational openness and leadership engagement are critical to turning peer review feedback into real change. Members reflected on how hearing directly from peer reviewers deepens understanding of the practical impact of policies on carers.
Q&A / Discussion
Members asked how organisations typically respond to lived-experience feedback.
The involved carer noted that openness and leadership support were key factors in whether reviews led to meaningful change.
Discussion reinforced the importance of preparing services for peer review so that carers feel genuinely welcomed and listened to.
4. Carer Contingency Planning – Presentation and Local Practice
Mary Patel Local example: Carly Driscoll – Bradford District Care
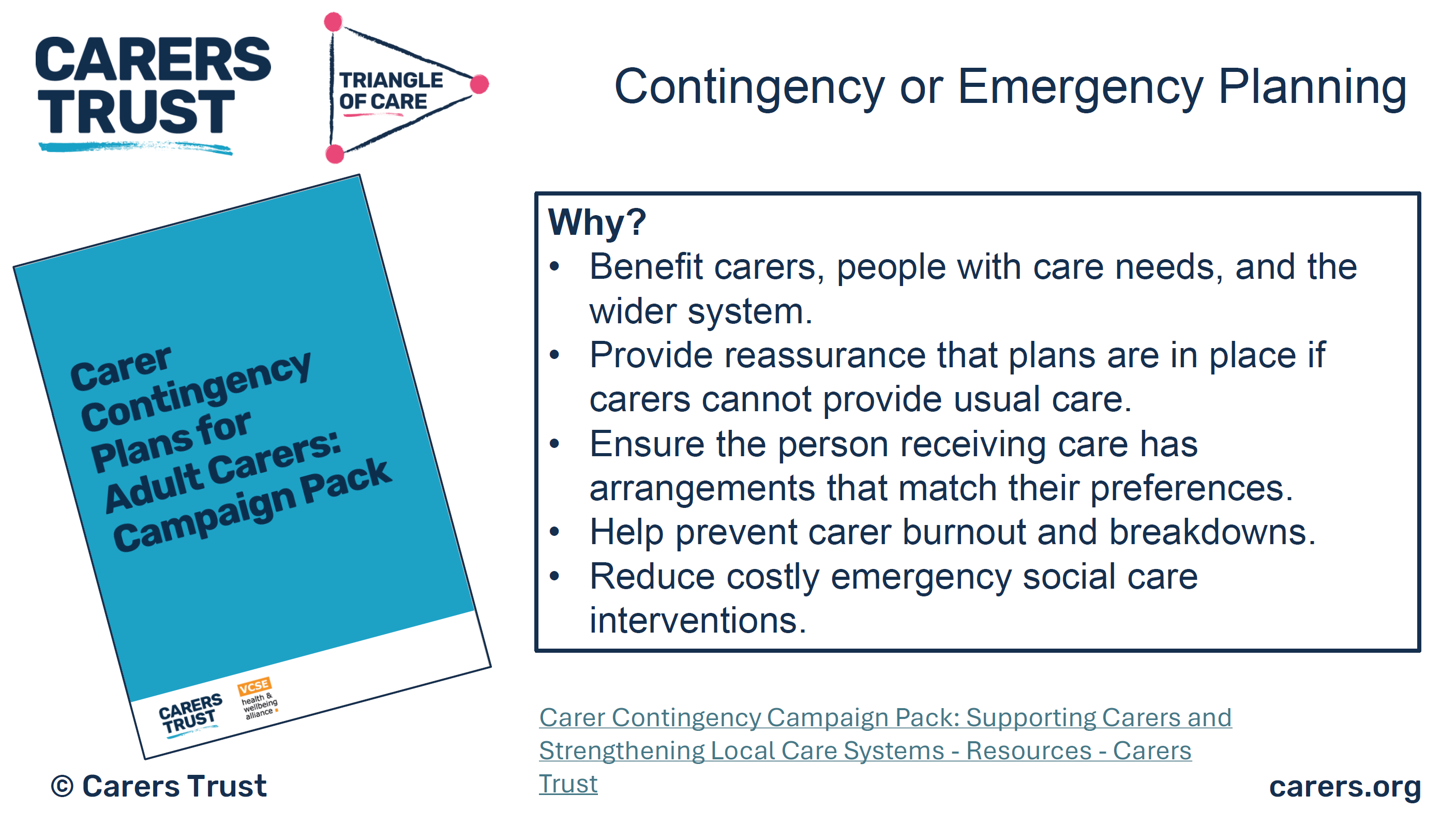
This session focused on carer contingency planning as a key element of carer support and crisis prevention. The presentation outlined why contingency planning is critical in reducing carer anxiety, preventing emergency admissions, and ensuring continuity of care when carers are unable to continue their role.
Carer Contingency Planning (CCP), as championed by Carers Trust, is designed to support carers by planning ahead for times when they might suddenly be unable to continue caring. This might include illness, emergencies, hospitalisation, or other crises. CCP shifts the focus from reactive support during crisis moments to proactive planning that reduces anxiety and prevents avoidable breakdowns in care.
Carers Trust emphasises that CCP is a conversational, personalised process where the carer’s expertise is central. Carers know the routines, preferences, and cues that matter for the person they care for; the goal of CCP is to capture that knowledge in a way that can be shared quickly and effectively with services, families, and emergency responders when needed.
A local practice example from Bradford District Care demonstrated how contingency planning can work in practice, highlighting practical tools, partnership working, and engagement with carers. Discussion explored the benefits of clear, accessible plans, while also acknowledging challenges around awareness, consistency, and uptake
The local practice example demonstrated how contingency planning can be embedded into routine work through partnership approaches and proactive engagement with carers. Members discussed the importance of introducing plans early and reviewing them regularly.
Key features of the Bradford approach
Routine integration: CCP discussions happen early, not just in crisis moments
Partnership working: Health, social care, and voluntary sector staff work in concert
Accessible documentation: Plans are shared in forms that carers can use and update
Support for carers: Carers are supported to lead the planning, not be passive recipients
Ongoing review: Plans are revisited as needs and circumstances evolve
Benefits seen locally
Carers report feeling more confident and less anxious
Greater clarity across professionals when carers are unavailable
Fewer last-minute, unplanned crises or service escalations
Better use of local support networks when official services are stretched
Q&A / Discussion
Questions focused on how contingency plans are introduced to carers and reviewed over time.
Members raised concerns about low awareness of contingency planning among carers not already engaged with services.
Discussion highlighted the need for flexibility, recognising that carers’ circumstances can change rapidly.
5. Carer Contingency Planning – System Perspective
Sara Lewis – SW London ICB
Sara Lewis’s session focused on Carer Contingency Planning (CCP) as a core, preventative element of carer support rather than a reactive or optional add-on. CCP is a structured way of planning for what should happen if a carer is suddenly unable to continue caring due to illness, crisis, exhaustion, or an emergency. At its heart, CCP is about reducing uncertainty and anxiety for carers while ensuring continuity and safety for the person they support.
Sara emphasised that effective CCP recognises carers as partners with expert knowledge of the person they care for. The process supports carers to articulate what matters most, what routines and support are essential, and who needs to be contacted in an emergency. When done well, CCP helps prevent avoidable crises, emergency admissions, and breakdowns in care by making plans visible, accessible, and shared across relevant services.
Accessibility was a major theme, particularly the risks of digital exclusion. While digital tools can be effective, members stressed the need for non-digital options, language support, and culturally appropriate approaches to ensure equity.
Key Takeaways from Sara Lewis’s Session
Carer Contingency Planning is preventative, not reactive
CCP is built on early, ongoing conversations with carers
Plans should reflect what matters to carers and the cared-for person
CCP must be accessible, inclusive, and culturally appropriate
Digital tools can help, but must not increase exclusion
Successful CCP requires shared ownership across services
When embedded well, CCP reduces crisis, anxiety, and system pressure
Q&A / Discussion
Members questioned how to balance digital innovation with the risk of digital exclusion.
Language barriers and accessibility for carers with different communication needs were highlighted.
Discussion emphasised that contingency planning must be embedded into standard care planning processes, not treated as optional or additional.
6. Looking Ahead: Priorities for the Community Group
The “Looking Ahead” discussion focused on how the Triangle of Care Community Group can continue to influence meaningful change for carers in an evolving policy and practice landscape. Members reflected on the increasing complexity of health and care systems and the importance of ensuring that carers are not left behind as reforms, digital transformation, and workforce pressures accelerate.
A strong theme throughout the discussion was visibility, making carer involvement, equality, and partnership explicit in practice, evidence, and outcomes. Participants emphasised that carers must not only be recognised in principle but experience consistent involvement and support in real-world settings. The group agreed that the next phase of work should strengthen both strategic influence and practical implementation.
Mental Health Act Reform and Carer Involvement
Members discussed the implications of upcoming Mental Health Act reform, particularly around carers’ rights, information-sharing, and involvement in decision-making. There was recognition that Triangle of Care principles provide a strong foundation for supporting services to meet new expectations, but that further work will be needed to translate legislation into everyday practice.
The group highlighted the risk that carers could be inconsistently involved if workforce understanding is weak or if systems focus narrowly on legal compliance. Proactive guidance, training, and examples of good practice were seen as essential to ensure carers are meaningfully included rather than consulted as an afterthought.
Equality, Race Equity, and Inclusion
A central priority looking ahead is ensuring that Triangle of Care activity visibly aligns with the Patient and Carer Race Equality Framework (PCREF). Members stressed that carers from racialised and marginalised communities often face additional barriers to involvement, including mistrust, cultural misunderstandings, and unequal access to support.
The group agreed that equality must be embedded into standards, peer review evidence, and training—not treated as a parallel or optional agenda. This includes capturing meaningful data, listening to diverse carer voices, and ensuring culturally responsive practice is clearly demonstrated.
Workforce Training and Education
Workforce development was identified as a critical lever for long-term change. Members highlighted the need to strengthen carer awareness training across all roles, particularly for staff new to mental health and social care settings. Without this foundation, carer involvement remains inconsistent and dependent on individual attitudes rather than organisational culture.
There was strong support for influencing pre-registration education, including universities and training providers, to embed carer awareness earlier. This was seen as an opportunity to normalise partnership with carers from the start of professional careers rather than trying to retrofit it later.
Key points
Strengthening carer awareness across the workforce
Embedding Triangle of Care principles early in training
Influencing universities and pre-registration pathways
Moving from individual goodwill to system-wide culture change
Digital, Data, and Accessibility
Digital transformation featured prominently in the discussion, with members acknowledging both its potential and its risks. While improved data systems and digital tools can support information-sharing and coordination, there was concern that carers without digital access or confidence may be excluded.
Participants emphasised that digital solutions must be designed inclusively, with non-digital alternatives always available. Data collection should support understanding of carer experience and inequality, not become a barrier to support.
Key points
Digital tools should support, not replace, relationships
Risk of digital exclusion for some carers
Importance of non-digital alternatives
Using data to improve equity, not reinforce gaps
Young Carers and Marginalised Groups
Supporting young carers and carers from marginalised communities was highlighted as a continuing priority. Members noted that these groups are often under-identified and less likely to be involved in care planning or decision-making, despite carrying significant caring responsibilities.
The group agreed that future work should focus on visibility, early identification, and tailored approaches that recognise the specific needs and challenges faced by these carers. Partnership with education, community, and voluntary sector organisations was seen as essential.
Key points
Improving identification of young carers
Addressing barriers faced by marginalised carers
Tailored, age-appropriate and culturally sensitive support
Stronger partnership working beyond health services
Collective Commitment Moving Forward
The discussion concluded with a shared commitment to using the Community Group as a platform for influence, learning, and accountability. Members recognised the value of continuing to share practical examples alongside strategic discussion, ensuring that Triangle of Care principles are translated into everyday practice.
Looking ahead, the group aims to remain proactive, inclusive, and responsive—supporting services to recognise carers as equal partners and ensuring that no carer is left unseen or unsupported as systems evolve.
Key discussion points
Preparing for Mental Health Act reform
Embedding the Patient and Carer Race Equality Framework
Improving workforce training and education pathways
Supporting young carers and marginalised communities
Improving data and digital systems without exclusion
As Chair I thanked contributors and reaffirmed the importance of continued collaboration to ensure carers are recognised as equal partners in care, with Triangle of Care principles translated into meaningful practice across services.
For those interested to hear more about triangle of care, see details below
Our final Triangle of Care (ToC) Community Group meeting of the year brought together carers, professionals, and ToC members from across the UK to share updates, raise concerns, and discuss priorities for 2026 and beyond. Although Microsoft Teams provided some surprises, we made it work, thanks to teamwork and patience. The conversation was rich, heartfelt, and often very moving.
1. Opening & Agenda
As chair of the meeting, I acknowledged technical teething problems as the group used Teams for the first time in this format. Mary (ToC Programme Lead) welcomed attendees and explained the privacy-driven decision to hide email addresses, which also unfortunately hid attendees’ names. A fix will be implemented before the January meeting.
The agenda included:
Triangle of Care national updates (Mary)
Carer co-production and lived experience input (Matthew)
Surrey & Borders’ co-production example (postponed)
Research priority-setting presentation (Richard, University of Manchester)
Carer questions and discussion
2. Triangle of Care National Update (Mary)
Mary provided a comprehensive end-of-year update structured around ToC’s three priority areas for 2024–25.
2.1 Embedding the Relaunched Triangle of Care Framework
Growth & progress
16 new members have joined the scheme since April, bringing ToC membership to over 80.
The first Welsh hospital achieved a ToC Star Award, prompting the creation of a new Welsh-language logo and Welsh materials.
A social care pilot is underway with Livewell South West, with West Hertfordshire Teaching Hospital reviewing ToC criteria for an acute setting.
Nine Star Awards have been achieved this year, with a further 12 annual reviews approved. Many more annual reports are pending review before year-end.
Standardising data Mary emphasised the push for consistent reporting across Trusts, including:
numbers of carers identified
uptake of carer awareness training
numbers of carer champions
This will help build a national picture of impact.
Webinars ToC’s Lunch & Learn series continues, with the recent Carers Rights Day webinar (in partnership with University of Bristol) focusing on the Nearest Relative role under the Mental Health Act (MHA). Resources are available via Carers Trust’s YouTube channel.
2.2 Young Carers: Identification & Support
A major update was the successful national policy win relating to young carers and the Mental Health Act.
Mental Health Act Reform – Safety Net for Young Carers
Following campaigning by Carers Trust, the Young Carers Alliance, and ToC members who wrote to MPs:
Government has agreed to update the MHA Code of Practice to require:
identification of children when an adult is detained
sharing of information about available support
referrals for young carer needs assessments
Updates to advance choice documents will require practitioners to ask about dependent children.
Expected implementation: Summer 2026.
This win was warmly welcomed by the group.
2.3 Racially Minoritised Carers & PCREF
Mary updated members on ToC’s work to ensure carers are fully represented in the Patient & Carer Race Equality Framework (PCREF).
Key updates
A national Task & Finish Group has now completed its review of the first four ToC standards; the final standard is underway.
Piloting of new culturally sensitive criteria is planned with 10 NHS Trusts beginning April 2026.
Example of early good practice: Livewell South West is implementing a new “essential data template” that includes carers, enabling services to better identify and support racially minoritised carers.
Carers Trust is calling for a statutory duty for NHS mental health providers to implement PCREF in full, including community governance.
2.4 Changing the Narrative on Care – New Research
Mary introduced new research (supported by the Health Foundation and Oxfam GB) titled Changing the Narrative on Care, highlighting:
Although 80% of the public value unpaid care, this does not translate into policy action or investment.
Three recommended reframes:
Care is a universal experience, not a niche issue.
No care without support, make support visible and tangible.
Care is a partnership between families, communities and systems—not something families must do alone.
The full report is available on Carers Trust’s website.
I then presented an in-depth reflection on the value of authentic carer involvement, drawing on his lived experience and his role working with multiple NHS organisations.
Key points included:
Carers are not passive observers, they hold critical lived knowledge that improves services.
Real co-production goes beyond consultation; carers must be equal partners in shaping policy, documentation, training, and strategic decisions.
Examples Matthew gave from his own involvement:
redesigning welcome packs and leaflets
addressing confidentiality misapplication
involvement in recruitment panels
delivering training to staff at induction
reviewing complaints and compliments themes
advising on discharge processes and family-inclusive safety protocols
participating in research steering groups
Carers’ insight is especially essential in safeguarding, quality boards, and identifying service gaps often invisible to professionals.
4. Surrey & Borders Co-Production Example
A planned presentation from Surrey & Borders was postponed, as the relevant colleague could not attend with materials. They hope to present at a future meeting.
5. Research Priority Setting in Secure & Forensic Mental Health (Richard Kears)
Richard introduced a national project with the James Lind Alliance (JLA) aiming to identify the top 10 research priorities for secure and forensic mental health services across England, Scotland and Wales.
Who is the survey for?
Carers
People with lived experience of secure/forensic services
Staff working in these services
Anyone indirectly connected (victims, families)
Purpose
To ensure future mental health research is led by the real concerns of those most affected, not only by academics or pharmaceutical interests.
Process
National survey gathering research questions.
Analysis to identify common themes.
Second, more focused survey to refine priorities.
National workshops with carers, staff and people with lived experience to finalise the top 10.
A QR code and flyer were shared for distribution. The group expressed strong support.
6. Attendee Discussion & Questions
This was the richest section of the meeting, with many heartfelt contributions. The themes below reflect the key concerns raised.
6.1 Scotland & UK-wide ToC Alignment
A carer asked why Scotland’s ToC framework is separate and not integrated into the UK ToC accreditation model. Mary explained:
Scotland currently uses ToC only as a free policy framework.
Implementing the accreditation model in Scotland would require groundwork to assess willingness and ability of providers to fund membership.
Integration is being discussed but is not imminent.
6.2 Clarity on Co-Production
Several carers voiced concerns that:
“Co-production” is often used as a buzzword.
Some NHS Trusts label work as co-produced after completing it.
Carers need clarity on what ToC means when using the term.
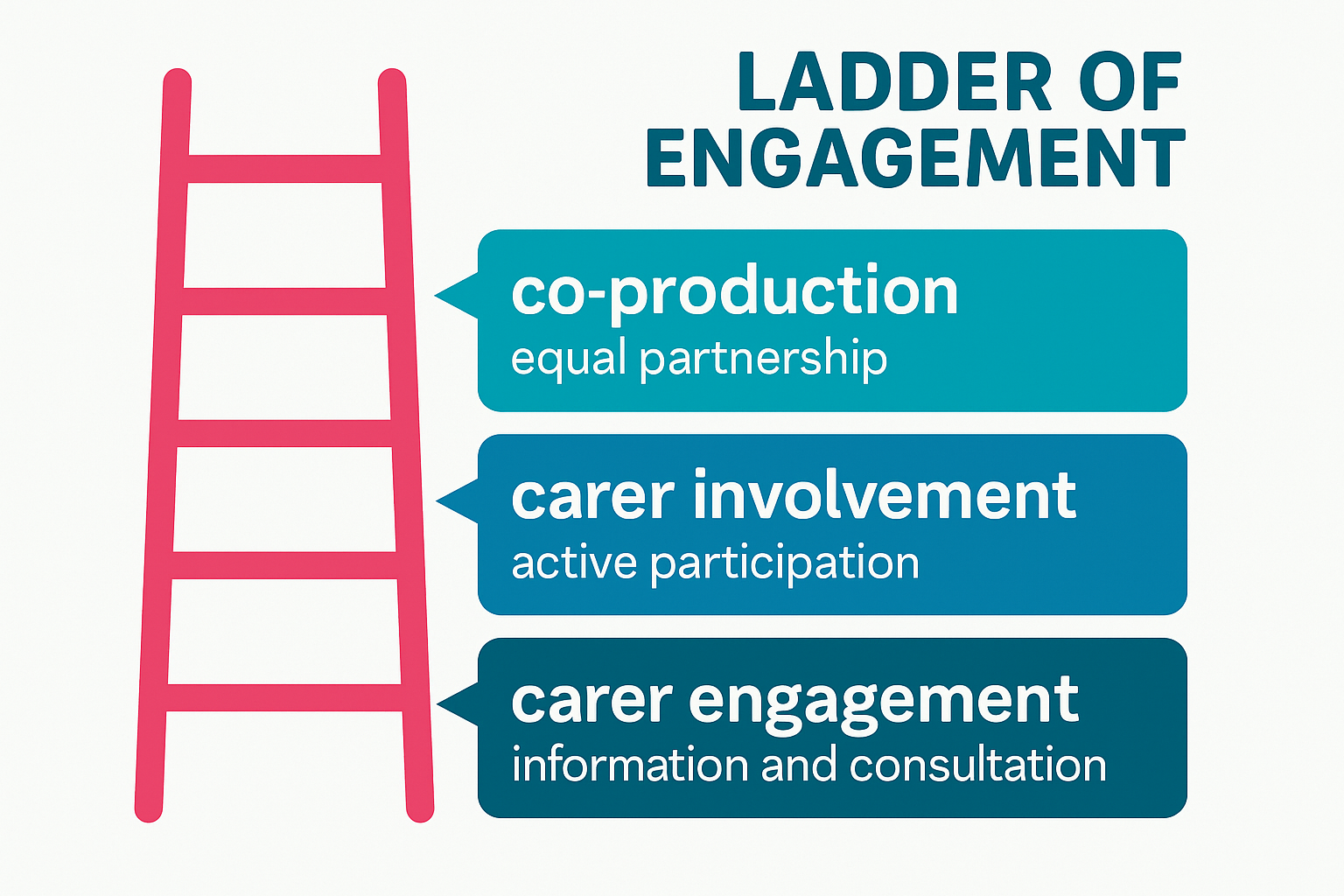
Mary responded that ToC uses a ladder of engagement, distinguishing:
carer engagement
carer involvement
full co-production
Carers Trust is developing a formal principles-based statement on involvement for future meetings.
6.3 Older Carers: Visibility, Support & Inequalities
The majority of carer questions focused on the unmet needs of older adult carers, many of whom are supporting people with severe mental illness—not dementia—and often have been caring 20–40 years.
Attendees reported:
Feeling “invisible” within both policy and services.
Being incorrectly grouped under “older carers = dementia”.
Their own poor health affecting their caring ability.
Increasing struggle to get responses from professionals.
Serious concerns about who will care for their loved ones when they die.
Feeling less heard as they age, compared with younger carers or newer voices.
One carer (age 78) shared:
“I can’t retire from caring. Benefits stop at 65, but the caring doesn’t.”
Another said:
“We have to shout louder as older women to be heard—and still we aren’t.”
Mary acknowledged the seriousness of these issues and committed to:
bringing older carers’ concerns into ongoing ToC work
exploring dedicated guidance and better mainstreaming within the ToC standards
sharing good practice on carer contingency planning in upcoming meetings
I also reiterated the group’s role in surfacing policy gaps and influencing future national lobbying.
6.4 Carer Registration & Meeting Access
Several carers raised issues with:
The length of the ToC sign-up form
Not receiving meeting links despite signing up
Verification barriers when joining Teams
Mary agreed to:
review and shorten the form
clarify which fields are optional
address email deliverability issues
adjust MS Teams settings to reduce joining friction while maintaining security
6.5 Concerns About Confidentiality Misuse
One carer reported that in a CQC meeting at an NHS Trust, raising questions about communication was dismissed as “confidentiality”, preventing meaningful dialogue. I then encouraged carers to bring such examples into:
ToC Star peer reviews
Carer involvement forums
Local advocacy routes
He noted that misuse of confidentiality is a common and unacceptable barrier and must be challenged.
6.6 Petition on Antipsychotic Medication Research
Carers highlighted concerns about:
long-term prescribing of antipsychotics
lack of regular medication review
inadequate research into long-term effects
A carer shared a petition calling for investigation of psychiatric medications. Richard noted that he had signed and shared it previously.
7. Closing Remarks
Matthew thanked all attendees for their honesty, passion and persistence:
“Carers’ voices shape policies and improve care. That is exactly what this group is here to do.”
Mary acknowledged:
the importance of every concern raised
the need to better support older carers
improvements to ToC communications and meeting accessibility
that the next meeting will be in January (provisionally 19th)
The meeting closed with gratitude from carers who said they felt heard, supported, and connected.
Walking into the RCN PSI Alumni Conference at Cowdray Hall on that crisp November morning, I felt a mix of pride, gratitude, and curiosity. It’s been many years since I first began speaking at RCN events like this, yet every time feels new because each gathering brings together nurses, carers, service users, and leaders who continue to shape the future of mental health care.
Before I continue to describe the event, let me sum up the Royal College of Nursing PSI programme. Basically the Psychosocial Interventions (PSI) programme is a nationally recognised training initiative designed to strengthen therapeutic skills of mental health professionals and embed recovery-focused, relationship-based care across services.
The PSI program is rooted in the principles of collaboration, reflection, co-production and empowerment, PSI equips practitioners with practical tools to support individuals experiencing mental distress, while also valuing the insight of carers and families.
I think what makes PSI stand out is its emphasis on seeing people beyond their diagnosis and fostering empathy, curiosity, and shared understanding between nurses, service users, and carers.
At the start of the conference and during it, I spoke to a few nurses over coffee, each reflecting on how PSI had shaped their practice one mental health nurse told me it had helped her “find her voice again.” For me, as a carer with lived experience, it was great to witness this sense of renewal. It reminded me why collaboration between professionals and lived experience communities is so essential.
Around 10 a.m., Catherine Gamble formally opened the event, setting a tone of gratitude and shared learning. Her introduction reminded us how much the alumni network had grown and how lived experience was now firmly part of the PSI culture.
As someone with lived experience of caring for my mum, who lived with schizophrenia, I approached the events not just as an observer but as someone deeply invested in the stories and struggles that bring us together as a triangle.
When I was invited to open the event and share my reflections as a carer, I knew I wanted to do more than talk about carers, I wanted to speak for them, and with them.
My Opening Talk – “The Nurses Who Walk With Us”
Standing at the podium, looking out at rows of passionate mental health nurses and lived experience, I began with gratitude. My words were simple but heartfelt:
“This is really about the nurses who walk with us, the ones who move beyond the labels, beyond the charts, and see the person, not the problem.”
I read a poem I had written to honour the compassion and resilience of those in the room a piece I called The Nurses Who Walk With Us.
The poem spoke about presence, about listening, and about the small acts of care that ripple into great change.
After my talk, I was moved by the warmth of the response. Many came up to share how my words mirrored their experiences or reminded them of why they came into nursing. That moment of connection that shared understanding set the tone for the day.
The Locksmiths Animation and Alumni Showcase
Following our opening session, Ellie Gordon and Stephen Jones launched the new animation “We Are the Locksmiths.” The film poetically portrayed mental health nurses as key-cutters shaping, adapting, and helping people find the right fit for recovery.
Watching it, I was struck by how accurately it captured the emotional labour of care, the balancing of vulnerability, patience, and professionalism
Next we had the Mentimeter session that morning, which was led by Professor Sally Hardy. She guided participants through reflective wellbeing questions using the interactive Mentimeter tool, encouraging everyone to think about how to sustain personal and professional wellbeing in mental health practice. Sally’s session wasn’t just about gathering feedback
Afterwards, the Alumni and Facilitators’ “Show and Tell Time” began. Groups from Sheffield NHS Trust, Sussex Mental Health Partnership, Lancashire Mental Health NHS trust, and Hereford NHS Trust sharing creative projects and reflections from their PSI practice. There were posters, poems, and community initiatives that had grown directly from the training. I wandered around the tables, speaking with participants who described how PSI had changed their teams. I think One mental health nurse told me, “We stopped seeing interventions as techniques and started seeing them as relationships.” It was inspiring
Workshop One – Working Together in Risk and Safety
After refreshments, we broke into workshops. I joined Workshop One: Lived Experience and Co-Production – Utilising Our Expertise, led by Hannah Cadogan and colleagues. It was energising to see lived experienced and mental health nurses working side by side.
I spoke about what co-production really means from a carer’s point of view. I shared my journey as someone who has cared for a family member living with schizophrenia and another with autism, and how those experiences taught me the importance of being included as an equal partner in care.
I explained that carers often hold a deep understanding of the person they support insights that can make a real difference if professionals take the time to listen and involve us from the start, not as an afterthought. Drawing on my work with Carers UK, the Carers Trust, and the Triangle of Care as many nurses from the mental health trusts were members of triangle of care programme., I spoke about how true co-production is built on trust, openness, and shared learning.
We discussed barriers time, fear, power differences but also solutions, like embedding co-production in supervision and reflective practice.
In this session, the discussion turned to how we can meaningfully involve carers and service users in planning safety not as tick-box exercises, but as genuine collaborations. I found myself reflecting on my own experiences of sitting in meetings where decisions were made about my mum rather than with us.
Hearing the nurses speak so openly about their challenges about time pressures, fear of getting it wrong, and the emotional toll of risk reminded me that we’re all human in this process. True co-production means sharing not only responsibility but also vulnerability.
One participant spoke about the importance of patience: “We’re not here to fix; we’re here to find a way in.” That line stayed with me. It echoed my own philosophy that care starts with listening, not solving.
By the end of the workshop, we agreed that co-produced safety isn’t about removing risk; it’s about building trust so we can face risk together.
Workshop Two – Co-Production and Carer Involvement
Lunch provided another opportunity for networking. The Mental Health Forum stand and MHP stall displayed resources on psychosocial practice.
I met others who had recently completed the course.
Conversations were open, curious, and full of mutual respect the kind of professional empathy that sustains hope in challenging work.
After lunch we heard from Professor Nicola Ranger, RCN General Secretary, who welcomed everyone back, commending the alumni for sustaining PSI’s legacy. Her words “you are the custodians of compassion” perfectly captured the spirit of the day.
The evaluation session of the RCN PSI Alumni Conference was presented in partnership with London South Bank University (LSBU), who have been key academic collaborators in examining the outcomes and long-term impact of the Psychosocial Interventions (PSI) programme. This section was introduced by Stephen Jones, and Professor Chris Flood, a leading figure in mental health nursing and research at LSBU.
Together, they outlined how LSBU’s evaluation seeks to capture not just the quantitative outcomes of PSI such as improved confidence and competence among practitioners but also the qualitative stories of change, growth, and compassion that the alumni community embodies.
There will be several teams at LSBU, but I was impressed on the make up of the Advisory and Supervisory Team provides academic oversight and strategic direction.
Professor Patrick Callaghan, Professor of Mental Health Science at LSBU, offers extensive expertise in psychosocial interventions and nursing research leadership.
Professor Chris Flood, a leading mental health and adult nurse researcher, specialises in health economics, survey design, and qualitative inquiry.
Professor Neil Brimblecombe, Professor of Mental Health and Learning Disability, contributes his expertise in workforce development, nurse prescribing, and policy analysis linking the PSI evaluation to broader NHS workforce strategies.
Professor Eddie Chaplin, an expert in intellectual disabilities and psychosocial interventions, supports the development of inclusive frameworks for peer support, guided self-help, and service co-production.
Afternoon workshop
In the afternoon, I attended Workshop Three: Working Together in Risk – Co-Production, Suicide and Personalised Safety. It was deeply emotional. We discussed how carers can be crucial in early warning and safety planning, but only if professionals create safe spaces for them to speak. The workshop was presented by Berkshire Healthcare NHS Foundation Trus
During the workshop, we took part in reflective exercises that encouraged us to consider what “shared safety” truly means. We were asked to think of times when communication broke down between families, patients and professionals, and how different outcomes might have been possible if trust and collaboration had been stronger.
Celebrating Archievements
Those who finished the RCN PSI programm were presented with a RCN PSI alumni badge, which i felt was a small but powerful symbol of commitment, compassion, and continued learning. For many, receiving that badge wasn’t just about completing a programme; it represented belonging to a network that values empathy, partnership, and the courage to keep improving mental health care together.
Reflections and Looking Ahead
As the day drew to a close, we took a quiet moment to reflect. Conferences like this are not just about learning they are about belonging. They remind me that, while the caring role can often feel isolating, there is a wider network of understanding and solidarity.
I missed out a lot more that took place at the alumni event, but watch out for more exciting news from the RCN in future.
To find out more about the RCN PSI Progamme, click link below.
The recent Carers Forum brought together unpaid carers, health professionals, and community organisations from across South London to share updates, experiences, and ideas for improving mental health support. The event, chaired by Matthew McKenzie, created a safe and open space for carers to connect, exchange information, and have their questions heard by local health leaders.
Setting the Scene
Matthew opened the session by welcoming carers from across Lambeth, Lewisham, and Southwark. He spoke about the importance of providing carers with dedicated time to hear from service providers, particularly those supporting someone with mental ill-health and to ensure their voices shape local mental health strategies.
As someone who’s been advocating for carers for years through A Caring Mind, I know how important it is that carers’ experiences influence the way support systems are built. The OSMOSIS project offers a real chance to help improve understanding and services for those of us supporting loved ones with severe mental health conditions.
If you are caring for someone living with psychosis, schizophrenia, or bipolar disorder, here’s an opportunity to make your voice heard.
By Matthew McKenzie FRSA BEM, Chair, Triangle of Care Community Group
This week’s Triangle of Care Member Webinar, hosted by Carers Trust, which focused on a vital question: What makes for meaningful carer involvement?
We heard from across the Triangle of Care network, these being carers, professionals, and trust representatives coming together to share what genuine involvement looks like in practice.
I spoke about my own lived experience as a carer, supporting two non-verbal brothers with autism and my late mother with mental health challenges and how this journey has shaped my advocacy for stronger partnerships between carers and professionals.
Over the years, through the Triangle of Care, I’ve seen how much difference early and equal involvement can make.
The meeting focused on introductions and updates from various organizations supporting unpaid carers across London. Matthew McKenzie facilitated the session, introducing participants from different boroughs and organizations, including
North Central London Carer Support Project (covering Barnet, Haringey, Camden, Enfield, and Islington)
The PSE (supporting South East London local authorities: Bexley, Bromley, Lambeth, Lewisham, Greenwich, and Southwark)
Richmond Borough Mind
Richmond Carers Centre
Kingston Carers Network
St George’s, Epsom and St Helier Hospital Group
Sutton Carers Centre
Carers Hub Lambeth (supporting unpaid carers, with hospital carers leads at King’s College Hospital and Guy’s & St Thomas’ Hospital)
Lewisham carers services (Imargo service manager)
Apologies from
Bromley Wells Bexley Carers Support Greenwich Carers Ealing Carers Partnership Tower Hamlets Carers Centre
NHS England updates including Universal Care Plan Updates
A representative from NHS England highlighted good news about the Hospital Discharge Toolkit, which had been originally developed in London by Debbie Hustings. The toolkit has already been adopted across much of southwest London with strong results. Recently, all NHS regions were asked to contribute work on hospital discharge, focusing particularly on carers’ experiences. When this went up to the Executive Quality Board at the national level, the London toolkit received recognition. The recommendation that came back was that all regions should develop something similar they could adopt London’s version directly or tailor one for their own needs. The representative stressed that this kind of recognition is significant because it helps the toolkit be taken more seriously and provides momentum for further rollout
On 21st of July 2025, carers, professionals, and stakeholders from across the UK gathered virtually for the latest Triangle of Care (ToC) Community Meeting. Chaired by Matthew McKenzie, this session was packed with insight, action points, and open dialogue. Whether you were new to the group or a long-time contributor, there was something valuable for everyone.
This meeting was particularly significant as it marked a turning point for carer participation. The formal recognition of the community group in ToC’s national governance structure. It affirmed that carer lived experience should not be sidelined, and that carers must continue to shape mental health services from the inside out.
If you weren’t able to attend, this blog will bring you up to speed. As the ToC community group covered a wide range of topics, from updates on national strategy and governance, to inclusive language, carer-led training, and advocacy for better research funding. At the heart of it all was a single message: when carers unite, systems must listen.
Official Recognition and Governance Progress
We are delighted to announce that the Triangle of Care Community Group is now formally integrated into the Triangle of Care governance structure. This gives the group a direct route to influence national decisions. The community will now sit alongside steering and regional groups in shaping policy, reviewing practices, and helping determine what carer inclusion should look like across all participating trusts.
What this means practically is improved alignment and visibility. For years, many carers and grassroots contributors have worked tirelessly behind the scenes, often without formal platforms. This change allows community voices to be heard before decisions are made not just consulted afterwards. Matthew described this shift as “a recognition of the years of unpaid care, leadership, and advocacy carers have always provided.”
It also means that our meetings will align with national timelines and decisions, ensuring a timely flow of updates between local groups, regional networks, and national forums. This is a pivotal opportunity to embed carers more meaningfully into NHS structures and accountability.
New Mailing List & Sign-Up System
Mary Patel from Carers Trust announced the launch of a new centralised mailing list for Triangle of Care community members. This will make sure everyone receives meeting invites, resources, and updates reliably. Participants will soon be asked to complete a Microsoft sign-up form, which will securely transfer contact details onto the Carers Trust system for ongoing communications.
The form will include a few demographic questions to help build a picture of the diversity within the ToC community. These questions are entirely optional but are designed to help Carers Trust identify who is engaging, and where gaps might exist—ensuring outreach strategies reflect real needs. For example, better regional balance, or increased visibility for underrepresented carer groups.
There was also discussion about moving from Zoom to Microsoft Teams for future meetings. Teams offers benefits like attendance tracking, secure file sharing, and easier scheduling. However, this won’t be a forced change, Matthew and Mary invited feedback, emphasising that any transition would be made collaboratively with community input.
Stronger Carer Involvement
Carer involvement was at the heart of the meeting. Matthew shared a passionate update on the need for carers particularly those from minority backgrounds or marginalised communities to step forward and engage in all aspects of the Triangle of Care. This includes involvement in peer reviews, shaping surveys, and suggesting new training or webinar content that reflects their lived experience.
The community was reminded that leading change doesn’t require a title or formal position. Sharing your story, participating in surveys, or simply raising your hand during a meeting is a form of leadership. Matthew emphasised that carers hold the kind of insight that no policy or textbook can replicate. As he put it, “This community is only as strong as the carers who show up.”
Peer reviewing was especially encouraged. Carers can play a vital role in reviewing mental health trust practices and making sure those trusts aren’t just ticking boxes but are genuinely improving the carer experience. Anyone interested in joining these review panels was invited to contact Mary Patel directly. The experience is meaningful and empowering and it places carers right where they should be: in positions of influence.
CQC Expectations and Carer Experiences
A powerful part of the meeting focused on the role of the Care Quality Commission (CQC) and how effectively it monitors carer inclusion in mental health services. Several carers and professionals shared their experiences some positive, others deeply concerning about how the CQC engages (or fails to engage) with carers during inspections.
A senior experience lead from an acute trust, explained that when CQC inspectors review services, they typically look for a clear carers policy, systems for identifying and supporting carers, and evidence of staff training. However, the level of scrutiny and the quality of carer-related feedback can vary significantly between inspections. The experience lead noted that while policy is important, it’s the systems around those policies that really matter, things like whether staff actually follow them, and whether carers know where to go for help.
Carers in the meeting shared contrasting experiences. A carer described a disappointing CQC visit where the inspector seemed dismissive, rushed, and uninformed about carers’ rights. Her feedback about lack of communication and exclusion was barely acknowledged, leaving her feeling invalidated. In contrast, Another carer spoke of a more recent inspection where the CQC officer seemed empathetic, asked thoughtful questions, and even disclosed their own possible caring experience. These differing accounts highlighted a common theme: carers’ confidence in the CQC is mixed, and their approach to carers can sometimes feel inconsistent.
There was strong consensus that CQC needs better training in carer engagement and not just understanding legal frameworks like the Care Act 2014, but also how to meaningfully include carers in service reviews. Kelvin added that cultural competence should also be part of the equation, noting that carers from minority backgrounds are too often left out of consultations. Matthew urged carers not to wait for trusts to invite them to speak during inspections ask to be involved, request to meet inspectors, and use carers’ councils or governors to raise visibility. It was clear from this session that carers want the CQC to be more than a compliance body, they want it to be a true advocate for accountability and equity in care.
Confidentiality Roadshow by Donna Bradford
A standout session was led by Donna Bradford, who presented her team’s work on the Confidentiality Roadshow a training programme developed by Lincolnshire Partnership NHS Foundation Trust. Designed to upskill staff on consent, confidentiality, and communication, the roadshow is tailored around carer inclusion and co-produced with the Carers Council.
The training helps staff understand not only what they can share legally, but also how to navigate nuanced emotional and ethical situations with carers. Donna reminded attendees that sharing basic, non-confidential information, such as medication side effects, is not only lawful but essential. “If you can Google it, you can say it,” she noted, driving home the importance of clarity over confusion.
Over 550 staff have already received the training, with 100% reporting that it improved their confidence. The programme includes real-life carer scenarios, emotional video testimonials, and interactive quizzes to help reinforce learning.
Beyond the training content itself, what makes the Confidentiality Roadshow so impactful is its co-production with carers. Donna highlighted that every scenario used in the sessions came from real-life examples shared by carers and families. This ensures the training isn’t theoretical so it’s grounded in lived experience. The emotional and practical realities of caring for someone with mental health needs are at the heart of the learning, helping staff understand why clear, compassionate communication is so essential. The training also underscores the importance of listening to carers, not just as bystanders but as active contributors to a person’s care journey.
Several attendees raised the idea of incorporating this training into broader staff induction and continuing professional development programmes. Others asked about adapting it for use in different trust settings, such as acute hospitals or community services. Donna encouraged trusts to reach out if they’d like to adopt or customise the resource. The message was clear: confidentiality shouldn’t be a barrier, it should be a bridge, and with the right training and tools, staff can navigate those conversations with confidence, legality, and humanity.
Mental Health Research Petition
Irene Harris spoke passionately about a new parliamentary petition calling for improved research funding into serious mental illnesses (SMIs) like psychosis. The petition aims to shine a spotlight on how outdated treatments and under-researched conditions continue to place carers and their loved ones in difficult, often heartbreaking positions.
Here is the video about Psychosis medication and its impact by the Stockport carers forum.
She shared how mental health medications for SMIs haven’t evolved as rapidly as physical health treatments, and how this results in long-term side effects and compromised quality of life. Research is desperately needed, not only to improve diagnosis and treatment, but also to create support structures that ease the burden on unpaid carers.
Irene asked attendees to sign and circulate the petition widely, with a goal of hitting 10,000 signatures by November 15th.
She also announced plans to launch new social media channels to raise awareness. This initiative is about more than funding it’s about giving carers and service users a louder voice in national healthcare priorities.
or contact Irene on irene@mhcarersgroupstockport.co.uk
Language, Inclusivity, PCREF & the ‘Global Majority’ Debate
Language and inclusivity were major themes of the meeting, particularly around the term “global majority.” Some attendees expressed concern that the phrase could be divisive or misinterpreted, particularly by politically sensitive audiences or media outlets. A carer shared a personal anecdote illustrating how words can carry unintended consequences.
Others responded by highlighting the intention behind the term to emphasise that those historically described as “minorities” are, in fact, the global majority in population terms. They called for continued use of the phrase in contexts that promote empowerment, equity, and lived experience.
The discussion didn’t produce a consensus, but it modelled what respectful disagreement and co-learning should look like. Matthew reinforced that ToC should be a space for constructive dialogue, not debate for its own sake. Ultimately, we are united in our aim to ensure no carer is left behind regardless of background, heritage, or identity.
Next Steps & Community Actions
The session wrapped up with a summary of action points and responsibilities. Carers Trust will soon circulate the new mailing list sign-up form. Matthew will share updated meeting dates for 2026 once confirmed, and he will continue to distribute posters for the upcoming National Ethnic Carers Group, taking place on the last Friday of each month.
There will be support the rollout of the Confidentiality Roadshow materials and follow up with those interested in joining peer review panels. A reminder was issued for everyone to contribute to current surveys, share their feedback, and suggest future topics for community meetings.
Finally, participants were encouraged to stay connected beyond the meetings. Whether through peer networks, local carers centres, or email updates, the message was clear: carers must stay visible, vocal, and valued. You are the change-makers, and this group is your platform.
Final Thoughts: “Carers Are Not Just a Cog in the Wheel”
Matthew ended the session with a rallying call to action: “We’re not just a cog in the wheel as we are the energy behind it.” His words served as a reminder that carers are not passive recipients of services. They are drivers of quality, advocates for change, and protectors of dignity in the mental health system.
He also reminded everyone that systems often change slowly, but they do change when people keep showing up, keep speaking up, and keep sharing their truths. “This isn’t just about the Triangle of Care,” he said. “It’s about reshaping the whole narrative around mental health and care.”
If you missed the meeting and would like to receive the slides, recordings, or further resources, feel free to contact Matthew McKenzie directly: 📧 mmckenzie@carers.org
Thanks to to all who attended, contributed, and championed carers’ voices. The next meeting should in September where we hope to see you there.
The meeting focused on carer involvement and representation across different regions, with participants discussing their roles in supporting carers and addressing discrimination. The main focus for this meeting was on “What does good look like?” when it comes to Triangle of Care and PCREF.
The group explored the Triangle of Care initiative and its five key elements, including discussions about medication-related challenges and the need for better communication between healthcare providers and carers. The conversation ended with conversations about improving carer support systems, including the importance of advocacy, training, and creating safe spaces for carers to share concerns confidentially.